

Abstract
Background: Precursor B acute lymphoblastic leukemia (B-ALL) is the most common cancer in children and overall, has an excellent prognosis. However, the Philadelphia chromosome translocation (Ph+), t(9;22)(q34;q11), is present in a small subset of patients and confers poor outcomes. CD25 (IL-2 receptor alpha chain) expression has been associated with Ph+ B-ALL in adults, but no similar study has been performed in pediatric B-ALL. Methods: A retrospective analysis of 221 consecutive pediatric patients with a diagnosis of B-ALL (blood and/or bone marrow) from 2009 to 2012 was performed to determine an association between Ph+ B-ALL and CD25 expression. A threshold of 25% was used to define positive cases for CD25 expression by flow cytometry. Results: There were 221 patients with a diagnosis of B-ALL ranging from 2 to 22 years (median, 6 years). Eight (3.6%) B-ALL patients were positive for the Philadelphia chromosome translocation (Ph+ B-ALL) and 213 were negative (Ph-negative B-ALL). CD25 expression was observed in 6 of 8 (75%) Ph+ B-ALL patients and 6 of 213 (2.8%) Ph-negative B-ALL patients. CD25 expression was significantly higher in Ph+ B-ALL compared to Ph-negative B-ALL, with median CD25 expression of 64% (range 0-93%) and 0.1% (range 0-91%), respectively (P ≤ 0.0002). Therefore, CD25 expression as a predictor of Ph+ B-ALL had 75% sensitivity, 97% specificity, 50% positive predictive value and 99% negative predictive value. Conclusions: CD25 expression is a specific and relatively sensitive marker for the identification of Ph+ B-ALL in the pediatric population.
Keywords: CD25, BCR-ABL, Philadelphia chromosome, Ph+, t(9;22), B acute lymphoblastic leukemia, B-ALL, Ph+ B-ALL, flow cytometry, pediatric
Introduction
Precursor-B-acute lymphoblastic leukemia (B-ALL) is the most common cancer in children [1]. Overall, childhood B-ALL has an excellent prognosis, with complete remission achieved in over 95% and long-term event-free survival of approximately 85% [2-7]. The Philadelphia chromosome (Ph+) or BCR-ABL1 fusion gene is the result of a t(9;22)(q34;q11) translocation and is present in 20-30% of adults with B-ALL but only in 3-5% of childhood B-ALL [8-10]. Both pediatric and adult Ph+ B-ALL patients are more difficult to treat with higher rates of relapse and worse overall survival [10-12]. Early identification of Ph+ B-ALL is important for early initiation of a tyrosine kinase inhibitor in combination with conventional chemotherapy.
Expression of CD25 (interleukin-2 receptor alpha chain) by flow cytometric analysis has been shown to have an association with Ph+ B-ALL in adult leukemia studies [13-15], suggesting that CD25 could be used as a surrogate marker for adult Ph+ B-ALL. However, no such study has been conducted in pediatric B-ALL.
Materials and methods
The study was approved by the Institutional Review Board of Baylor College of Medicine, Houston, Texas. A retrospective analysis of consecutive patients at Texas Children’s Hospital with a new diagnosis of B-ALL over a three-year period (May 2009 to June 2012) was performed. The diagnosis of B-ALL was made based on criteria published by the World Health Organization 2008 [16]. Flow cytometric, cytogenetic, and FISH analyses were performed in all cases. Corresponding results of RT-PCR analysis of BCR-ABL1 transcripts were collected from medical records if available. Cases of infantile B-ALL (≤ 1 year) were excluded from analysis. Of note, all seven cases of infantile B-ALL had MLL gene rearrangement by FISH analysis.
Multi-parametric flow cytometry
A six-color multi-parametric flow cytometric analysis was performed on fresh cells according to standard protocol. The panel of 33 antibodies was performed using combination of FIT-C/PE/PerCP-Cy5.5/PE-Cy7/APC/APC-H7 as follows: CD7/CD2/CD3/CD8/CD4/CD45, Lambda/Kappa/CD19/CD10/CD5/CD45, CD15/CD42+61/CD34/CD38/CD11b/CD45, CD64/CD16+56/CD13/CD14/CD117/CD45, CD71/Glycophorin A/HLA-DR/CD20/CD22/CD45, CD99/CD58/CD33/CD25/CD52/CD45.
All antibodies were purchased from Becton-Dickinson (San Jose, CA, USA), except anti-CD52-APC (BioLegend, SanDiego, CA). CD25 (Clone M-A251, BD Biosciences, San Jose, CA, USA) was used for this study. The stained samples were run on BD-FACS Canto cytometer and analyzed with BD DIVA version 6.1.3 software (Becton-Dickinson, Franklin Lakes, New Jersey). Approximately 15,000 total events were acquired.
CD25 expression was reported as the percentage of CD25 positive lymphoblasts. CD25/CD52 dot plots were used to determine positive and negative populations by using normal lymphocytes as a reference to set the quadrants (Figure 1A and 1B). In the majority of cases, two distinct populations of residual normal CD25+ and CD25- lymphocytes were identified, and the quadrants were set between these two populations.
Figure 1.
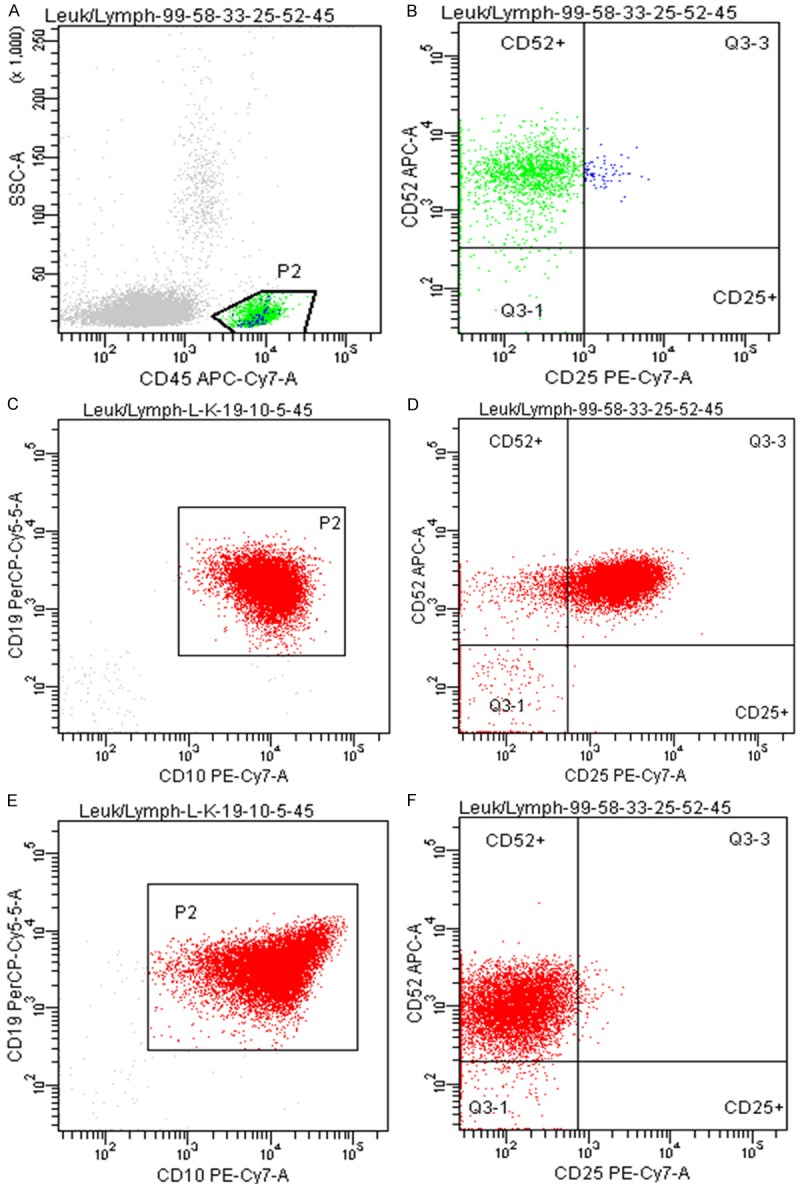
Representative plots used in CD25 analysis. A, B: Gating strategy for CD25 analysis. A: Normal lymphocytes (P2) were gated on a CD45 vs side scatter dot plot. B: Normal lymphocytes (P2) from plot A show a sub-population (in blue) that expresses CD25. This quadrant is used to identify the percentage of gated blasts that express CD25. C, D: Representative example of positive CD25 expression in B-ALL (Ph-negative). C: Gated lymphoblasts (P2) shown on a CD10 vs. CD19 plot. D: 90% of the gated lymphoblasts express CD25, which is considered positive. E, F: Representative example of negative CD25 expression in B-ALL (Ph-negative). E: Gated lymphoblasts (P2) on CD10 vs CD19 plot. F: 0.7% of gated lymphoblasts express CD25, which is considered negative.
Statistical analysis
IBM-SPSS Statistics v.21 was used for all statistical analysis. CD25 expression in Ph+ B-ALL was compared with Ph-negative B-ALL using the Mann-Whitney U test (MW). A receiver-operating characteristic (ROC) curve was generated to determine optimal cutoff values to distinguish Ph+ B-ALL from Ph-negative B-ALL, with a cutoff of 25% for CD25 expression to indicate a CD25-positive case.
Results
There were 221 pediatric B-ALL patients diagnosed in our hospital from May 2009 to June 2012, which was comprised of 118 males (53.4%) and 103 females (46.6%), and ranged in age from 2 to 22 years (median 6 years). Of note, two patients were older than 18 years old, 19 and 22, respectively, and both were negative for CD25 expression and were negative for BCR-ABL1 translocations. Eight (3.6%) B-ALL patients were BCR-ABL1 positive (Ph+ B-ALL), and 213 patients were BCR-ABL1 negative (Ph-negative B-ALL), by both chromosome and FISH analysis.
CD25 expression by flow cytometry was analyzed in newly diagnosed B-ALL patients (Figure 1C-F). Positive CD25 expression, using 25% as a cutoff, was observed in 6 of 8 (75%) Ph+ B-ALL patients [CD25+ Ph+ B-ALLs] with a median CD25 expression of 80.5% (range 26-93%). Among 2 Ph+ B-ALL cases with negative CD25 expression [CD25- Ph+ B-ALLs], CD25 expression was 0% and 6%, respectively. Positive CD25 expression was identified in 6 cases of 213 (2.8%) of Ph-negative B-ALL patients [CD25+ Ph-negative B-ALL] with a median CD25 expression of 63% (range 35-91%). Overall, CD25 expression was significantly higher in Ph+ B-ALL compared to Ph-negative B-ALL, with median CD25 expression of 64% (0-93%) and 0.1% (0-91%) respectively (P ≤ 0.0002) (Table 1). CD25 expression in Ph+ B-ALL had 75% sensitivity, 97% specificity, 50% positive predictive value (PPV) and 99% negative predictive value (NPV). Of note, we identified 4 patients who had relapsed B-ALL, with time of relapse ranging from 4 to 30 months, and all cases were Ph-negative B-ALL that showed negative CD25 expression in both original and relapse samples.
Table 1.
Association between CD25 expression and the Philadelphia chromosome (BCR-ABL1) translocation in pediatric B-ALL
| BCR-ABL1 Status | CD25- | CD25+ | Median CD25 Expression (%) | P |
|---|---|---|---|---|
| Ph-positive | 2 | 6 | 64 (0-93) | 0.00018 |
| Ph-negative | 207 | 6 | 0.10 (0-91) |
Discussion
Previous studies have been conducted to identify an association between CD25 expression and Ph+ B-ALL in adult populations. Our study is the first to specifically focus on pediatric patients [13-15,17]. The adult studies found an association between CD25 expression and adult Ph+ B-ALL cases. However, these studies use different methods to define a positive population, for example, some use an isotype control [13-15]. Moreover, different thresholds for assigning positive and negative CD25 expression were also used [13-15]. Another study did not describe an optimal cutoff [15]. An arbitrary cut off of 20% to define cases as positive for CD25 expression was used by another [14], while yet another used 30% as a cut off as determined by ROC curve [13]. In contrast to these studies, we used the normal lymphocyte population in each individual patient sample to determine positive and negative populations. We also found 25% to be an optimal cutoff as determined by ROC curve to define positive and negative CD25 expression in a pediatric population. We found 3.6% of pediatric B-ALL patients in our institution to be positive for the Philadelphia chromosome translocation by chromosome and FISH analysis, which is consistent with previously published findings of 3-5% prevalence in pediatric B-ALL [9,10]. Our analysis of pediatric patients diagnosed with B-ALL found significantly higher expression of CD25 in Ph+ B-ALL compared to that of Ph-negative B-ALL. Because of its excellent specificity (97%) and NPV (99%), CD25 could be used as an initial screening test for BCR-ABL1 in pediatric B-ALL, with the added benefit of a more rapid turnaround time for flow cytometry results than for FISH analysis. However, the low prevalence of BCR-ABL1 in pediatric B-ALL patients results in a higher number of false positives and a relatively low sensitivity of 75%. With a PPV of only 50% for CD25, potential use of CD25 expression as a diagnostic test for BCR-ABL1 is limited [18]. Nonetheless, identification of CD25 in a case of B-ALL could suggest prioritization of FISH analysis in order to confirm suspicions for Ph+ B-ALL, thus permitting earlier identification of Ph+ B-ALL and enrollment on appropriate treatment protocols.
We found CD25 expression, using a 25% cutoff, to be a specific and relatively sensitive marker for identifying Ph+ B-ALL in a pediatric population. Further investigation, however, is needed to determine optimal method and cutoff to assign cases as positive or negative for CD25 expression in adult and pediatric B-ALL as well as a prognostic significance of CD25 expression with or without Philadelphia chromosome.
Disclosure of conflict of interest
None.
References
- 1.Howlader NNA, Krapcho M, Garshell J, Neyman N, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA. SEER Cancer Statistics Review, 1975-2010. Bethesda, MD: National Cancer Institute; 2012. [Google Scholar]
- 2.Moricke A, Reiter A, Zimmermann M, Gadner H, Stanulla M, Dordelmann M, Loning L, Beier R, Ludwig WD, Ratei R, Harbott J, Boos J, Mann G, Niggli F, Feldges A, Henze G, Welte K, Beck JD, Klingebiel T, Niemeyer C, Zintl F, Bode U, Urban C, Wehinger H, Niethammer D, Riehm H, Schrappe M German-Austrian-Swiss ALL-BFM Study Group. Risk-adjusted therapy of acute lymphoblastic leukemia can decrease treatment burden and improve survival: treatment results of 2169 unselected pediatric and adolescent patients enrolled in the trial ALL-BFM 95. Blood. 2008;111:4477–89. doi: 10.1182/blood-2007-09-112920. [DOI] [PubMed] [Google Scholar]
- 3.Gaynon PS, Angiolillo AL, Carroll WL, Nachman JB, Trigg ME, Sather HN, Hunger SP, Devidas M. Long-term results of the children’s cancer group studies for childhood acute lymphoblastic leukemia 1983-2002: a Children’s Oncology Group Report. Leukemia. 2010;24:285–97. doi: 10.1038/leu.2009.262. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Moghrabi A, Levy DE, Asselin B, Barr R, Clavell L, Hurwitz C, Samson Y, Schorin M, Dalton VK, Lipshultz SE, Neuberg DS, Gelber RD, Cohen HJ, Sallan SE, Silverman LB. Results of the Dana-Farber Cancer Institute ALL Consortium Protocol 95-01 for children with acute lymphoblastic leukemia. Blood. 2007;109:896–904. doi: 10.1182/blood-2006-06-027714. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Pui CH, Campana D, Pei D, Bowman WP, Sandlund JT, Kaste SC, Ribeiro RC, Rubnitz JE, Raimondi SC, Onciu M, Coustan-Smith E, Kun LE, Jeha S, Cheng C, Howard SC, Simmons V, Bayles A, Metzger ML, Boyett JM, Leung W, Handgretinger R, Downing JR, Evans WE, Relling MV. Treating childhood acute lymphoblastic leukemia without cranial irradiation. N Engl J Med. 2009;360:2730–41. doi: 10.1056/NEJMoa0900386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Salzer WL, Devidas M, Carroll WL, Winick N, Pullen J, Hunger SP, Camitta BA. Long-term results of the pediatric oncology group studies for childhood acute lymphoblastic leukemia 1984-2001: a report from the children’s oncology group. Leukemia. 2010;24:355–70. doi: 10.1038/leu.2009.261. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Veerman AJ, Kamps WA, van den Berg H, van den Berg E, Bokkerink JP, Bruin MC, van den Heuvel-Eibrink MM, Korbijn CM, Korthof ET, van der Pal K, Stijnen T, van Weel Sipman MH, van Weerden JF, van Wering ER, van der Does-van den Berg A Dutch Childhood Oncology Group. Dexamethasone-based therapy for childhood acute lymphoblastic leukaemia: results of the prospective Dutch Childhood Oncology Group (DCOG) protocol ALL-9 (1997-2004) Lancet Oncol. 2009;10:957–66. doi: 10.1016/S1470-2045(09)70228-1. [DOI] [PubMed] [Google Scholar]
- 8.Moorman AV, Harrison CJ, Buck GA, Richards SM, Secker-Walker LM, Martineau M, Vance GH, Cherry AM, Higgins RR, Fielding AK, Foroni L, Paietta E, Tallman MS, Litzow MR, Wiernik PH, Rowe JM, Goldstone AH, Dewald GW Adult Leukaemia Working Party, Medical Research Council/National Cancer Research Institute. Karyotype is an independent prognostic factor in adult acute lymphoblastic leukemia (ALL): analysis of cytogenetic data from patients treated on the Medical Research Council (MRC) UKALLXII/Eastern Cooperative Oncology Group (ECOG) 2993 trial. Blood. 2007;109:3189–97. doi: 10.1182/blood-2006-10-051912. [DOI] [PubMed] [Google Scholar]
- 9.Arico M, Schrappe M, Hunger SP, Carroll WL, Conter V, Galimberti S, Manabe A, Saha V, Baruchel A, Vettenranta K, Horibe K, Benoit Y, Pieters R, Escherich G, Silverman LB, Pui CH, Valsecchi MG. Clinical outcome of children with newly diagnosed Philadelphia chromosome-positive acute lymphoblastic leukemia treated between 1995 and 2005. J. Clin. Oncol. 2010;28:4755–61. doi: 10.1200/JCO.2010.30.1325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Arico M, Valsecchi MG, Camitta B, Schrappe M, Chessells J, Baruchel A, Gaynon P, Silverman L, Janka-Schaub G, Kamps W, Pui CH, Masera G. Outcome of treatment in children with Philadelphia chromosome-positive acute lymphoblastic leukemia. N Engl J Med. 2000;342:998–1006. doi: 10.1056/NEJM200004063421402. [DOI] [PubMed] [Google Scholar]
- 11.Lee HJ, Thompson JE, Wang ES, Wetzler M. Philadelphia chromosome-positive acute lymphoblastic leukemia: current treatment and future perspectives. Cancer. 2011;117:1583–94. doi: 10.1002/cncr.25690. [DOI] [PubMed] [Google Scholar]
- 12.Pui CH, Evans WE. Treatment of acute lymphoblastic leukemia. N Engl J Med. 2006;354:166–78. doi: 10.1056/NEJMra052603. [DOI] [PubMed] [Google Scholar]
- 13.Jaso J, Thomas DA, Cunningham K, Jorgensen JL, Kantarjian HM, Medeiros LJ, Wang SA. Prognostic significance of immunophenotypic and karyotypic features of Philadelphia positive B-lymphoblastic leukemia in the era of tyrosine kinase inhibitors. Cancer. 2011;117:4009–17. doi: 10.1002/cncr.25978. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nakase K, Kita K, Miwa H, Nishii K, Shikami M, Tanaka I, Tsutani H, Ueda T, Nasu K, Kyo T, Dohy H, Shiku H, Katayama N. Clinical and prognostic significance of cytokine receptor expression in adult acute lymphoblastic leukemia: interleukin-2 receptor alpha-chain predicts a poor prognosis. Leukemia. 2007;21:326–32. doi: 10.1038/sj.leu.2404497. [DOI] [PubMed] [Google Scholar]
- 15.Paietta E, Racevskis J, Neuberg D, Rowe JM, Goldstone AH, Wiernik PH. Expression of CD25 (interleukin-2 receptor alpha chain) in adult acute lymphoblastic leukemia predicts for the presence of BCR/ABL fusion transcripts: results of a preliminary laboratory analysis of ECOG/MRC Intergroup Study E2993. Eastern Cooperative Oncology Group/Medical Research Council. Leukemia. 1997;11:1887–90. doi: 10.1038/sj.leu.2400836. [DOI] [PubMed] [Google Scholar]
- 16.Borowitz MJ, Chan JKC. Precursor Lymphoid Neoplasms. In: Swerdlow SHCE, Harris NL, editors. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. Fourth edition. Lyon, France: IARC; 2008. pp. 168–175. [Google Scholar]
- 17.Geng H, Brennan S, Milne TA, Chen WY, Li Y, Hurtz C, Kweon SM, Zickl L, Shojaee S, Neuberg D, Huang C, Biswas D, Xin Y, Racevskis J, Ketterling RP, Luger SM, Lazarus H, Tallman MS, Rowe JM, Litzow MR, Guzman ML, Allis CD, Roeder RG, Müschen M, Paietta E, Elemento O, Melnick AM. Integrative epigenomic analysis identifies biomarkers and therapeutic targets in adult B-acute lymphoblastic leukemia. Cancer Discov. 2012;2:1004–23. doi: 10.1158/2159-8290.CD-12-0208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Altman DG, Bland JM. Diagnostic tests 2: Predictive values. BMJ. 1994;309:102. doi: 10.1136/bmj.309.6947.102. [DOI] [PMC free article] [PubMed] [Google Scholar]