

Abstract
Background
'Traffic light' (red-yellow-green) maps are potentially powerful tools for 'at a glance' problem detection, for optimising resource allocation/reallocation, setting priorities, and targeting interventions to areas most in need. The maps can be also used for administrative area comparisons and performance monitoring over time. Interactive Web versions of the maps can be generated with many handy features to further empower organisations and decision makers. Methodological issues to consider when creating 'traffic light' maps include hue thresholding, data timeliness and stability of administrative boundaries.
Results
We used 'traffic light' maps to study the distribution of dentists per 1,000 population in all 304 English Primary Care Trusts (PCTs) and 22 Welsh Local Health Boards (LHBs) using datasets of dentist numbers per PCT (as at 31 December 2002) and LHB (as at 26 February 2004) from the Dental Practice Board, and 2001 Census population figures for PCTs and LHBs from the Office for National Statistics. The overall NHS dentists per 1,000 population figures for England (0.374) and Wales (0.359) are low compared to many other countries, with less than 0.3 dentist per 1,000 people available to 24.1% of the total population of England (81 PCTs or 26.6% of all PCTs) and 26.1% of the total population of Wales (6 LHBs or 27.3% of all LHBs). A general shortage of NHS dentists can be observed at a glance across England and Wales on all the 'traffic light' maps in our study, even on those using a more "tolerant" classification and an additional orange-yellow class. The distribution of NHS dentists in England and Wales was also found to be not uniform, with some PCTs/LHBs, especially those located in some of the deprived or less populated urban and rural communities, suffering significantly more shortage of dentists than others (see http://healthcybermap.org/PCT/dentists/). These results confirm recent media reports of a shortage of NHS dentists in various parts of England and Wales.
Conclusion
Suitable programmes are urgently needed to increase the numbers of NHS dentists across England and Wales. We have included a set of recommendations to dental health policymakers and planners, in addition to ideas for further work.
Background
What is happening to NHS dentistry in England and Wales?
The number of adults registered with a National Health Service (NHS) dentist in England and Wales has sharply declined over recent years. As of 2002, less than 50% of the population were registered with an NHS dentist. In some places today, no dentists will accept adult NHS patients, which is of particular concern to people with low incomes who have to pay higher, private sector charges or travel long distances to obtain NHS treatment [1,2].
In 2003 and 2004, NHS dentistry received very negative media coverage. Reports repeatedly described the picture of hundreds of people in different parts of England and Wales spending hours queuing to register with an NHS dentist because they are unable to afford private treatment, with many of them being turned away at the end. A shortage of dentists and the increasing number of existing dentists who are dropping their NHS commitment in favour of more lucrative private work have been put forward as the main causes for the current state of affairs of NHS dentistry [3-10]. According to a media release from the GDPA (General Dental Practitioners' Association), which carried out a national survey in November 2003, over 90 per cent of dentists will be doing less NHS work in five years [11].
Almost all dentists in the UK are self-employed and have traditionally mixed NHS and private patients on their books. Based on National Statistics' mid-2002 population estimates for Great Britain (England, Scotland and Wales: 57,535,300) and their quoted figure of 22,194 general dental practitioners working in Great Britain as of 2002 (General and Personal Dental Services – dentists having contracts with more than one Health Authority have been counted only once), the number of dentists per 1,000 population in Great Britain is 0.386 [12,13]. This figure is low compared to many other countries. For example, the corresponding 1996/1997 figures of practising dentists per 1,000 population reported in 'OECD (Organisation for Economic Co-operation and Development) Health Data 1998' are 0.5 for Austria, Canada, Italy and Poland, 0.6 for the Czech Republic and the United States, 0.7 for Belgium and Germany, 0.8 for Norway and 0.9 for Finland. The 1995 figures from the same report are 0.5 for Denmark, Hungary, Netherlands and Switzerland, 0.7 for France and 1.0 for Greece and Sweden (cited in [14]). (At the time of writing, we didn't have access to the latest OECD Health Data 2003, which can be purchased from http://www.oecd.org/document/30/0,2340,en_2649_34631_12968734_1_1_1_1,00.html).
The role of GIS in dental care
Today's health planners aim at developing health policy and services that address geographic and social inequalities in health, and therefore should benefit from evidence-based approaches that can be used to investigate spatial aspects of health policy and practice, and evaluate geographic equity (or inequity) in health service provision [15].
The cost of General Dental Services to the government in the year to March 2002 was £1.12 billion (about two per cent of the annual NHS budget of £65 billion in 2002) [1]. Under the recent Health and Social Care (Community Health and Standards) Act 2003, from April 2005 commissioning and contracting for NHS dentistry will devolve from the Department of Health to PCTs (Primary Care Trusts) [16]. Moreover, in September 2003, it was announced that £65.2 million will be made available to improve dental care for NHS patients. Of this latter sum, £35 million will be allocated to enable PCTs to improve access, choice and quality for patients, and £30 million will be directed to information technology to integrate dentistry within the national information technology programme [17]. The latter has yet to recognise the many potentials of spatial information and GIS (Geographic Information Systems) for the NHS [18].
Profiling service areas and needs assessment, dental healthcare commissioning, and improving/ensuring equitable access to dental services are all areas where GIS can make a positive difference. GIS have significant potential in examining spatial patterns in dental health, and in analysing patterns of registration and utilisation of dental services for different sectors of the community. GIS can reveal gaps in dental health provision, and thus help target resources and programmes to particular areas of needs. GIS can be also used to analyse the composition and spatial distribution of the dental workforce, and to inform the development and monitor the execution of programmes for attracting dental care professionals to work in under-served areas [15,19,20].
'Traffic light' maps as a decision support tool
'Traffic light' maps are potentially powerful tools for 'at a glance' problem detection, for identifying priority actions and targeting interventions to areas most in need. They can be used for performance monitoring of administrative areas, e.g., PCTs, over time, and also administrative area comparisons.
The simplest 'traffic light' maps use only one tint/shade of each of the three basic hues (red, yellow and green) to represent three 'traffic light' classes, but if required, more than one tint/shade of red and/or yellow and/or green can be used to represent more transition points/level ranges or classes of mapped variables. Blue is also sometimes inserted between yellow and green.
The colours are used to distinguish between, and compare at a glance map areas associated with: (1) a range of decisions or plans/actions of varying quantity, quality or priority; or (2) high, medium, and low level ranges of variables that have practical implications, e.g., prompting different courses of action or different degrees of endorsement of the same action depending on level range.
Depending on the mapped topic and the quality to be conveyed, e.g., capacity, potentiality, severity, vulnerability, risk, suitability/readiness for some action, or urgency/priority, the red and green ends of the 'traffic light' map spectrum can assume different meanings. Figure 1 shows some of the meanings commonly associated with red, yellow and green colours in the context of 'traffic light' maps.
Figure 1.

Meanings commonly associated with red, yellow and green colours Some of the meanings commonly associated with red, yellow and green colours in the context of 'traffic light' maps.
Many good examples of 'traffic light' maps exist. Kelly and Murekezi produced colour-coded maps using the 'traffic light' colours of red, yellow, and green to convey fertiliser promotion recommendations for each crop analysed in Rwanda, with green at one end denoting that a strong fertiliser promotion programme is recommended, and red at the other end denoting that fertiliser promotion is not recommended. Grey and white were used to shade areas for which inconclusive or no data were available [21].
A World Bank Policy Research Working Paper by Kaufmann et al features 'traffic light' maps depicting six dimensions of governance (voice and accountability, political stability, government effectiveness, regulatory quality, rule of law, control of corruption) covering 199 countries and territories for four time periods (1996, 1998, 2000, and 2002). The maps use three hue classes (green, yellow and red) and different shades/tints of the three basic hues (dark green, light green, yellow, orange, light red/pink and red). Each country colour pattern follows a simple quartile distribution: the best quartile (over 75th percentile) is in green (with top 10th coloured in darker green), the second best quartile (over 50th) is in yellow, the third (over 25th) is in orange, and the fourth is in red (with bottom 10th in darker red). If data are unavailable for a country, it is coloured in dark grey. The maps allow at a glance appreciation of governance data by country and country comparisons. An interactive online version of the maps is also available http://info.worldbank.org/governance/kkz2002/govmap.asp – Figure 2) [22].
Figure 2.
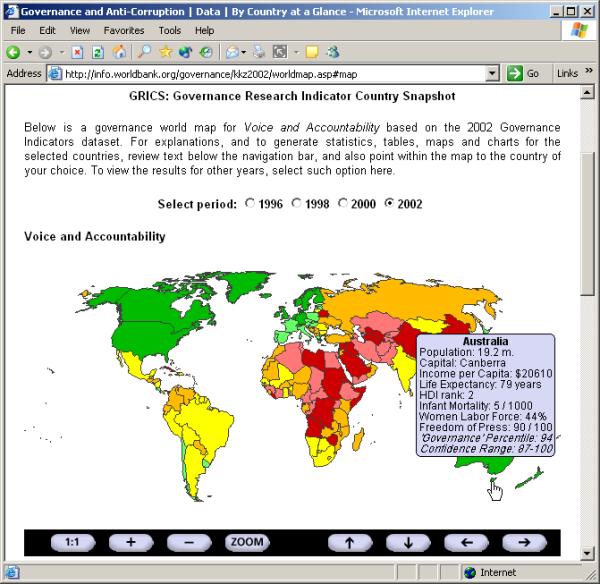
An interactive online example of 'traffic light' maps Web browser screenshot by this author of one of the World Bank's interactive online governance world maps. The 'traffic light' map featured in this screenshot shows the 'voice and accountability' governance indicator results for the year 2002 http://info.worldbank.org/governance/kkz2002/gov2001map.asp. The Web-based map interface tool allows users to view results for other years(1996, 1998, 2000, 2002), and offers zooming, panning and drill-down functionalities. The latter displays the underlying map data and details (a map tip is displayed on moving the mouse over a country; clicking the country displays corresponding country charts of all 6 governance indicators).
The National Retail Data Monitor (NRDM – http://www.health.pitt.edu/rods/NRDM.htm), developed at the Real-time Outbreak and Disease Surveillance Laboratory (RODS), Centre for Biomedical Informatics, University of Pittsburgh, US, monitors sales of over-the-counter healthcare products to identify disease outbreaks as early as possible. NRDM maps plot for each Zip Code – using the colours green, blue, yellow, orange, and red to indicate increasing levels of concern – how "unusual" sales were for the day in question relative to historical patterns of sales for that Zip Code [23]. This 'red-orange-yellow-blue-green' colour system is identical to the one used in the US Homeland Security Advisory System [24].
Traffic light' colours were also used in some of the maps published in the Atlas of Cancer Mortality and Other Causes of Death in Spain, 1978–1992 http://www2.uca.es/hospital/atlas92/www/Atlas92.html.
In this paper, we describe and discuss another use of 'traffic light' maps to study the distribution of dentists per 1,000 population in all 304 English PCTs and 22 Welsh Local Health Boards (LHBs). This is one way of measuring the level of access to dental care in various parts of England and Wales, and can be very useful in informing dental health policymakers and planners to optimise and target programmes to attract more dentists to areas in need. It is also hoped that this small GIS exercise will act as another "proof of concept and benefits application", which is much needed today to convince more people about the value of GIS in health and healthcare in order to gain and sustain proper support, and secure further funding for wider and much better coordinated GIS programmes within the NHS [18].
Results
Dentists per 1,000 population in England
In England, the overall number of NHS dentists per 1,000 population was found to be 0.374 based on a Census 2001 total population figure of 49.1 million (49,138,831) and a Dental Practice Board figure of 18,369 dentists in the 304 English PCTs as at 31 December 2002 (including 16,429 principals, 1,348 assistants and 592 vocational trainees – dentists who were both principals and assistants have been counted once as principals). A detailed analysis showed that 3.9 million (3,904,057 or 7.9%) people live in PCT areas (26 PCTs or 8.6% of all PCTs) served by 0.5 or more dentist per 1,000 population (the median for this class interval is 0.53 dentist per 1,000 people), 14.1 million (14,099,290 or 28.7%) live in PCT areas (80 PCTs or 26.3% of all PCTs) served by 0.4–0.499 dentist per 1,000 population, and the remaining 31.1 million (31,135,484 or 63.4 %) live in PCT areas (198 PCTs or 65.1% of all PCTs) served by less than 0.4 dentist per 1,000 population. Of the latter group, 11.8 million (11,834,724 or 24.1% of the total population of England) live in PCT areas (81 PCTs or 26.6% of all PCTs) served by less than 0.3 dentist per 1,000 population (0.159–0.299).
Figure 3 is a 'traffic light' map of England showing the distribution of dentists per 1,000 people by PCT as at 31 December 2002, classified into three classes: 0–0.4 (red), 0.4–0.5 (orange-yellow) and 0.5–1 (green) dentist per 1,000 population. An online version of this map with minimal interactivity has also been produced to give the reader some flavour of what can be done to communicate map results to the decision maker in a more efficient and effective way on the Internet or an intranet http://healthcybermap.org/PCT/dentists/. In Figure 4, the same data were classified into four classes to produce another 'traffic light' map: 0–0.2 (red), 0.2–0.3 (dark orange-yellow), 0.3–0.4 (light orange-yellow) and 0.4–1 (green) dentist per 1,000 population. Table 1 presents selected records from the dentists distribution dataset for England that was used to produce the above mentioned maps. The selected rows show details of PCTs with the highest and lowest figures of dentists per 1,000 population.
Figure 3.
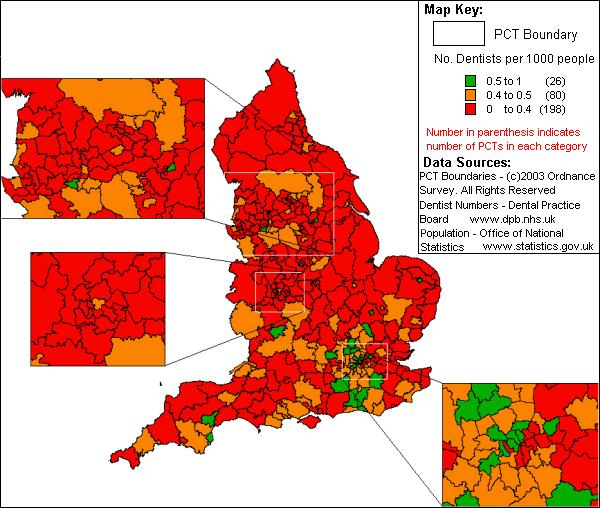
'Traffic light' map of dentists distribution per 1,000 people by PCT in three classes 'Traffic light' map of England showing the distribution of dentists per 1,000 people by PCT as at 31 December 2002, classified into three classes: 0–0.4 (red = shortage of NHS dentists), 0.4–0.5 (orange-yellow = some shortage of NHS dentists) and 0.5–1 dentist per 1,000 population (green = acceptable/good number of dentists).
Figure 4.
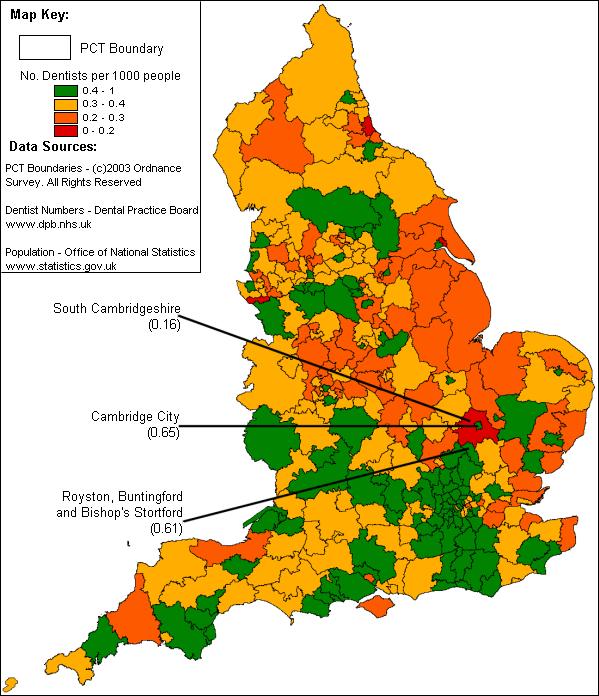
'Traffic light' map of dentists distribution per 1,000 people by PCT in four classes 'Traffic light' map of England showing the distribution of dentists per 1,000 people by PCT as at 31 December 2002, classified into four classes: 0–0.2 (red = serious shortage of NHS dentists), 0.2–0.3 (dark orange-yellow = shortage of NHS dentists), 0.3–0.4 (light orange-yellow = some shortage of NHS dentists) and 0.4–1 dentist per 1,000 population (green = low, but acceptable or good number of dentists). Note the location of South Cambridgeshire PCT, which has a very low dentist per 1,000 population figure of 0.16, in relation to Cambridge City and Royston, Buntingford and Bishop's Stortford PCTs, which both have a dentist per 1,000 population figure of more than 0.6.
Table 1.
Details of English PCTs with the highest and lowest figures of dentists per 1,000 population. For each PCT, the total number of dentists as at 31 December 2002 is shown. This includes principals, assistants and vocational trainees. Dentists who were both principals and assistants have been counted once as principals.
| Primary Care Trust | Population (Census 2001) | Number of dentists (2002) | Dentists per 1,000 people |
| Westminster | 181286 | 160 | 0.882583 |
| Doncaster Central | 69292 | 49 | 0.707152 |
| Cambridge City | 108863 | 71 | 0.652196 |
| South West Kent | 176439 | 109 | 0.617777 |
| Camden | 198020 | 122 | 0.616099 |
| Hammersmith and Fulham | 165242 | 101 | 0.611225 |
| Royston, Buntingford and Bishop's Stortford | 62249 | 38 | 0.610452 |
| Yorkshire Wolds and Coast | 143541 | 30 | 0.209000 |
| Hinckley and Bosworth | 115258 | 24 | 0.208228 |
| Central Suffolk | 98786 | 20 | 0.202458 |
| Eastern Hull | 116394 | 23 | 0.197605 |
| South Cambridgeshire | 130689 | 21 | 0.160687 |
| Easington | 93993 | 15 | 0.159586 |
| Ellesmere Port and Neston | 81672 | 13 | 0.159173 |
Dentists per 1,000 population in Wales
In Wales, the overall number of NHS dentists per 1,000 population was found to be 0.359 based on a Census 2001 total population figure of 2.9 million (2,903,085) and a Dental Practice Board figure of 1,042 principal dentists in the 22 Welsh LHBs as at 26 February 2004 (dentists were counted in each LHB that they have a contract). A detailed analysis revealed that 0.8 million (841,499 or 29%) people live in LHB areas (5 LHBs or 22.7% of all LHBs) served by 0.417–0.488 dentist per 1,000 population, while the remaining 2.1 million (2,061,586 or 71%) live in LHB areas (17 LHBs or 77.3% of all LHBs) served by 0.24–0.373 dentist per 1,000 population. Of the latter group, 0.76 million (756,519 or 26.1% of the total population of Wales) live in LHB areas (6 LHBs or 27.3% of all LHBs) served by less than 0.3 dentist per 1,000 population (0.24–0.299).
Figure 5 is a 'traffic light' map of Wales showing the distribution of dentists per 1,000 people by LHB as at 26 February 2004, classified into three classes: 0–0.4 (red), 0.4–0.5 (orange-yellow) and 0.5–1 (green) dentist per 1,000 population. In Figure 6, the same data were classified into four classes to produce another 'traffic light' map: 0–0.2 (red), 0.2–0.3 (dark orange-yellow), 0.3–0.4 (light orange-yellow) and 0.4–1 (green) dentist per 1,000 population. An online version of this map with minimal interactivity has also been produced (http://healthcybermap.org/LHB/dentists/ – Figure 7). Table 2 presents selected rows from the dentists distribution dataset for Wales that was used to produce the above mentioned maps. The chosen records show details of LHBs with the highest and lowest figures of dentists per 1,000 population.
Figure 5.
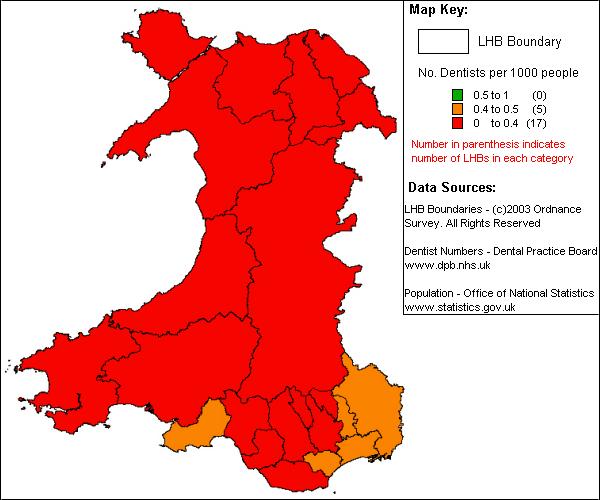
'Traffic light' map of dentists distribution per 1,000 people by LHB in three classes 'Traffic light' map of Wales showing the distribution of dentists per 1,000 people by LHB as at 26 February 2004, classified into three classes: 0–0.4 (red = shortage of NHS dentists), 0.4–0.5 (orange-yellow = some shortage of NHS dentists) and 0.5–1 dentist per 1,000 population (green = acceptable/good number of dentists).
Figure 6.
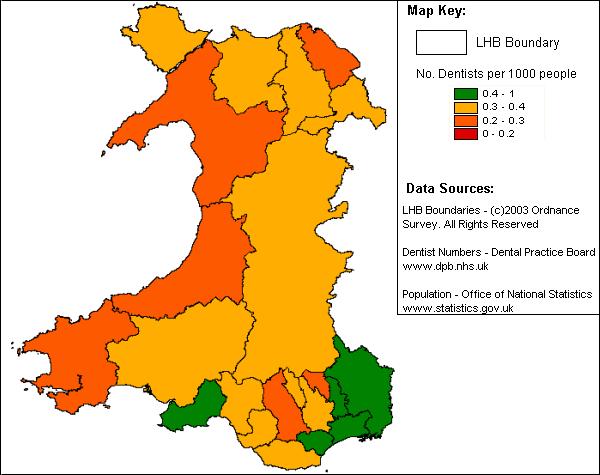
'Traffic light' map of dentists distribution per 1,000 people by LHB in four classes 'Traffic light' map of Wales showing the distributionof dentists per 1,000 people by LHB as at 26 February 2004, classified into four classes: 0–0.2 (red = serious shortage of NHS dentists), 0.2–0.3 (dark orange-yellow = shortage of NHS dentists), 0.3–0.4 (light orange-yellow = some shortage of NHS dentists) and 0.4–1 dentist per 1,000 population (green = low, but acceptable or good number of dentists).
Figure 7.
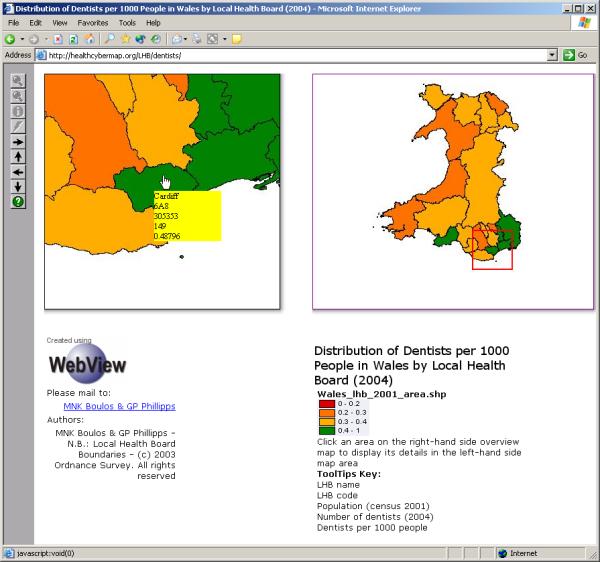
Online interactive 'traffic light' map of dentists distribution per 1,000 people by Welsh LHB Web browser screenshot of our online version of the 'traffic light' map of Wales showing the distribution of dentists per 1,000 people by LHB in four classes as at 26 February 2004 http://healthcybermap.org/LHB/dentists/. The online map interface offers some interactivity. Panning in the detail map (left-hand side map area) is possible, either by using the arrow buttons (toolbar on the left) or by clicking an area on the right-hand side overview map. Attribute information (map tips) are displayed on moving the mouse over the detail map.
Table 2.
Details of Welsh LHBs with the highest and lowest figures of dentists per 1,000 population. For each LHB, the number of principal dentists as at 26 February 2004 is shown. Dentists were counted in each LHB that they have a contract.
| Local Health Board | Population (Census 2001) | Number of dentists (2004) | Dentists per 1,000 people |
| Cardiff | 305353 | 149 | 0.48796 |
| Monmouthshire | 84885 | 41 | 0.483006 |
| Swansea | 223301 | 95 | 0.425435 |
| Newport | 137011 | 64 | 0.467116 |
| Torfaen | 90949 | 38 | 0.417817 |
| Pembrokeshire | 114131 | 33 | 0.289141 |
| Rhondda, Cynon, Taff | 231946 | 67 | 0.28886 |
| Blaenau Gwent | 70064 | 20 | 0.285453 |
| Flintshire | 148594 | 42 | 0.282649 |
| Ceredigion | 74941 | 18 | 0.240189 |
The complete dentists distribution datasets that were used to produce all the maps for England and Wales in this study are also included as an additional file with this manuscript (Additional file 1 – Microsoft Excel Workbook).
Discussion
A shortage of NHS dentists in England and Wales
The overall NHS dentists per 1,000 population figures for England (0.374) and Wales (0.359) are low compared to many other countries (see "Background" section above). Though there is no Government target for the number of NHS dentists per 1,000 population [25], it seems appropriate to consider a figure of '0.5 dentist per 1,000 population' as an acceptable/adequate target (floor not ceiling target) based on corresponding figures for other developed countries. (The 'traffic light' map in Figure 3 adopts this figure of 0.5 dentist per 1,000 people for the lower end of its green class (>=0.5).)
We created two sets of 'traffic light' maps for England (PCTs) and Wales (LHBs), varying the thresholding of hues in each set to produce two maps, with three and four classes, for each country (Figures 3, 4, 5, 6). A general shortage of NHS dentists can be observed at a glance across England and Wales, even in the second set of maps (the maps with four classes – Figures 4, 6), which use a more "tolerant" classification with a reduced minimum of 0.4 dentist per 1,000 population for the green class (instead of 0.5), and a reduced maximum for the red band (0.2 dentist per 1,000 people instead of 0.4), with an extra orange-yellow class.
The distribution of dentists in England and Wales is not uniform, with some PCTs/LHBs suffering more shortage of dentists than others (Tables 1, 2). Dentists tend to be somewhat concentrated in major cities/urban centres and away from some of the deprived or less populated urban and rural communities, e.g., the rural South Cambridgeshire PCT with a Census 2001 population of 130,689 and only 0.16 dentist per 1,000 people as at 31 December 2002.
Although we are using 2002 dentists data for England, our results seem to echo and confirm recent media reports of a serious shortage of NHS dentists in parts of England. Whilst the mean yearly increase in NHS dentist numbers between March 1992 and March 2003 was 1.5% (with much higher percents in some years, e.g., a 4% increase in March 1998 compared to March 1997), the total number of NHS dentists in England and Wales has grown very little since December 2002 (19,379 to 19,555 as of September 2003 or a 0.9% increase), so the picture for England should be largely the same today [26]. As mentioned before, our results also reveal a shortage of NHS dentists in large parts of Wales (using 2004 data for Wales).
An important point to note is that a dentist holding a GDS (General Dental Service) contract to provide NHS services has no commitment at the present time to provide specific levels of service, and may, in fact, provide extremely limited access to NHS care and only have a small number of NHS patients.
Westminster, a very affluent area, has 0.88 dentists per 1000 population (Table 1), and as such would appear well served with NHS dentists, however, it may be that these dentists commit very limited time to NHS work and access problems to NHS dentistry may actually be quite considerable for this area.
On the other hand, Ellesmere Port and Neston, which appears to be poorly served with only 0.159 dentists per 1000 people (Table 1), may be enjoying greater access to NHS dental care, as the dentists in this area are likely to be spending most of their clinical time providing NHS treatment (see also http://www.dpb.nhs.uk/mod_dentistry/documents/December_report.pdf).
Consequently, the current figures and maps should be only taken as an indication of the level of overall provision of NHS dental services. A more complete representation of the actual access to NHS dental care in different PCTs would require more data to indicate the level of NHS provision attributed to each dentist (see "What else can be done?" below).
'Traffic light' maps for PCT/LHB performance monitoring over time
A simple time series analysis (comparing 'traffic light' maps of England and Wales for successive periods of time) can demonstrate changes over time in different PCTs/LHBs (deteriorating, stable or improving situations). If corrective programmes/interventions are implemented, we can gauge their success by watching/monitoring their effects on the targeted areas over time (e.g., a positive change from orange-yellow to green). We can then modify our plans/programmes accordingly, if needed. Animated time series maps can be also created to communicate findings (for some examples of animated time series maps, see http://circ.rupri.org/animation/).
'Traffic light' maps for PCT/LHB comparisons
We think PCT and LHB directors will be keen to look at local/regional comparisons between 'competing' PCTs and LHBs. The Georgia Medical Care Foundation Diabetes Quality Indicators project http://www.gmcf.org/Professional/initiatives/Diabetes/interactive/ provides a good example of how such comparisons could help improving practice. At a glance visual PCT/LHB comparisons as provided by our 'traffic light' maps would also certainly add much value to the kind of textual and tabular reports currently produced by the Commission for Health Improvement on PCT performance against targets http://www.chi.nhs.uk/Ratings/Search/SearchResults.asp?TrustType=PCT.
Online interactive 'traffic light' maps for better communication of results
We have also generated online versions of the 'traffic light' maps presented in Figures 3 and 6 (available from http://healthcybermap.org/PCT/dentists/ and http://healthcybermap.org/LHB/dentists/ – Figure 7). These particular online versions offer limited interactivity, and are only meant to give the reader some flavour of what can be done to share map results in better ways on the Internet or an intranet (using only a standard Web browser), and further empower the decision maker who is reading the map. Interactivity features vary depending on the software used to produce the online interactive version of a desktop GIS map [27], and include the ability of the online map user to query the map and display attribute information, to perform other GIS functions as necessary, and in the case of 'traffic light' maps to vary the thresholding of hues (class intervals in choropleth maps) and see the results of this instantly on the map, in addition to the basic map zooming and panning capabilities.
What else can be done?
Though the 'traffic light' maps and results presented in this study give some very useful insights into the distribution of the NHS dental workforce in England and Wales, we still need to investigate the factors and determinants causing, or associated with the observed distribution. Despite the improvements in oral health that have been reported since the early 1970s in many parts of the UK, the picture of dental health in deprived areas looks less rosy, with fewer people registered with a dentist (see also http://www.empho.org.uk/products/dentalreport2004.pdf). In some localities children's decay levels are as bad as they were 15 years ago [2]. A multivariate geographic analysis could be conducted of dentists distribution in different regions in relation to the following factors and determinants in these areas: (1) administrative area size and nature (urban, accessible rural or remote rural); (2) local population size, distribution, socio-economic characteristics and other demographics; (3) local transport networks; (4) figures of registration with NHS dentists and of service use (figures of visits to NHS dentists and breakdown of corresponding diagnoses/procedures); and (5) dental health indicators/outcomes (see the examples of oral health indicators published by the US National Institute of Dental and Craniofacial Research (NIDCR) and the CDC Division of Oral Health: http://drc.nidcr.nih.gov/indicators.htm). 'Traffic light' maps are much suited for mapping NHS dentist registrations per PCT, and also oral health indicators by PCT like the prevalence of untreated dental caries by age/selected demographics.
Besides examining the numbers of patient registrations with NHS dentists per PCT, investigating the total figures for the proportion of NHS to private work provided by dentists per PCT could also give a clearer indication of the level of NHS dental treatment within each PCT. Another possibility is to use dentists' practice profiles, which state annual workload and fees earned within the NHS, with comparisons with local and national figures. This might indicate the volumes of NHS work done within each PCT (see also http://www.dpb.nhs.uk/mod_dentistry/documents/pctguidancejan04.pdf).
It is noteworthy that in the US where Medicaid operates similarly to the NHS dental system (in some respects – see http://www.cga.state.ct.us/ps99/rpt/olr/htm/99-r-0428.htm and http://www.nashp.org/_docdisp_page.cfm?LID=448D07B6-6CBC-11D6-BD1100A0CC76FF4C), dentists voluntarily enroll as Medicaid providers in most states and by contract must do some things, but may not be required to participate at minimum levels or to see a certain number of Medicaid patients. Different metrics for measuring dentists' participation in Medicaid have been used or suggested, e.g., seeing a certain number of Medicaid patients within some time period, but so far there have been no agreement on a "best" measure [28,29].
The same 'traffic light' map exercise can be also repeated for PCT 'median waiting time' and 'waiting list size' (figures included in Hospital Episode Statistics, which can be freely downloaded from the Department of Health Web site: http://www.dh.gov.uk/PublicationsAndStatistics/Statistics/HospitalEpisodeStatistics/fs/en) after determining what are the appropriate (national/target) figures for (1) waiting time; and (2) waiting list size (when addressing waiting list size, we need to take into consideration PCT population size). The maps would show PCTs with bad (red), not so bad (orange-yellow), and good/excellent waiting time/list size (green), and enable comparing and monitoring PCTs over time for these targets.
Recommendations
Suitable programmes are urgently needed to increase the numbers of NHS dentists across England and Wales. To ensure their success, such programmes must take into consideration the current distribution of NHS dentists per 1,000 people in different PCTs/LHBs, so that areas with the lowest figures (most in need) are given the highest priority. When targeting different areas, factors and determinants causing, or associated with the currently observed distributions should be also addressed for best results (see "What else can be done?" above).
Based on National Statistics' mid-2002 population estimates for England (49,561,800) and Wales (2,918,700) [12], if we are to increase the overall figure of NHS dentists per 1,000 population by just 0.1, we will have to provide extra 4,956 dentists for England and a further 292 dentists for Wales (or a total of 5,248 more dentists for England and Wales). Such large figures could be met on the short term by developing better programmes to attract more dentists to undertake more NHS work and by relying on suitably qualified foreign dental graduates (which is already taking place – see [30]), and on the longer term by providing further support to dental schools and increasing the number of dental graduates in the UK (the figure was 749 graduates in the year 2000 [31]).
Another possible short term remedy, where conditions and logistics permit (e.g., availability of suitable local transport networks), involves redirecting/reallocating resources (in controlled ways) from areas of surplus to neighbouring areas where a shortage has been detected. 'Traffic light' maps can help instantly spot areas where this might be feasible. For example, Cambridge City PCT with a relatively high figure of 0.65 dentist per 1,000 people is surrounded by the rural South Cambridgeshire PCT, which has a very low figure of 0.16 dentist per 1,000 people. It might be possible for dentists working for Cambridge City PCT to also take on their lists patients from the neighbouring South Cambridgeshire PCT, but it could be that Cambridge City PCT cannot provide for all of South Cambridgeshire PCT dentistry needs, as the combined dentist per 1,000 people figure for both PCTs together is 0.384. Royston, Buntingford and Bishop's Stortford PCT, another neighbouring PCT with a relatively high figure of 0.61 dentist per 1,000 people, can also potentially provide help to South Cambridgeshire PCT (Table 1 and Figure 4). The combined dentist per 1,000 people figure for the three PCTs is 0.43.
The above recommendation may in fact be already taking place, as patients are free to visit any NHS dentist in any area, and many patients choose a dentist who is more conveniently located in relation to their work rather than home. This is often why there are increased numbers of dentists in city centres where people are employed, rather than in the suburbs.
In all cases, NHS work needs to be made more attractive to dentists, e.g., by offering them better payment schemes.
Conclusions
'Traffic light' (red-yellow-green) maps are potentially powerful tools for 'at a glance' problem detection, for identifying priority actions, for optimising resource allocation/reallocation and targeting interventions to areas most in need. The maps can be also used for performance monitoring of administrative areas over time, and for administrative area comparisons. Interactive Web versions of the maps can be generated with many handy features to better communicate map results and further empower the decision maker who is reading the maps. Methodological issues to consider when creating 'traffic light' maps include hue thresholding, data timeliness and stability of administrative boundaries.
We used 'traffic light' maps to study the distribution of dentists per 1,000 population in all 304 English PCTs and 22 Welsh LHBs using datasets of dentist numbers per PCT (as at 31 December 2002) and LHB (as at 26 February 2004) from the Dental Practice Board, and 2001 Census population figures for PCTs and LHBs from the Office for National Statistics. We used the 2001 Census PCT (post April 2002 change) and LHB (post April 2003 change) boundary datasets from Ordnance Survey. The overall NHS dentists per 1,000 population figures for England (0.374) and Wales (0.359) were found to be low compared to many other countries, with less than 0.3 dentist per 1,000 people available to 24.1% of the total population of England (81 PCTs or 26.6% of all PCTs) and 26.1% of the total population of Wales (6 LHBs or 27.3% of all LHBs). (Whilst such a comparison requires validation by more holistic investigation of dental health conditions and infrastructure between countries, it does indicate a level of accessibility to NHS dentists by the UK population.) A general shortage of NHS dentists can be observed at a glance across England and Wales on all the 'traffic light' maps we have created, even on those using a more "tolerant" classification and an additional orange-yellow class. The distribution of NHS dentists in England and Wales was also found to be not uniform, with some PCTs/LHBs, especially those located in some of the deprived or less populated urban and rural communities, suffering significantly more shortage of dentists than others.
Despite the limitations of the data we have used in this study (only counting dentists holding contract(s) for GDS services and not taking into consideration other factors affecting NHS dental care provision), our results confirm recent media reports of a shortage of NHS dental services in various parts of England and Wales. Suitable programmes are urgently needed to increase the numbers of NHS dentists and levels of NHS dental care they provide across England and Wales. We have included a set of recommendations to dental health policymakers and planners based on the results of our study, in addition to ideas for further studies.
Methods
Datasets and software used
To compute the numbers of dentists per 1,000 population in all 304 English PCTs and 22 Welsh LHBs, we used datasets of dentist numbers per PCT (as at 31 December 2002) and LHB (as at 26 February 2004) from the Dental Practice Board (http://www.dpb.nhs.uk/ – see "Acknowledgements" section below) and a dataset of 2001 population figures for PCTs and LHBs from Neighbourhood Statistics and Census Output Division, Office for National Statistics (dataset KS01HN – 2001 Resident Population; available from: http://neighbourhood.statistics.gov.uk/Downloads.asp?nsid=false&CE=True&SE=True&T=D&dsid=4726). The formula to calculate the number of dentists per 1,000 for a given PCT/LHB is: (1000 * dentists count in the PCT or LHB/2001 Census population for that PCT or LHB).
The geographic analysis was done in ESRI ArcView GIS Version 3.1 http://www.esri.com/ and exactly the same results were reproduced in MapInfo v7.5 http://www.mapinfo.com/. We used the 2001 Census PCT (post April 2002 change) and LHB (post April 2003 change) boundary datasets, which are the copyright of the Crown/Ordnance Survey http://www.ordsvy.gov.uk/, and are freely available in both ArcView and MapInfo formats to the UK academic community from EDINA UKBORDERS service with the support of the ESRC and JISC http://edina.ac.uk/ukborders/.
The online interactive maps were produced using the free light edition of Zebris WebView for ESRI ArcView GIS 3.x (WebView LT – http://zebris-gis.de/english/main.htm). (Other options for generating more advanced Web maps from a desktop GIS are discussed in [27].)
Methodological issues: hue thresholding, data timeliness and boundary stability
It has been said that maps can lie. GIS integration of complex data into visually easy-to-understand pictures can sometimes be a setup for misunderstanding and misuse. It is therefore necessary that we design maps in such a way as to avoid drawing false conclusions from them [18].
When classifying data to create 'traffic light' maps, we need to decide on the number of classes to use (the minimum is three, corresponding to the three basic 'traffic light' hues: red, yellow and green; more than three classes can be defined and associated with additional shades/tints of the three basic hues). We also need to carefully choose the endpoints (cut-off points or hue thresholds) for our class intervals. The effects of changing the number of classes and hue thresholds of a 'traffic light' map can be dramatic, and may even convey very different interpretations of the same underlying data. In deciding on the number of classes to use in a 'traffic light' map and the associated cut-off points for class intervals, we should strive to neither raise false alarms nor overlook/miss areas of concern on the resultant map. Establishing appropriate criteria for NHS dental shortage area designation thus becomes extremely important. Of relevance in this context are the criteria set by the US Health Resources and Services Administration (HRSA)–Bureau of Health Professions for the designation of areas having shortages of dental professionals [32]. One of these criteria is 5000:1 population to dentist ratio or 0.2 dentist per 1,000 people, which corresponds to the lowest category presented on the more detailed maps in our study (Figures 4, 6).
If we were to repeat this study in two years (i.e., in 2006), we would need updated PCT/LHB population figures (or estimates, if we have reliable inter-census population growth/decline rate figures for different regions) to care for local population growth/decline in different PCTs/LHBs since 2001 Census.
Furthermore, the stability of administrative boundaries (PCT and LHB boundaries), of performance indicators and data definitions, and of classifications used in producing 'traffic light' maps are all necessary for carrying out appropriate performance monitoring and comparisons over time.
Authors' contributions
Both authors contributed equally to this work, and read and approved the final manuscript.
Supplementary Material
Dentists distribution datasets for England and Wales (Excel Workbook). Datasets of dentists distribution per 1,000 population in England (by PCT, as at 31 December 2002) and Wales (by LHB, as at 26 February 2004) that were used in producing maps in this study. For each PCT/LHB, the corresponding Census 2001 population figure and number of dentists are also included. Format: Microsoft Excel Workbook (England and Wales datasets are on two separate sheets in the workbook).
Acknowledgments
Acknowledgements
The authors would like to thank Robert Bain, Information Development Analyst, Dental Practice Board http://www.dpb.nhs.uk/gds/index.shtml, for providing us with the datasets of dentist numbers per PCT/LHB for England and Wales, which were used in this research.
Contributor Information
Maged N Kamel Boulos, Email: M.N.K.Boulos@bath.ac.uk.
Guy Picton Phillipps, Email: guy.picton-phillipps@brentpct.nhs.uk.
References
- General Dental Services in England and Wales (GDS) Statistics http://www.dpb.nhs.uk/gds/index.shtml
- Audit Commission: Dentistry – Primary dental care services in England and Wales http://www.audit-commission.gov.uk/reports/NATIONAL-REPORT.asp?ProdID=2D847593-050A-427d-B31B-C0A4683939AA
- What happened to NHS dentistry? (19 February 2004) http://news.bbc.co.uk/1/hi/magazine/3502813.stm
- Millions miss out on NHS dentists (18 February 2004) http://news.bbc.co.uk/1/hi/health/3499215.stm
- Hundreds queue for NHS dentists (16 February 2004) http://news.bbc.co.uk/1/hi/england/north_yorkshire/3494409.stm
- Why there is a shortage of NHS dentists (30 July 2003) http://news.bbc.co.uk/1/hi/health/3109915.stm
- Dentist shortage – hundreds queue (28 July 2003) http://news.bbc.co.uk/1/hi/wales/south_west/3102641.stm
- Less than half have NHS dentists (11 April 2003) http://news.bbc.co.uk/1/hi/health/2935611.stm
- Dentists 'stressed to limit' (25 March 2003) http://news.bbc.co.uk/1/hi/wales/2882909.stm
- Dentists' private income soars (6 January 2003) http://news.bbc.co.uk/1/hi/health/2625845.stm
- GDPA Media Release (28 November 2003): 90 per cent of dentists will quit NHS http://www.gdpa.org.uk/docs/Media%20Release%2031128%20Survey.pdf
- National Statistics Online: Population estimates http://www.statistics.gov.uk/cci/nugget.asp?id=6
- National Statistics Online: Health and personal social services: workforce summary, 1993–2002 http://www.statistics.gov.uk/STATBASE/ssdataset.asp?vlnk=3982
- South Korean Ministry of Health and Welfare – Health Guide: Number of practising dentists per 1,000 population in different countries: 1960–1997 (source: OECD Health Data, 1998) http://healthguide.kihasa.re.kr/eng/statistics/sts100028.html
- Higgs G, Richards W. The use of geographical information systems in examining variations in sociodemographic profiles of dental practice catchments: a case study of a Swansea practice. Prim Dent Care. 2002;9:63–9. doi: 10.1308/135576102322527829. [DOI] [PubMed] [Google Scholar]
- Dental Practice Board http://www.dpb.nhs.uk/
- £65.2 M to improve dental care for NHS patients http://www.dh.gov.uk/PublicationsAndStatistics/PressReleases/PressReleasesNotices/fs/en?CONTENT_ID=4054268&chk=mlfcsb
- Boulos MN. Towards evidence-based, GIS-driven national spatial health information infrastructure and surveillance services in the United Kingdom. Int J Health Geogr. 2004;3:1. doi: 10.1186/1476-072X-3-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White DA, Anderson RJ, Bradnock G, Gray MM, Jenkins P. The use of a geographical information system in investigating dental services. Community Dent Health. 2000;17:79–84. [PubMed] [Google Scholar]
- Susi L, Mascarenhas AK. Using a geographical information system to map the distribution of dentists in Ohio. J Am Dent Assoc. 2002;133:636–42. doi: 10.14219/jada.archive.2002.0239. [DOI] [PubMed] [Google Scholar]
- Kelly V, Murekezi A. Fertilizer Response and Profitability in Rwanda: A Synthesis of Findings from MINAGRI Studies Conducted by the Food Security Research Project (FSRP) and the FAO Soil Fertility Initiative Kigali, Rwanda: FSRP, MINAGRI/DSA. 2000. http://www.aec.msu.edu/agecon/fs2/Rwanda/fertilizer.pdf
- Kaufmann D, Kraay A, Mastruzzi M. Governance Matters III: Governance Indicators for 1996–2002 World Bank Policy Research Working Paper 3106 Washington, DC: World Bank Institute. 2003. http://www.worldbank.org/wbi/governance/pubs/govmatters3.html
- Wagner MM, Robinson JM, Tsui FC, Espino JU, Hogan WR. Design of a national retail data monitor for public health surveillance. J Am Med Inform Assoc. 2003;10:409–18. doi: 10.1197/jamia.M1357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Department of Homeland Security – Homeland Security Advisory System http://www.dhs.gov/dhspublic/display?theme=29
- House of Commons Hansard Written Answers for 24 Apr 2002 (pt 27) http://www.parliament.the-stationery-office.co.uk/pa/cm200102/cmhansrd/vo020424/text/20424w27.htm
- GDS dentists, principal dentists and vocational dental practitioners in England and Wales by quarter http://www.dpb.nhs.uk/gds/data/gds_dentists.htm
- Boulos MNK, Roudsari AV, Carson ER. A simple method for serving Web hypermaps with dynamic database drill-down. Int J Health Geogr. 2002;1 doi: 10.1186/1476-072X-1-1. http://www.ij-healthgeographics.com/content/1/1/1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Griffin SO, Gooch BF, Beltran E, Sutherland JN, Barsley R. Dental services, costs, and factors associated with hospitalization for Medicaid-eligible children, Louisiana 1996–97. J Public Health Dent. 2000;60:21–7. doi: 10.1111/j.1752-7325.2000.tb03287.x. [DOI] [PubMed] [Google Scholar]
- Mayer ML, Stearns SC, Norton EC, Rozier RG. The effects of Medicaid expansions and reimbursement increases on dentists' participation. Inquiry. 2000;37:33–44. [PubMed] [Google Scholar]
- General Dental Council Annual Report 2002–3 http://www.gdc-uk.org/GDC_Annual_Report.pdf
- Total number of UK dental graduates has been declining in the last decade http://www.scotland.gov.uk/library3/health/sacd-17.asp#f9
- Health Professional Shortage Area – Dental Designation Criteria (US) http://www.bhpr.hrsa.gov/shortage/hpsacritdental.htm
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Dentists distribution datasets for England and Wales (Excel Workbook). Datasets of dentists distribution per 1,000 population in England (by PCT, as at 31 December 2002) and Wales (by LHB, as at 26 February 2004) that were used in producing maps in this study. For each PCT/LHB, the corresponding Census 2001 population figure and number of dentists are also included. Format: Microsoft Excel Workbook (England and Wales datasets are on two separate sheets in the workbook).