

Abstract
Background:
Stones in the urinary system are common in our country. This study was done to assess the composition of the urinary stones in eastern part of India.
Materials and Methods:
A prospective study was done over a period of thirty months. A total of 90 stones were analyzed in this time period by using X-ray diffraction crystallography.
Results:
Of the 90 stones analyzed, 77 were renal stones, 12 were ureteric stones and one was a bladder stone. Six stones (all renal) did not have properties to be represented by X-ray diffraction crystallography. The overall prevalence of the oxalate containing stones was 85.7% with calcium oxalate monohydrate (COM) being the major constituent. Calcium oxalate dihydrate (COD) was the next most common constituent. Struvite stones constituted 9.5% of the stones analyzed. Pure calcium phosphate stones were found in 4.7% of the cases.
Conclusion:
Our study reveals that the stone composition in the eastern part of India is different from that in other parts of the country. We have a comparatively lower prevalence of oxalate stones while a higher prevalence of phosphate and struvite stones.
Keywords: India, renal stones, stones, stone analysis
INTRODUCTION
Urinary stones have afflicted humankind since antiquity. The overall prevalence of urinary tract stone disease is estimated to be between 2% and 10%.[1,2,3] Urolithiasis is an entity which has high morbidity and socio-economic impact. The advent of extra corporeal techniques for stone destruction and the refinements in the endoscopic surgery have greatly decreased the morbidity associated with stone surgery, and the disorder is changing from a major health problem to a major nuisance.[4,5,6] Unfortunately, these interventions can treat stones but do not prevent them; however, as anyone who has passed a stone can tell that prevention of recurrence is what the majority of the patients with stone disease need. The holistic management of stone disease is deemed incomplete if prevention is not given its due importance.
Stone composition has a great role in selecting the modality of treatment to be offered as well as in providing the clinician the information with which he may help the patient in avoiding stone formation.[7,8] India is the second most populous country in the world. The incidence of stone disease in various parts of the country logically varies due to the differences in climate, dietary habits, quality of ground water etc. We, in this study, utilized X-ray diffraction crystallography to assess the composition of stones in West Bengal. We also compared our results with other major studies to assess whether the stone composition is any different in this belt.
MATERIALS AND METHODS
This was a prospective observational study. Ethical clearance was obtained. The study period was from September 2008 to March 2011. All the patients who were admitted in the Department of Urology at the Calcutta National Medical College with a diagnosis of a stone in the urinary system and those who consented for the study were included in the study. As children (less than 14 years, as per our protocol) can have a different stone composition, they were not included in the study. All the patients underwent thorough clinical examinations, routine hematological and biochemical investigations, urine examination including culture and sensitivity. The patients who had any abnormality in the above mentioned examinations or did not give their consent or had a personal or family history of recurrent stone formation or any intervention done previously for stone disease in the past were excluded from the study. The treatment offered was decided by a single clinician depending upon the site of the stone and the size of the stone.
Stones were collected after the following interventions: Open operations (n = 6), extra corporeal shock wave lithotripsy (ESWL) (n = 15) and percutaneous nephrolithotomy (n = 69). A total of 90 stones were analyzed in this time period. The actual number of patients treated by ESWL was quiet high but only those patients who could retrieve a stone from their urine after the procedure could be included in the study. Only one stone was taken from one patient. X-ray diffraction crystallography was used to assess the stone composition.
X-ray diffraction crystallography is a technique in which X-rays are used, which undergo diffraction when subjected to closely spaced atoms in a crystal. The patterns produced by this are then analyzed to reveal the nature of the crystal lattice. This technique has been widely used in determining the structure of DNA, proteins etc. It has also been used in analyzing the composition of urinary tract calculi. Various techniques have been used for analysis of stones, which include chemical analysis, polarization microscopy, infra-red spectroscopy, thermo-gravimetry, scanning electron microscopy etc. It has been found that X-ray diffraction crystallography and infra red spectroscopy are the most reliable methods for stone analysis. The advantage of X-ray diffraction crystallography is that it is less labor intensive and more reliable as compared to infra red spectroscopy. The disadvantages are high cost, inability to analyze amorphous substances and lack of availability.[9]
RESULTS
A total of 90 stones were analyzed. The mean age of the patients was 38 years (range 22 to 65 years). There were 51 males and 39 females. The mean age of males was 37.5 years while that of females was 38.7 years. All the patients were from West Bengal. Of the stones analyzed, 77 were renal stones, 12 were ureteric stones and one was a bladder stone. Six stones (all renal) did not have properties to be represented by X-ray diffraction crystallography and hence, could not be analyzed. The overall patterns of stone composition observed in the study are summarized in Table 1. The patterns of different stones on X-ray diffraction crystallography have been shown in the Figures 1–6.
Table 1.
Overall stone composition (n=84)
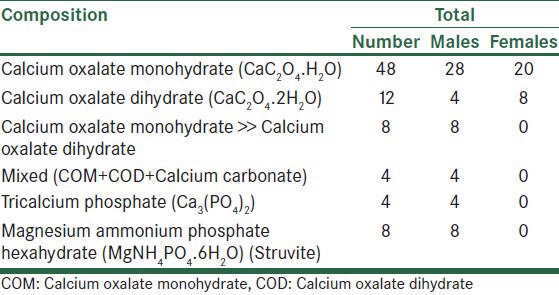
Figure 1.
X-ray diffraction crystallography pattern of calcium oxalate monohydrate
Figure 6.
X-ray diffraction crystallography pattern of stones composed of magnesium ammonium phosphate hexahydrate
Figure 2.
X-ray diffraction crystallography pattern of calcium oxalate dihydrate
Figure 3.
X-ray diffraction crystallography pattern of stones having calcium oxalate monohydrate>> calcium oxalate dihydrate
Figure 4.
X-ray diffraction crystallography pattern of mixed stones
Figure 5.
X-ray diffraction crystallography pattern of calcium phosphate stones
Out of the 71 renal stones that could be analyzed, 39 were composed of pure calcium oxalate monohydrate (COM), 12 were pure calcium oxalate dihydrate (COD) stones, four had COM>>COD, four were mixed stones (varying ratios of COM, COD and calcium carbonate), four had calcium phosphate while eight were composed of magnesium ammonium phosphate hexahydrate (MAP). Of the 12 ureteric stones, eight were pure calcium oxalate monohydrate (COM) stones and four were COM>>COD stones. The bladder stone was composed of COM. In our study there were eight staghorn stones. Of these stones, six stones were composed of COM and COD, one had MAP while one had properties which could not be represented by X-ray diffraction crystallography. There were no uric acid stones or cystine stones.
DISCUSSION
Assessment of stone composition is an important aspect in providing a holistic treatment to the patients. It can provide an insight into the reason of the stone formation thus allowing the physician to intervene in order to prevent recurrence. The stone composition can also be an important factor in deciding the modality of the treatment offered to the patients.[7,8]
The stone compositions vary in different populations and are dependent on various factors like geographic location, environmental conditions, dietary patterns, socioeconomic status, water quality etc. The stone composition in our country is different from the rest of the world. In the Western literature, the overall prevalence of oxalate stones (COM or COD) has been variously quoted to be between 30 and 66%.[10,11,12,13] The analysis of Indian literature suggests that the prevalence of oxalate stones is much higher as compared to the West, about 90-97% as per the various studies. Most of these studies have been performed in the Northern population.[7,14,15,16,17,18] Ahlawat et al. reported that 97% of the stones in their study population had oxalate of which 90% had COM and 4.6% had COD as the major constituent while 5.5% were mixture of COM and COD.[14] Ansari et al. reported that 93.04% of their study group had oxalate calculi out of which 80% had COM, 20% had COD.[15] In our study, the overall prevalence of the oxalate containing stones was 85.7%. COM was the predominant constituent in our study population. Pure COM stones were present in 57.1%. COD was the next commonest constituent. Pure COD stones were present in 14.3%. Thus, the prevalence of oxalate stones in our study shows a striking contrast as compared to those in the Northern population. Struvite stones constituted 9.5% of the stones. Four pure calcium phosphate stones were found. This too is significantly different from the contemporary Indian literature, which reveals a low prevalence of both the varieties of stones in the northern population.[7,14,15] On the other hand, a study done in Manipur (a state in the eastern part of the country) found high prevalence of phosphate stones in their study group. This may indicate that the eastern belt of the country is more prone to have phosphate calculi.[19] In our study, majority of the staghorn calculi were made of oxalate instead of struvite which is more common in the western literature. This pattern has also been observed in other Indian studies and implies that any calculi may become a staghorn if it continues to grow.[15] It may also be of interest to note that MAP was present in seven stones that did not have a staghorn configuration.
Our study is not free of limitations. Firstly, the number of patients in our study is small and a larger study may be necessary to get the true picture of the stone composition in this belt. We did not stratify our results on the basis of the body mass index, residence of the patient, the occupation of the patient, dietary habits, socio-economic status, etc., which can have implications upon the stone composition.[20] Another issue is that this study was done in a hospital setting. Hospital attendance depends upon various factors and is prone to “Berksonian bias” and it may not be reflective of the true nature of stone composition in the population.[21]
CONCLUSION
Our study highlights the difference in the stone composition in Eastern India as compared to the northern parts of the country. We have a comparatively lower prevalence of oxalate stones while a higher prevalence of phosphate and struvite stones. One should keep in mid these regional variations in stone compositions while deciding the treatment modality for the patients.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Delvecchio FC, Preminger GM. Medical management of stone disease. Curr Opin Urol. 2003;13:229–33. doi: 10.1097/00042307-200305000-00011. [DOI] [PubMed] [Google Scholar]
- 2.Lee YH, Huang WC, Tsai JY, Lu CM, Chen WC, Lee MH, et al. Epidemiological studies on the prevalence of upper urinary calculi in Taiwan. Urol Int. 2002;68:172–7. doi: 10.1159/000048445. [DOI] [PubMed] [Google Scholar]
- 3.el-Reshaid K, Mughal H, Kapoor M. Epidemiological profile, mineral metabolic pattern and crystallographic analysis of urolithiasis in Kuwait. Eur J Epidemiol. 1997;13:229–34. doi: 10.1023/a:1007346727944. [DOI] [PubMed] [Google Scholar]
- 4.Yuhico MP, Ko R. The current status of percutaneous nephrolithotomy in the management of kidney stones. Minerva Urol Nefrol. 2008;60:159–75. [PubMed] [Google Scholar]
- 5.Hall PM. Nephrolithiasis: Treatment, causes, and prevention. Cleve Clin J Med. 2009;76:583–91. doi: 10.3949/ccjm.76a.09043. [DOI] [PubMed] [Google Scholar]
- 6.Wignall GR, Canales BK, Denstedt JD, Monga M. Minimally invasive approaches to upper urinary tract urolithiasis. Urol Clin North Am. 2008;35:441–54. doi: 10.1016/j.ucl.2008.05.004. [DOI] [PubMed] [Google Scholar]
- 7.Singh I, Gupta NP, Hemal AK, Dogra PN, Ansari MS, Seth A, et al. Impact of power index, hydroureteronephrosis, stone size, and composition on the efficacy of in situ boosted ESWL for primary proximal ureteral calculi. Urology. 2001;58:16–22. doi: 10.1016/s0090-4295(01)01088-3. [DOI] [PubMed] [Google Scholar]
- 8.Seitz C, Tanovic E, Kikic Z, Fajkovic H. Impact of stone size, location, composition, impaction, and hydronephrosis on the efficacy of holmium: YAG-laser ureterolithotripsy. Eur Urol. 2007;52:1751–7. doi: 10.1016/j.eururo.2007.04.029. [DOI] [PubMed] [Google Scholar]
- 9.Basiri A, Taheri M, Taheri F. What is the state of the stone analysis techniques in urolithiasis? Urol J. 2012;9:445–54. [PubMed] [Google Scholar]
- 10.Daudon M, Donsimoni R, Hennequin C, Fellahi S, Le Moel G, Paris M, et al. Sex- and age-related composition of 10 617 calculi analyzed by infrared spectroscopy. Urol Res. 1995;23:319–26. doi: 10.1007/BF00300021. [DOI] [PubMed] [Google Scholar]
- 11.Smith LH. The medical aspects of urolithiasis: An overview. J Urol. 1989;141:707–10. doi: 10.1016/s0022-5347(17)40990-6. [DOI] [PubMed] [Google Scholar]
- 12.Choo-Kang E. Chemical composition of urinary tract stones at the University Hospital of the West Indies. West Indian Med J. 2008;57:427–30. [PubMed] [Google Scholar]
- 13.Mandel NS, Mandel GS. Urinary tract stone disease in the United States veteran population. II. Geographical analysis of variations in composition. J Urol. 1989;142:1516–21. doi: 10.1016/s0022-5347(17)39145-0. [DOI] [PubMed] [Google Scholar]
- 14.Ahlawat R, Goel MC, Elhence A. Upper urinary tract stone analysis using X-ray diffraction: Results from a tertiary referral centre in northern India. Natl Med J India. 1996;9:10–2. [PubMed] [Google Scholar]
- 15.Ansari MS, Gupta NP, Hemal AK, Dogra PN, Seth A, Aron M, et al. Spectrum of stone composition: Structural analysis of 1050 upper urinary tract calculi from northern India. Int J Urol. 2005;12:12–6. doi: 10.1111/j.1442-2042.2004.00990.x. [DOI] [PubMed] [Google Scholar]
- 16.Rao BN, Gupta HN, Rangnekar GV. Chemical composition of urinary calculi. A study of 225 cases. J Indian Med Assoc. 1964;43:469–71. [PubMed] [Google Scholar]
- 17.Pundir CS, Goyal L, Thakur M, Kuchhal NK, Bhargava AK, Yadav SP. Chemical analysis of urinary calculi in Haryana. Indian J Med Sci. 1998;52:16–21. [PubMed] [Google Scholar]
- 18.Rao MV, Agarwal JS, Taneja OP. Studies in urolithiasis: II. X-ray diffraction analysis of calculi from Delhi region. Indian J Med Res. 1976;64:102–7. [PubMed] [Google Scholar]
- 19.Singh PP, Singh LB, Prasad SN, Singh MG. Urolithiasis in Manipur (north eastern region of India). Incidence and chemical composition of stones. Am J Clin Nutr. 1978;31:1519–25. doi: 10.1093/ajcn/31.9.1519. [DOI] [PubMed] [Google Scholar]
- 20.Curhan GC. Epidemiology of stone disease. Urol Clin North Am. 2007;34:287–93. doi: 10.1016/j.ucl.2007.04.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Westreich D. Berkson's bias, selection bias, and missing data. Epidemiology. 2012;23:159–64. doi: 10.1097/EDE.0b013e31823b6296. [DOI] [PMC free article] [PubMed] [Google Scholar]