

Abstract
Objective
Because of the complex anatomical association among vascular, dural, and bony structures, paraclinoid internal carotid artery (ICA) aneurysms remain a major challenge for vascular neurosurgeons. We studied the clinical outcomes of 61 paraclinoid ICA aneurysms after microsurgical clipping in comparison with endovascular coiling.
Materials and Methods
Between January 2008 and December 2012, we treated 61 paraclinoid ICA aneurysms created by surgical clipping or endovascular coiling. Preoperative neurologic status and postoperative outcome were evaluated using the Glasgow coma scale (GCS) and the modified Rankin scale (mRS). Postoperative hydrocephalus and vasospasm were reviewed using the patients' medical charts.
Results
Most patients were in good clinical condition before the operations and had good treatment outcomes. Clinical vasospasm was observed after the operation in five patients, and hydrocephalus occurred in six patients. No statistically significant difference regarding aneurysm size, sex, GCS score, H-H grade, and mRS was observed between the surgical clipping group and the endovascular coiling group. In addition, the treatment results and complications did not show statistically significant difference in either group.
Conclusion
Surgical occlusion of paraclinoid ICA aneurysms is difficult; however, no significant differences were observed in the treatment results or complications when compared with coil embolization. In particular, use of an adequate surgical technique may lead to better outcomes than those for coil embolization in the treatment of large and/or wide-neck paraclinoid ICA aneurysms.
Keywords: Paraclinoid aneurysms, Microsurgical clipping, Endovascular coiling, Outcome
INTRODUCTION
Aneurysms arising from the segment of the internal carotid artery (ICA) between the proximal dural ring and the origin of the posterior communicating artery (PCoA) constitute paraclinoid aneurysms.19),20),25) Nutik coined the term "paraclinoid aneurysm" to describe aneurysms arising from the ICA opposite the origin of the ophthalmic artery.25)
Paraclinoid aneurysms are mainly intradural and therefore are associated with a potential risk of subarachnoid hemorrhage (SAH). They are frequently large or giant and have a common close relationship with the bone of the skull base and with the dural folds around the ICA. Because of the complex anatomical relationship among neurovascular, dural, and bony structures, management of paraclinoid aneurysms is more challenging compared with intracranial aneurysms at other locations.6)
Advances in surgical techniques and cranial base approaches have resulted in significantly improved surgical outcomes for paraclinoid aneurysms.7) In addition, endovascular procedures have become the second choice management modality.20),27),32)
In this retrospective review, we analyzed the results of microsurgical treatment of paraclinoid ICA aneurysms managed in our institution from 2008 to 2012 by comparing them with the results of endovascular embolization.
MATERIALS AND METHODS
Sixty one patients with paraclinoid ICA aneurysms underwent surgical clipping or endovascular coil embolization between January 2008 and December 2012. We obtained patients' clinical information from their medical charts and reviewed their preoperative and postoperative images. Preoperative neurologic status and postoperative outcome were evaluated according to the Glasgow coma scale (GCS) and the modified Rankin scale (mRS) six months after treatment, respectively. The medical records were also reviewed for history of intervening hydrocephalus and vasospasm. All patients underwent computed tomographic (CT) angiography or digital subtraction angiography (DSA) before the operation, and actual aneurysm morphometry was measured.
Microsurgical treatment
Initially, all patients underwent neck dissection in order to expose the cervical ICA. The orbito-zygomatic approach (OZA) was used in most patients. The anterior clinoid process (ACP) was removed extradurally and/or intradurally, and the sphenoid ridge was flattened until the lateral edge of the superior orbital fissure (SOF) was reached. The roof of the optic canal and most of the optic strut was removed for adequate exposure of the proximal neck of the aneurysm and for intracranial proximal control of the ICA. All paraclinoid ICA aneurysms were completely obliterated by direct clipping without bypass. Microsurgical clipping was considered if preoperative angiogram showed that the ophthalmic artery was incorporated from the aneurysm neck, aneurysm had a broad-neck, or if an endovascular approach was otherwise technically not feasible.
Endovascular treatment
All procedures were performed under general anesthesia. Heparinization was only started in unruptured aneurysms with a loading dose of 3000 IU and was maintained with a dose of 1000 IU on an hourly basis after femoral puncture and femoral sheath placement. Using a guiding catheter, microcatheters with proper shapes were introduced over micro-guidewires and navigated into the aneurysms. Aneurysms were packed as densely as possible with coils. In wide-neck aneurysms, multiple catheters, balloons, or stents were used for safe coil deployment. Immediate postoperative and follow up angiographic results were classified as total occlusion, neck remnant, and body filling.31) Endovascular treatment was recommended for patients with significant medical comorbidities or age > 75 years. In this situation, if the aneurysm was amendable to both surgical clipping and endovascular treatment, endovascular treatment was considered under agreement from the patients or their relatives.
Statistical analysis
The Wilcoxon rank sum test and Fisher's exact test were used for analysis of differences between the two groups. A p value < 0.05 was considered significant. Analyses were performed using statistical analysis system version 9.2 (SAS Institute Inc., Cary, NC, United States).
RESULTS
A total of 61 patients underwent surgical clipping or endovascular coil embolization. Of these, 30 aneurysms were clipped, and the remaining ones were embolized. Among them, 52 patients were female and nine patients were male. The mean age was 54 years (27-81 years). The mean aneurysm diameter was 6.5 mm in the greatest dimension. Forty five patients had small aneurysms (< 7 mm), eight patients had medium (7-12 mm), seven patients had large (13-24 mm), and one patient had a giant (≥ 25 mm) aneurysm (Table 1). Twelve patients had a subarachnoid hemorrhage (SAH) due to aneurysm rupture. In patients with unruptured aneurysms, initial symptoms were headache (n = 46), decreased visual acuity (n = 2), and cavernous sinus syndrome (n = 1). Most patients were in good clinical condition before the operation and had favorable outcomes. Five patients suffered vasospasm, and six patients showed hydrocephalus after surgical clipping (Table 1).
Table 1.
Characteristics of patients with paraclinoid ICA aneurysms
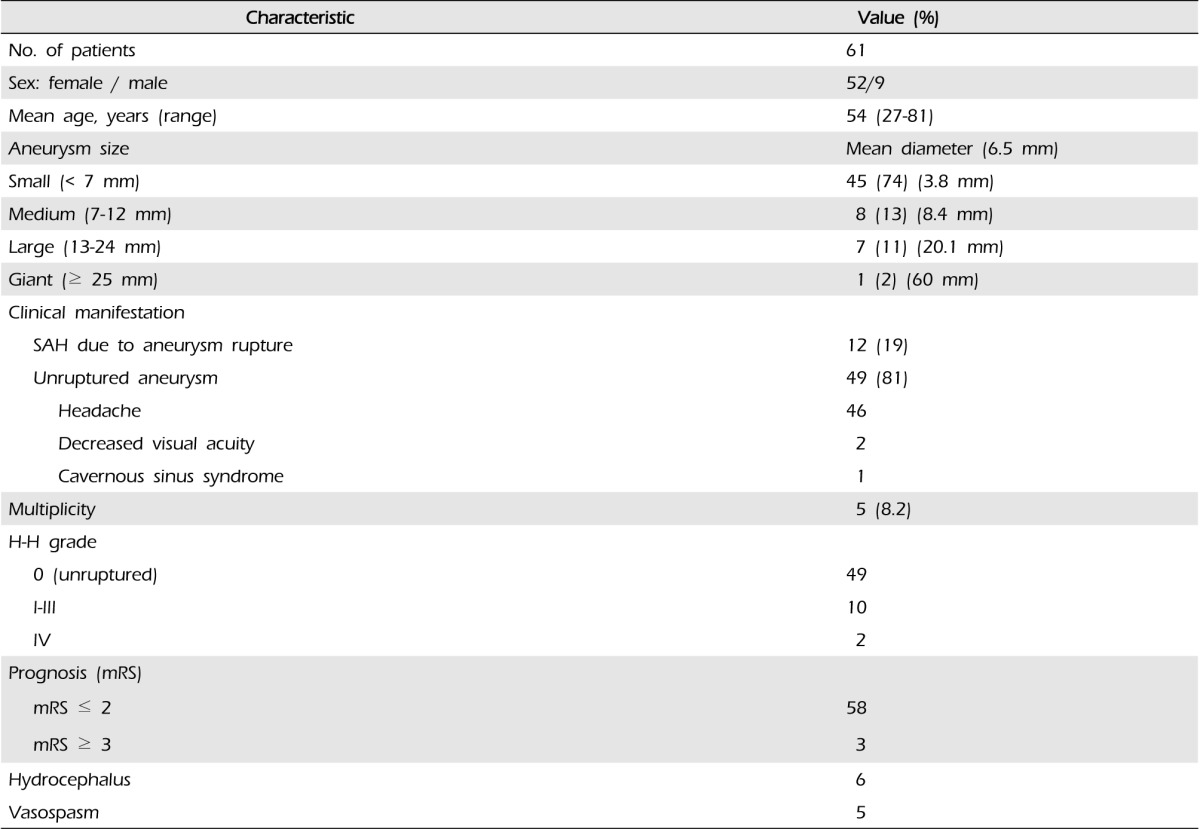
mRS= modified Rankin scale; H-H = Hunt-Hess classification; SAH = subarachnoid hemorrhage; ICA = internal carotid artery
Surgical clipping group
In the clipping group, the mean age was 49.77 ± 10.84 years, and the mean aneurysm diameter was 6.17 ± 5.09 mm in the greatest dimension (range 3-20 mm), except one patient with a giant aneurysm of 60 mm in the greatest dimension. Twenty four patients were female, and six patients were male. SAH with a ruptured paraclinoid ICA aneurysm was observed in 11 patients. Except for two patients, the initial neurologic examination showed a favorable clinical state (mean GCS was 14.43 ± 1.48) in 28 patients. After surgical clipping in 30 cases, six patients had hydrocephalus, and five had vasospasm. Among six hydrocephalic patients, two cases of hydrocephalus occurred in unruptured cases. One showed obstructive hydrocephalus due to a giant aneurysm, and the other had communicating hydrocephalus due to previous SAH associated with anterior communicating artery aneurysm rupture. Transient hemiparesis and ptosis occurred in four patients, but showed spontaneous recovery within one month. One patient had permanent motor weakness, and two patients had permanent visual complications.
Endovascular coiling group
In the coiling group, the mean age was 58.16 ± 10.61 years, and the mean aneurysm diameter was 5.45 ± 2.50 mm (ranged 3-13 mm). Twenty eight patients were female, and their mean GCS was 14.90 ± 0.30. Only one patient had SAH due to a ruptured aneurysm. After endovascular coil embolization, none of the patients had hydrocephalus or vasospasm (Table 2). Cerebellar hemorrhage was found in one patient, which resolved without neurological sequelae. Two patients had transient hemiparesis.
Table 2.
Comparison of characteristics and clinical outcomes between the surgical clipping and endovascular coiling groups
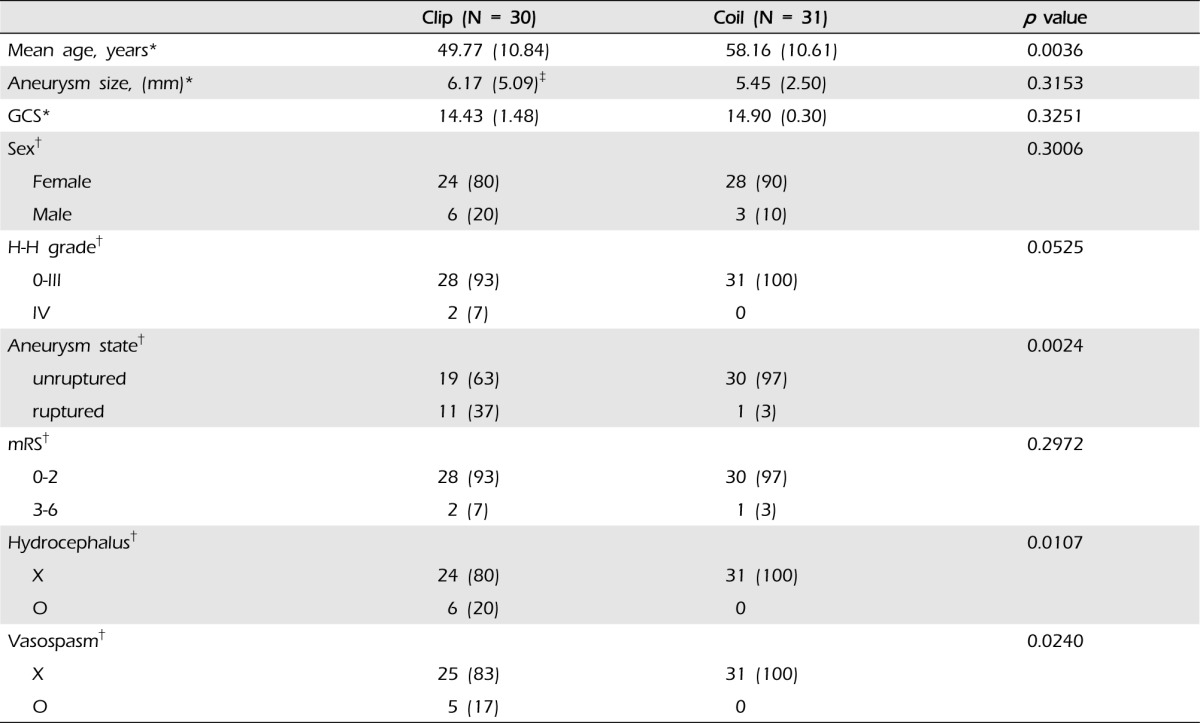
*Wilcoxon rank sum test, Mean (SD), p < 0.05, †Fisher's exact test, N (%), p < 0.05, ‡Excluding one patient with an exceptionally large aneurysm diameter (60 mm)
GCS = Glasgow coma scale; mRS = modified Rankin scale; H-H = Hunt-Hess grade scale
No statistical significance regarding aneurysm size, sex, GCS score, H-H grade, and mRS was observed between the surgical clipping and endovascular coil groups (Table 2). However, this statistical comparison is not valuable, because only one patient with SAH underwent endovascular coiling. Therefore, because the clipping group did not reach a sufficient number for statistical analysis, we performed subgroup frequency analysis in unruptured aneurysm cases (Table 3).
Table 3.
Subgroup analysis between the surgical clipping and endovascular coiling group in unruptured aneurysms
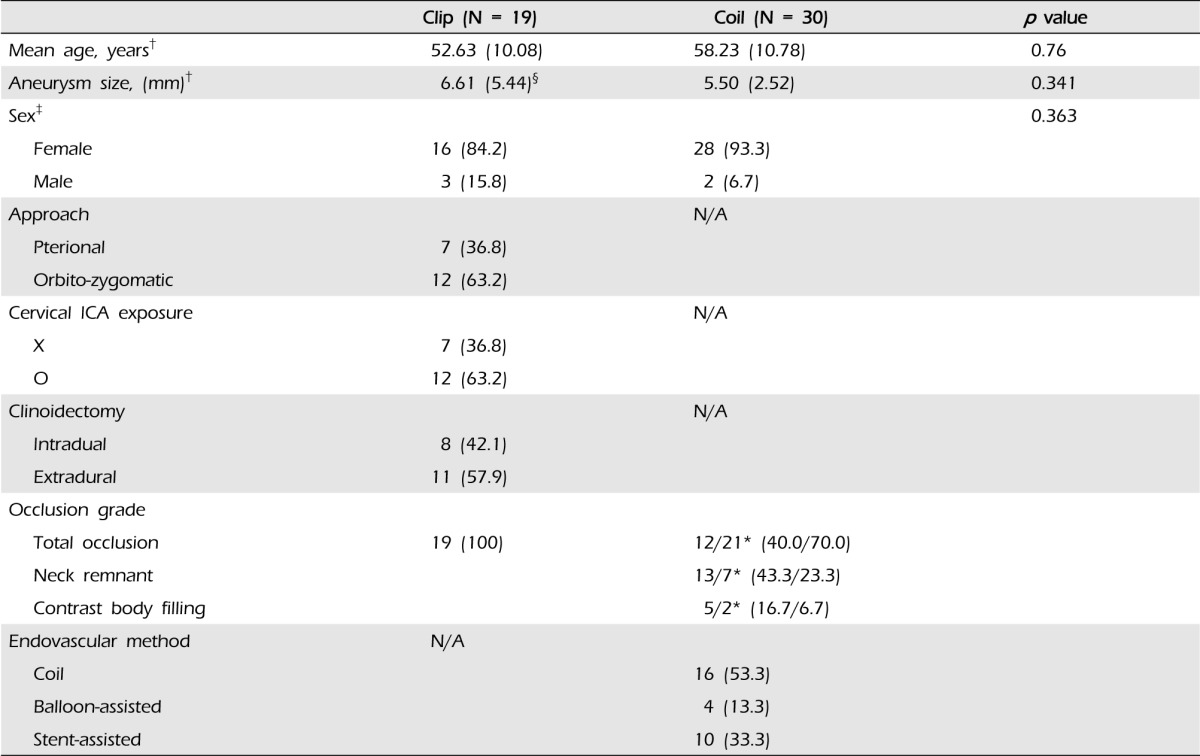
*Immediate/one-year follow up, †Wilcoxon rank sum test, Mean (SD), p < 0.05, ‡Fisher's exact test, N. (%), p < 0.05, §Excluding one patient with an exceptionally large aneurysm diameter (60 mm).
N/A = not applicable
Among 61 patients, two patients died after either surgical clipping or endovascular coiling. One patient was a 58-year-old woman who had an unruptured paraclinoid ICA aneurysm and a superior cerebellar artery (SCA) aneurysm. Her GCS score was 15, and the paraclinoid ICA aneurysm measured 13 mm in its greatest dimension. Stent-assisted coil embolization was performed, and the patient recovered without neurological problems. The next day, the patient was transferred to the general ward, however, sudden mental deterioration was observed seven days after embolization. Follow-up brain CT was performed, and SAH with a massive ICH was detected in the left cerebellar hemisphere. Because of antiplatelet agent usage, the amount of hematoma was much greater than expected. Her family members refused further intervention, and she died nine days after embolization. Another patient, a 51-year-old female, suffered SAH due to rupture of a left ophthalmic artery aneurysm, with a GCS score of 9 and Fisher and H-H grades of IV. Emergent surgical clipping of the aneurysm and decompressive craniectomy were performed in order to relieve severe brain edema. She was treated in the intensive care unit with intracranial pressure (ICP) control, but brain edema and severe vasospasm progressed. She died eight days after surgery.
Illustrative cases
Case 1: Unruptured left giant posterior wall aneurysm
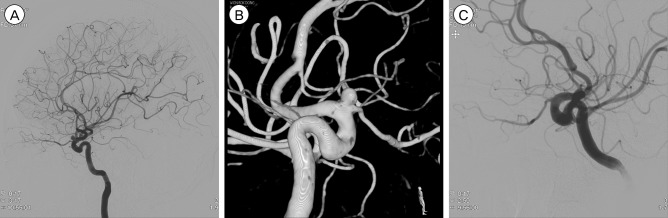
A 27-year-old female visited our hospital with abrupt occurrence of a left visual field defect. Neuro-ophthalmologic examination, including visual acuity by Snellen's chart, measured 0.1 in the right eye but showed blindness in the left. An aneurysm measuring 60 mm in its greatest dimension (Figs. 1. A-C) was identified. Using eight different types of fenestrated aneurysm clips, the giant aneurysm was directly occluded, and the supraclinoid ICA was reconstructed. Even though, no abnormal hypodense area was observed on the postoperative CT scans, the patient showed temporary right hemiparesis two days after surgery. Her right motor weakness resolved two days after hypervolemic and hypertensive therapy. A transient ischemia may have occurred due to temporary hypoperfusion, possibly associated with use of too many clips in ICA reconstruction. Postoperative DSA and CT angiography showed that the distal blood flow was preserved uneventfully (Figs. 1 D-F). The patient's left eye vision improved to a level that she could perceive hand movement 30 cm in front of her.
Fig. 1.

Preoperative left digital subtraction angiography (DSA) (A, B) representing a giant left internal carotid artery (ICA) posterior wall aneurysm. (A) Anteroposterior view. (B) Anterooblique view of three-dimensional (3-D) DSA. (C) 3-D computed tomographic (CT) angiography showing a giant sac adhering to all of the surrounding anterior and posterior cerebral arteries on both sides. Postoperative DSA (D, E) representing complete obliteration of the giant aneurysm sac and reconstruction of the ICA using eight different shapes of fenestrated clips. (D) Anteroposterior view (E) Lateral view of 3-D DSA. (F) Postoperative 3-D CT angiography.
Case 2: Unruptured left ophthalmic artery aneurysm
A 52-year-old female visited our hospital with complaints of intermittent headache and dizziness. An aneurysm at the ophthalmic segment measuring 4.5 mm in its greatest dimension was observed on digital subtraction angiography (DSA) (Figs. 2. A, B), however, ophthalmic examination did not uncover any abnormal findings. The patient underwent uneventful coil embolization without stent deployment. After embolization, the patient was discharged without symptoms or complications, and she noticed alleviation of her previous symptoms. Post-embolization DSA showed (Fig. 2. C) that the distal flow of the left ophthalmic artery was preserved, and the aneurysm sac was not filled with contrast medium.
Fig. 2.
Preoperative left digital subtraction angiography (DSA) (A, B) representing a left ophthalmic artery aneurysm. (A) Lateral view. (B) Lateral view of 3-D DSA. (C) Lateral view. Coil embolization was performed without using a stent. Postoperative left DSA (C) representing complete coil packing of the left ophthalmic artery aneurysm and showing that left ophthalmic artery flow was well preserved.
DISCUSSION
Within the paraclinoid segment, aneurysms can arise at various sites, including the ophthalmic artery, superior hypophyseal artery, carotid cave, and posterior carotid wall.27) Aneurysms in this location are usually challenging to surgeons. Refining of surgical techniques since the 1990s has led to significantly improved results of surgical clipping of paraclinoid ICA aneurysms.2),4),6),8),13),15),28)
Surgical treatment
Paraclinoid ICA aneurysms have imposed a significant technical burden on neurovascular surgeons. If possible, direct obliteration of the aneurysm is the most preferable treatment available. Before the development of microsurgical cranial base approaches, the ACP hindered the surgeon's view and thus restricted the angle of attack used in treatment of the aneurysm. Removal of the ACP allows for at least 6 mm of additional exposure of the distal ICA without entering the true CS.26) This technique has improved the approach to paraclinoid ICA aneurysms for direct surgical clipping.
Paraclinoid ICA aneurysms have different anatomical relationships with the dural folds and bony part of the cranial base and their surgical treatment requires specific surgical techniques such as exposure of the ICA in the neck, extra- and intradural ACP resection, ICA exposure of the clinoidal segment, opening of the distal dural ring, and hemostasis on the CS.5)
Raco et al., who studied the long-term efficacy of surgical clipping in treatment of ophthalmic segment aneurysms, 28) reported that clipping is a complete treatment for ophthalmic segment aneurysms with an acceptable morbidity rate (5.8%). In other literature, favorable outcomes (grades 4 and 5 of the GOS) ranging from 58.7% to 96.4% have been reported for surgical treatment of paraclinoid ICA aneurysms.1,2),3),6),8),9),12),15),16),18),22),24) The outcome in the current series was comparable to that reported in the published data. The results did not show a statistically significant difference when compared with the coil embolization group (Table 2).
Endovascular treatment
Because of the complex anatomy around the aneurysms and the characteristic risks associated with microsurgery, endovascular techniques have been popularized for treatment of paraclinoid ICA aneurysms.10),14),17),30),33) Endovascular embolization for paraclinoid ICA aneurysms has emerged as a major therapeutic option in selected patients, with comparable morbidity and mortality rates to surgery, as well as markedly reduced hospital stays.26),36)
Endovascular treatment is specifically suited for patients with the following conditions: a high medical risk for surgical clipping, worsening clinical grade, an aneurysm with no mass effect to be relieved or extension deep into the cavernous sinus, vasospasm before diagnostic angiography, and those who choose endovascular treatment.5),34) In this study, a statistically significant difference in age was observed between the clipping and coiling groups, which, as mentioned earlier, is expected due to the increased surgical risk associated with old age. In addition, it is also the reason that most elderly people are reluctant to undergo open surgery.
In a previous study, transient morbidity ranged from 0% to 4.8%, and permanent morbidity ranged from 0% to 3.5%.11),21),23),35) In the current study, most patients had good outcomes (97% with grades 0 to 2 of the mRS). However, for large or giant paraclinoid ICA aneurysms, dense coiling is difficult to achieve and can result in recanalization of the aneurysm. Aneurysm size larger than 10 mm is a significant predictor of recurrence, and, therefore, long-term angiographic follow-up is mandatory.29)
Complications
Overall transient or permanent postoperative complications have been reported at rates between 21.3% and 41.7% for surgical treatment of paraclinoid ICA aneurysms and from 27.3% to 50.0% for patients with giant aneurysms.1),6),8),9),15),18),22),24) The most frequent postoperative deficits or worsening status reported in the literature are attributed to compromise of the optic and oculomotor nerves. These complications are rarely seen in coil embolization; therefore, these low complications might be one of the advantages of coil embolization. Colli et al. reported vasospasm in 20.1% of patients with ruptured aneurysms and hydrocephalus in 4.8%.5) In this literature, routine opening of the lamina terminalis in aneurysm surgery might be attributed in part to the relatively low incidence of hydrocephalus.5)
In the current study, vasospasm (17%) and hydrocephalus (20%) were observed only in the clipping group. A statistically significant difference was observed between the clipping and coiling groups, however, it was believed to result from the discrepancy in the number of patients with aneurysm rupture in each group. In the clipping group, 11 of the 30 patients had ruptured aneurysms, but only one of 31 patients in the coiling group had a ruptured aneurysm. In this study, the clinical outcomes of microsurgical clipping for large or giant paraclinoid ICA aneurysms were favorable. Therefore, microsurgical clipping can be considered as the first-line treatment option in the case of large and/or broad-neck paraclinoid ICA aneurysms.
Limitations and future perspectives
First, the percentage of patients with ruptured aneurysms differed significantly between the groups, which might indicate a selection bias. Second, if we further divide patients based on location of the aneurysm, information about complications would provide more comprehensive data. Finally, future studies should include long-term, prospective allocation of all the available data in order to overcome the shortcomings encountered in the current study.
CONCLUSION
It is true that, when compared with aneurysm surgery at other locations, the complex anatomy of the paraclinoid ICA complicates the surgical management of aneurysms arising from this segment; however, in this study, when compared with coil embolization, the treatment results and complications did not differ significantly. In particular, if surgeons have adequate surgical experience and facilities, surgical outcomes may be better than those for coil embolization in treatment of large/giant or wide-neck paraclinoid ICA aneurysms. In order to achieve improved results, additional research on surgical techniques is needed.
Footnotes
There is neither financial support in any way nor any conflicts of interest in this manuscript.
References
- 1.Arnautovic KI, Al-Mefty O, Angtuaco E. A combined microsurgical skull-base and endovascular approach to giant and large paraclinoid aneurysms. Surg Neurol. 1998 Dec;50(6):504–518. doi: 10.1016/s0090-3019(97)80415-6. discussion 518-20. [DOI] [PubMed] [Google Scholar]
- 2.Barami K, Hernandez VS, Diaz FG, Guthikonda M. Paraclinoid carotid aneurysms: surgical management, complications, and outcome based on a new classification scheme. Skull base. 2003 Feb;13(1):31–41. doi: 10.1055/s-2003-820555. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Batjer HH, Kopitnik TA, Giller CA, Samson DS. Surgery for paraclinoid aneurysms. J Neurosurg. 1994 Apr;80(4):650–658. doi: 10.3171/jns.1994.80.4.0650. [DOI] [PubMed] [Google Scholar]
- 4.Beretta F, Andaluz N, Zuccarello M. Aneurysms of the ophthalmic (C6) segment of the internal carotid artery: treatment options and strategies based on a clinical series. J Neurosurg Sci. 2004 Dec;48(4):149–156. [PubMed] [Google Scholar]
- 5.Colli BO, Carlotti CG, Jr, Assirati JA, Jr, Abud DG, Amato MC, Dezena RA. Results of microsurgical treatment of paraclinoid carotid aneurysms. Neurosurg Rev. 2013 Jan;36(1):99–114. doi: 10.1007/s10143-012-0415-0. [DOI] [PubMed] [Google Scholar]
- 6.De Jesus O, Sekhar LN, Riedel CJ. Clinoid and paraclinoid aneurysms: surgical anatomy, operative techniques, and outcome. Surg Neurol. 1999 May;51(5):477–487. doi: 10.1016/s0090-3019(98)00137-2. discussion 487-8. [DOI] [PubMed] [Google Scholar]
- 7.Dolenc VV. A combined transorbital-transclinoid and transsylvian approach to carotid-ophthalmic aneurysms without retraction of the brain. Acta Neurochir Suppl. 1999;72:89–97. doi: 10.1007/978-3-7091-6377-1_8. [DOI] [PubMed] [Google Scholar]
- 8.Day AL. Aneurysms of the ophthalmic segment. A clinical and anatomical analysis. J Neurosurg. 1990 May;72(5):677–691. doi: 10.3171/jns.1990.72.5.0677. [DOI] [PubMed] [Google Scholar]
- 9.Eliava SS, Filatov YM, Yakovlev SB, Shekhtman OD, Kheireddin AS, Sazonov IA, et al. Results of microsurgical treatment of large and giant ICA aneurysms using the retrograde suction decompression (RSD) technique: series of 92 patients. World Neurosurg. 2010 Jun;73(6):683–687. doi: 10.1016/j.wneu.2010.03.017. [DOI] [PubMed] [Google Scholar]
- 10.Fernandez Zubillaga A, Guglielmi G, Vinuela F, Duckwiler GR. Endovascular occlusion of intracranial aneurysms with electrically detachable coils: correlation of aneurysm neck size and treatment results. AJNR Am J Neuroradiol. 1994 May;15(5):815–820. [PMC free article] [PubMed] [Google Scholar]
- 11.Ferrell AS, Lessne ML, Alexander MJ, Shah P, Golshani K, Zomorodi A, et al. Visual complications after stent-assisted endovascular embolization of paraophthalmic and suprasellar variant superior hypophyseal aneurysms: the Duke cerebrovascular center experience in 57 patients. World Neurosurg. 2012 Sep-Oct;78(3-4):289–294. doi: 10.1016/j.wneu.2011.12.003. [DOI] [PubMed] [Google Scholar]
- 12.Fulkerson DH, Horner TG, Payner TD, Leipziq TJ, Scott JA, Denardo AJ, et al. Endovascular retrograde suction decompression as an adjunct to surgical treatment of ophthalmic aneurysms: analysis of risks and clinical outcomes. Neurosurgery. 2009 Mar;64(3 Suppl):ons107–ons111. doi: 10.1227/01.NEU.0000330391.20750.71. discussion ons111-2. [DOI] [PubMed] [Google Scholar]
- 13.Giannotta SL. Ophthalmic segment aneurysm surgery. Neurosurgery. 2002 Mar;50(3):558–562. doi: 10.1097/00006123-200203000-00025. [DOI] [PubMed] [Google Scholar]
- 14.Heran NS, Song JK, Kupersmith MJ, Niimi Y, Namba K, Langer DJ, et al. Large ophthalmic segment aneurysms with anterior optic pathway compression: assessment of anatomical and visual outcomes after endovascular coil therapy. J Neurosurg. 2007 Jun;106(6):968–975. doi: 10.3171/jns.2007.106.6.968. [DOI] [PubMed] [Google Scholar]
- 15.Hoh BL, Carter BS, Budzik RF, Putman CM, Ogilvy CS. Results after surgical and endovascular treatment of paraclinoid aneurysms by a combined neurovascular team. Neurosurgery. 2001 Jan;48(1):78–90. doi: 10.1097/00006123-200101000-00014. discussion 89-90. [DOI] [PubMed] [Google Scholar]
- 16.Iihara K, Murao K, Sakai N, Shindo A, Sakai H, Higashi T, et al. Unruptured paraclinoid aneurysms: a management strategy. J Neurosurg. 2003 Aug;99(2):241–247. doi: 10.3171/jns.2003.99.2.0241. [DOI] [PubMed] [Google Scholar]
- 17.Jin SC, Kwon DH, Ahn JS, Kwun BD, Song Y, Choi CG. Clinical and radiological outcomes of endovascular detachable coil embolization in paraclinoid aneurysms: a 10-year experience. J Korean Neurosurg Soc. 2009 Jan;45(1):5–10. doi: 10.3340/jkns.2009.45.1.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Khan N, Yoshimura S, Roth P, Cesnulis E, Koenue-Leblebicioglu D, Curcic M, et al. Conventional microsurgical treatment of paraclinoid aneurysms: state of the art with the use of the selective extradural anterior clinoidectomy SEAC. Acta Neurochir Suppl. 2005;94:23–29. doi: 10.1007/3-211-27911-3_5. [DOI] [PubMed] [Google Scholar]
- 19.Kim JM, Romano A, Sanan A, van Loveren HR, Keller JT. Microsurgical anatomic features and nomenclature of the paraclinoid region. Neurosurgery. 2000 Mar;46(3):670–680. doi: 10.1097/00006123-200003000-00029. discussion 680-2. [DOI] [PubMed] [Google Scholar]
- 20.Kolasa PP, Kaurzel Z, Lewinski A. Treatment of giant paraclinoid aneurysms. Own experience. Neuro Endocrinol Lett. 2004 Aug;25(4):287–291. [PubMed] [Google Scholar]
- 21.Kwon BJ, Im SH, Park JC, Cho YD, Kang HS, Kim JE, et al. Shaping and navigating methods of microcatheters for endovascular treatment of paraclinoid aneurysms. Neurosurgery. 2010 Jul;67(1):34–40. doi: 10.1227/01.NEU.0000370891.67129.2F. discussion 40. [DOI] [PubMed] [Google Scholar]
- 22.Liu Y, You C, He M, Cai BW. Microneurosurgical management of the clinoid and paraclinoid aneurysms. Neurol Res. 2008 Jul;30(6):552–556. doi: 10.1179/174313208X298101. [DOI] [PubMed] [Google Scholar]
- 23.Loumiotis I, D'Urso PI, Tawk R, Cloft HJ, Kallmes DF, Kairouz V, et al. Endovascular treatment of ruptured paraclinoid aneurysms: results, complications, and follow-up. AJNR Am J Neuroradiol. 2012 Apr;33(4):632–637. doi: 10.3174/ajnr.A2825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Morgan MK, Efkhar B. Commentary: paraclinoid carotid aneurysms. J Clin Neurosci. 2011 Jan;18(1):23. doi: 10.1016/j.jocn.2010.07.123. [DOI] [PubMed] [Google Scholar]
- 25.Nutik S. Carotid paraclinoid aneurysms with intradural origin and intracavernous location. J Neurosurg. 1978 Apr;48(4):526–533. doi: 10.3171/jns.1978.48.4.0526. [DOI] [PubMed] [Google Scholar]
- 26.Nutik SL. Removal of the anterior clinoid process for exposure of the proximal intracranial carotid artery. J Neurosurg. 1988 Oct;69(4):529–534. doi: 10.3171/jns.1988.69.4.0529. [DOI] [PubMed] [Google Scholar]
- 27.Ogilvy CS. Paraclinoid carotid aneurysms. In: Ojemann RG, Ogilvy CS, Crowell RM, Heros RC, editors. Surgical management of neurovascular disease. 3rd ed. Baltimore: Williams & Wilkins; 1995. pp. 185–213. [Google Scholar]
- 28.Raco A, Frati A, Santoro A, Vangelista T, Salvati M, Delfini R, et al. Long-term surgical results with aneurysms involving the ophthalmic segment of the carotid artery. J Neurosurg. 2008 Jun;108(6):1200–1210. doi: 10.3171/JNS/2008/108/6/1200. [DOI] [PubMed] [Google Scholar]
- 29.Raymond J, Guilbert F, Weill A, Georganos SA, Juravsky L, Lambert A, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke. 2003 Jun;34(6):1398–1403. doi: 10.1161/01.STR.0000073841.88563.E9. [DOI] [PubMed] [Google Scholar]
- 30.Park HK, Horowitz M, Jungreis C, Kassam A, Koebbe C, Genevro J, et al. Endovascular treatment of paraclinoid aneurysms: experience with 73 patients. Neurosurgery. 2003 Jul;53(1):14–23. doi: 10.1227/01.neu.0000068789.08955.1c. discussion 24. [DOI] [PubMed] [Google Scholar]
- 31.Roy D, Milot G, Raymond J. Endovascular treatment of unruptured aneurysms. Stroke. 2001 Sep;32(9):1998–2004. doi: 10.1161/hs0901.095600. [DOI] [PubMed] [Google Scholar]
- 32.Roy D, Raymond J, Bouthillier A, Bojanowski MW, Moumdjian R, L'Esperance G. Endovascular treatment of ophthalmic segment aneurysms with Guglielmi detachable coils. AJNR Am J Neuroradiol. 1997 Aug;18(7):1207–1215. [PMC free article] [PubMed] [Google Scholar]
- 33.Thornton J, Aletich VA, Debrun GM, Alazzaz A, Misra M, Charbel F, et al. Endovascular treatment of paraclinoid aneurysms. Surg Neurol. 2000 Oct;54(4):288–299. doi: 10.1016/s0090-3019(00)00313-x. [DOI] [PubMed] [Google Scholar]
- 34.Xu BN, Sun ZH, Romani R, Jiang JL, Wu C, Zhou DB, et al. Microsurgical management of large and giant paraclinoid aneurysms. World Neurosurg. 2010 Mar;73(3):137–146. doi: 10.1016/j.surneu.2009.07.042. discussion e17, e19. [DOI] [PubMed] [Google Scholar]
- 35.Yadla S, Campbell PG, Grobelny B, Jallo J, Gonzalez LF, Rosenwasser RH, et al. Open and endovascular treatment of unruptured carotid-ophthalmic aneurysms: clinical and radiographic outcomes. Neurosurgery. 2011 May;68(5):1434–1443. doi: 10.1227/NEU.0b013e31820b4f85. discussion 1443. [DOI] [PubMed] [Google Scholar]
- 36.Zhao J, Wang S, Zhao Y, Sui D, Zhang Y, Tang J, et al. Microneurosurgical management of carotid-ophthalmic aneurysms. J Clin Neurosci. 2006 Apr;13(3):330–333. doi: 10.1016/j.jocn.2005.04.029. [DOI] [PubMed] [Google Scholar]