

Comprehensive cancer surveillance is necessary for establishing and monitoring effective cancer prevention and control programs and policies. Cancer occurrence data also inform governmental planning for national and local healthcare system resources. The steady increase in the establishment of population-based cancer registries internationally, despite challenging obstacles, is a testament to the value of data on cancer incidence and mortality.
Cancer is a major public health challenge in China. China’s population of 1.36 billion people represents almost 20% of the world’s population—more than the combined populations of North and South America, Western Europe, Russia, Australia, and New Zealand. The rapid urbanization and increased prosperity in China has led to a decline in infectious diseases and an increase in chronic diseases like cancer. In this issue of ATM, Chen et al. (1) provide a comprehensive report on the expansion of cancer registration in China, data quality indicators, the estimated national cancer burden, and age-standardized incidence and mortality rates stratified by urban or rural residence, geographic area, and age. In 2010, 3.1 million new cancer cases and close to 2 million cancer deaths occurred in China. According to GLOBOCAN data, these figures are expected to rise to 5.5 million new cases and 4.3 million deaths in 2035 (2).
Lung cancer was the most common cause of cancer in men, the second most common in women, and the leading cause of cancer in death in both men and women. The large lung cancer burden reflects the high prevalence of three major risk factors—tobacco, and both indoor and outdoor air pollution. China’s 300 million smokers (3) consumed more than 38% of the world’s cigarettes in 2009—more than the other top four tobacco-consuming countries combined. China is also the top tobacco producer, growing 43% of the world’s tobacco, more than the next nine tobacco-producing countries combined (4). Although China became a Party to the WHO Framework Convention on Tobacco Control (FCTC) (5) in 2005, the government’s implementation of tobacco-control policies as obligated by the treaty has been limited (6), partly due to a conflict of interest. The Chinese Ministry of Industry and Information Technology has led the implementation of the FCTC, while also being responsible for the China National Tobacco Corporation (7). Yet, some places in China, such as Hong Kong, have succeeded in implementing strong tobacco control policies that are supported by the local population and could serve as a model for other localities (8).
Another risk factor for lung cancer is indoor emissions from household combustion of coal and probably also biomass fuel (primarily wood), according to the International Agency for research on Cancer (IARC) (9). Despite rapid urbanization and increased use of gas and electricity for cooking and heating, the majority of China’s population remains dependent on solid fuels for household energy, resulting in potentially high levels of concentrated indoor pollutants. The concentrations of these particles can often exceed ambient air quality guidelines several times over. The Chinese population further suffers from exposure to chronic outdoor air pollution and particulate matter, both also classified as carcinogenic by IARC. The air pollution levels in Chinese cities are among the highest observed in the world today and frequently exceed health-based national and international guidelines (10).
Breast cancer is the most frequent cancer among women in China, as it is now throughout most of the world. China’s exploding economy has spurred lifestyle changes associated with westernization, such as delayed childbirth, that contribute to increasing breast cancer incidence. Currently, there is no nationwide systematic screening program for breast cancer in China despite national guidelines recommending mammography annually for women 40-49 years and every 1-2 years for women 50-69 years (11). Obstacles to establishing screening programs include insufficient cost-effectiveness data for Chinese women (particularly given the low incidence rate compared to most developed populations), the size and wide-spread geographic distribution of the population, insufficient mammography equipment, and inadequate insurance coverage. In addition, cultural barriers like cancer fatalism may hinder screening efforts, particularly in older and lower socioeconomic status women (11). Nevertheless, some areas have introduced mammography screening programs. For example, Taiwan has provided government-sponsored screening for women 45-69 years since 2009, adding coverage for high-risk women aged 40-44 years in 2010. In 2012, 33% of women aged 45-69 had had a mammogram within the past 2 years compared to 19% of Chinese women 40-69 years nationally (12).
Alcohol is a risk factor for cancers of the upper aerodigestive tract, liver, colon-rectum, and breast. According to data provided by the WHO Global Information System on Alcohol and Health (13), sharp increases in annual per capita alcohol consumption have occurred in China since the 1980s, up to a total average of 10.9 and 2.2 liters of pure alcohol consumed by men and women (aged 15+), respectively, in 2008-2010. In 2010, percentages of abstainers (aged 15+) over the past 12 months were 42% in men and 71% in women. The higher consumption in men may contribute to the disproportionately high rates of liver cancer in men (32.2 per 100,000 in men versus 10.4 in women). China’s policies on the sale and consumption of alcoholic beverages are lax compared with those of other countries in Asia. Weakest of all are its policies on drink driving laws, marketing licenses, taxation and alcohol sale to minors. For instance, regulations on the administration of alcohol sales issued by China’s Ministry of Commerce went into effect in 2006. Their purpose was to ban the sale of alcoholic beverages to minors, but the penalties for violations are not specified (14).
Implementing community-based cancer awareness programs is feasible, locally affordable and sustainable in low-income settings as proven in Kashi (Kashgar) Prefecture, Xinjiang, China (15). Still, provision of universal access to health care insurance is essential for people to be able to afford screening programs, cancer diagnosis and treatment. Promising reform to establish universal coverage that would provide “safe, effective, convenient, and affordable basic health services” to all urban and rural residents in the next decade was announced by China’s government in 2009 (16).
The implementation of new cancer registries in China will allow for the measurement of progress in cancer control, such as the effect of health protection policies, primary prevention, population awareness, and increased access to early detection, diagnosis and treatment. It is all the more important that China is going through major demographic and economic changes. The number of adults aged 65+ will more than triple between 2000 and 2050, going from less than 100 million to more than 300 million (Figure 1). In 2010, the incidence rate for this age group was over 900 per 100,000 (1). China’s rapid urbanization and adoption of a westernized lifestyle (e.g., more sedentary, consumption of more meat and fewer vegetables, and a higher prevalence of obesity), in combination with high rates of tobacco use, is reflected in the changing cancer landscape. Declines in cancers related to infectious agents, such as cervix, liver, and stomach, depending on the extension of known effective interventions such as cervical screening and HPV vaccine, hepatitis vaccination, and Helicobacter pylori treatment, respectively, may be counterbalanced by increases in lung, breast and colorectal cancers common in high-income countries (17). Cancer-registry data are used to monitor screening program by observing the proportion of patients detected by screening and shifts in stage distribution (18). As new cancer registries have been established in both rural and urban settings, comparing the cancer patterns in both areas will allow tailoring area-specific primary-prevention campaigns and healthcare policies. For instance, in 2010, in all age groups between 15 and 70 years old, mortality rates were higher in rural areas than in urban areas. With more than 250 cancer registries covering more than 200 million Chinese people, the cancer registration program might detect areas with very high cancer incidence caused by marked exposure to some carcinogens. Thus far, most cancer research has been performed in high-income countries and some findings may not apply universally—such as the recommended age and interval for breast cancer mammography (11), due to genetic, environmental, and healthcare differences. Additionally, some of the Chinese population is susceptible to some cancers that are considered rare in high-income countries, such as nasopharyngeal cancer (19). Expanded cancer registration also opens the door to new opportunities for surveillance research on cancer.
Figure 1.
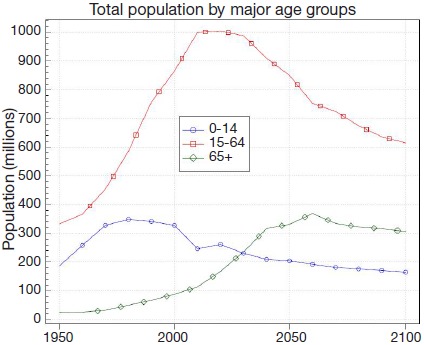
Trends in population, by age group, in China, from 1950 to 2100. Source: United Nations, Department of Economic and Social Affairs, Population Division (2013). World Population Prospects: The 2012 Revision, Volume II: Demographic Profiles. ST/ESA/SER.A/345. Published with the permission of the United Nations, Department of Economic and Social Affairs, Population Division.
Some cancer registries started a long time ago in China—such as in Shanghai, Tianjin and Qidong County—and have been chosen in several instances for publication in Cancer Incidence in Five Continents (CI5) (since 1975 for Shanghai, from 1981 to 1997 for Tianjin and from 1983 to 1997 and 2003-2007 for Qidong County) (20). The fact that 14 cancer registries (twelve mainland, plus Hong Kong and Macao) have been accepted in the latest volume of CI5 is indicative of each registry’s high data quality given the very discriminating selection process. This is more regional registries than were accepted for any other country in the area (twelve in India, nine in Republic of Korea, eight in Japan, six in Thailand, two in Philippines, and one in Russian Federation). Other countries in the area, aided by the Global Initiative for Cancer Registry Development (GICR) (http://gicr.iarc.fr/), are developing a population-based cancer registration system, such as Mongolia, Sri Lanka and Indonesia. China, along with the GICR regional hub for South, South-East, and East Asia based at Tata Memorial Centre in Mumbai (India), can be a model for cancer registration.
The successes of the recent expansion of population-based cancer registration in China are already measurable in the 2010 report. The results represent the best data currently available, and provide a sound appraisal of cancer occurrence in China. With the number of annual cancer cases and deaths likely to increase by at least 60% by 2030 (2) based solely on population aging and growth, there is a pressing need for surveillance systems to facilitate a coordinated approach to improving the extent and quality of cancer control in China.
Acknowledgments
Disclosure: The authors declare no conflict of interest.
References
- 1.Chen W, Zheng R, Zhang S, et al. Report of cancer incidence and mortality in China. Ann Transl Med 2014;2:61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 Lyon, France: International Agency for Research on Cancer; 2013. Available online: http://globocan.iarc.fr
- 3.Public smoking regulation in China: no more hot air. Lancet 2014;383:100. [DOI] [PubMed] [Google Scholar]
- 4.Eriksen M, Mackay J, Ross H. The Tobacco Atlas. Fourth ed. Atlanta, GA: American Cancer Society; New York, NY: World Lung Foundation; 2012. [Google Scholar]
- 5.WHO Framework Convention on Tobacco Control, 2003. Available online: http://www.who.int/fctc/en/
- 6.Samet JM. Invited commentary: the challenge of tobacco control in China. Am J Epidemiol 2014;179:1071-3. [DOI] [PubMed] [Google Scholar]
- 7.Wan X, Ma S, Hoek J, et al. Conflict of interest and FCTC implementation in China. Tob Control 2012;21:412-5. [DOI] [PubMed] [Google Scholar]
- 8.Wang MP, Wang X, Lam TH, et al. The tobacco endgame in Hong Kong: public support for a total ban on tobacco sales. Tob Control 2013. [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 9.IARC. Household use of solid fuels and high-temperature frying. Lyon: International Agency for Research on Cancer; 2010. Available online: http://monographs.iarc.fr/ENG/Monographs/vol95/mono95.pdf
- 10.Loomis D, Huang W, Chen G.The International Agency for Research on Cancer (IARC) evaluation of the carcinogenicity of outdoor air pollution: focus on China. Chin J Cancer 2014;33:189-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Fan L, Strasser-Weippl K, Li JJ, et al. Breast cancer in China. Lancet Oncol 2014;15:e279-89. [DOI] [PubMed] [Google Scholar]
- 12.Health Promotion Administration MoHaW, R.O.C. 2013 Health Promotion Administration Annual report. Promoting your health. Taiwan: 2013. Available online: http://health99.hpa.gov.tw/media/public/pdf/21759.pdf
- 13.World Health Organization. Global Information System on Alcohol and Health (GISAH). 2014. Available online: http://www.who.int/gho/alcohol/en/
- 14.Tang YL, Xiang XJ, Wang XY, et al. Alcohol and alcohol-related harm in China: policy changes needed. Bull World Health Organ 2013;91:270-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Simayi D, Yang L, Li F, et al. Implementing a cervical cancer awareness program in low- income settings in Western China: a community-based locally affordable intervention for risk reduction. Asian Pac J Cancer Prev 2013;14:7459-66. [DOI] [PubMed] [Google Scholar]
- 16.Meng QT, Tang S. Universal Coverage of Health Care in China: Challenges and Opportunities. WHO Geneva, Switzerland: 2010. Available online: http://www.who.int/healthsystems/topics/financing/healthreport/7ChinaM_T.pdf
- 17.McCormack VA, Boffetta P. Today’s lifestyles, tomorrow’s cancers: trends in lifestyle risk factors for cancer in low- and middle-income countries. Ann Oncol 2011;22:2349-57. [DOI] [PubMed] [Google Scholar]
- 18.Brewster DH, Coebergh JW, Storm HH. Population-based cancer registries: the invisible key to cancer control. Lancet Oncol 2005;6:193-5. [DOI] [PubMed] [Google Scholar]
- 19.Cao SM, Simons MJ, Qian CN. The prevalence and prevention of nasopharyngeal carcinoma in China. Chin J Cancer 2011;30:114-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Forman D, Bray F, Brewster DH, et al. eds. Cancer Incidence in Five Continents, Vol. X (electronic version) Lyon, IARC. Available online: http://ci5.iarc.fr