

Abstract
Liposarcoma is the most common soft tissue sarcoma and accounts for 15%-20% of all mesenchymal malignancies. The tumor occurs most frequently in the limbs, retroperitoneum and rarely has a visceral location. We report a case of a gastric liposarcoma in a male patient. A 68 years old male patient was admitted to hospital for abdominal discomfort and fullness lasting for a month. He reported rare episodes of vomiting. The CT examination revealed a large epigastric mass (8 cm x 4 cm) involving the lesser curvature of the stomach, in contact with the pancreas and gallbladder. Fatty areas within the mass were evident. A total gastrectomy together with cholecystectomy was performed. The histopathological diagnosis was a well differentiated liposarcoma. The patient did not undergo any adjuvant treatment, he is under close follow up and two years later he is disease free. We report this case due to the rarity of this tumor in the stomach (nine cases reported in the literature).
Keywords: Gastric liposarcoma, Lipoblasts, CT diagnosis, Total gastrectomy, Well-differentiated type
INTRODUCTION
Liposarcoma is a common soft tissue tumor occurring in 15%-20% of all patients with sarcoma. The hallmark of liposarcoma is the immature fat cells or lipoblasts. It is usually localized in the limbs, retroperitoneum and trunk. Viscera rarely are involved. Histologically, liposarcomas are subdivided into-differentiated, myxoid, round cell and pleomorphic[1] sarcomas. Gastric liposarcomas are very rare and only a few (nine) cases have been reported worldwide[2-4]. We report a case of a large epigastric mass proven to be a gastric liposarcoma.
CASE REPORT
A 68-year old male patient was admitted to the surgical ward with symptoms of abdominal pain and discomfort localized in the epigastrium during the last month. He reported rare episodes of vomiting and weight loss of more than 8 kg in that period. He had not any specific past medical history. At physical examination a palpable mass was found in the epigastrium and the right upper quadrant. Blood tests showed a mild leucocytosis and tumor marker values were normal. Plain abdominal X-ray showed no specific findings. Computed tomography (CT) examination revealed a large epigastric mass (9 cm × 4 cm) arising from the gastric fundus and protruding beyond the gastric wall, being in contact with the pancreas and gallbladder. Heterogeneous fatty density areas were demonstrated. No hepatic metastasis or nodal involvements were detected. An upper GI endoscopy revealed a mucosal lesion and the posterior gastric wall seemed to be compressed (Figure 1). The patient underwent a laparotomy. During laparotomy the pancreas was found to be free of tumor involvement and there were fibrous adhesions of the duodenum to the gallbladder. A total gastrectomy was carried out due to the size of the lesion in order to achieve negative margins, cholecystectom was also performed. Histopathological examination revealed a well-differentiated liposarcoma. The tumor was basically composed of mature adipocytes which varied in size and shape and had enlarged atypical hyper chromatic nuclei. Uni- and multivacuolated lipoblasts were sparsely distributed throughout the lesion. Mitotic activity was generally very low, ranging from 0 to 1 mitosis per 10 high-power fields (Figure 2).
Figure 1.
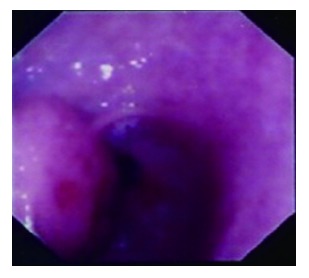
Upper GI endoscopy showing a mucosal lesion in the gastric antrum being suspected for lipomatous tumor.
Figure 2.
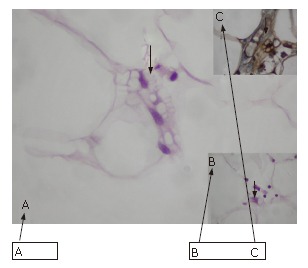
Multivacuolated (A) and univacuolated (B) lipoblasts as well as a multivacuolated lipoblast positive immunohistostain for S-100 protein (C).
The patient did not undergo any adjuvant treatment, he was under close follow-up including biannual CT scanning and upper GI endoscopy at the time we wrote our report and 2 years later he was disease free.
DISCUSSION
Liposarcoma is primarily a tumor in adults with a peak incidence between age 50 and 65. It is the most common soft tissue sarcoma appearing anywhere in the body. Gastric liposarcomas are extremely rare and characterized by an exophytic growth being adherent to the gastric wall. Its typical location is in the lesser curvature. Gastric liposarcomas originate due to proliferation of undifferentiated mesenchymal cells within the submucosa and the tunica muscularis layer of the stomach. As with other sarcomas there are no characteristic clinical findings[5].
Upper gastrointestinal series may support the diagnosis by the appearance of submucosal filling defects. Gastroscopy may sometimes reveal ulcerations[5]. The definite diagnosis is best established by CT examination. There is a strong correlation between CT and histopathological findings. Cytology has a value in diagnosis since in adipose tissue tumors with fat content less than 75% of the tumor volume, liposarcoma is the most likely diagnosis[6].
Histologically, there are four types of liposarcomas: well- differentiated, myxoid, round cell and pleomorphic. Well- differentiated liposarcomas account for 40% of all liposarcomas, having a peak incidence between the 5th and 7th decades. They are further subdivided into adipocytic, sclerosing, inflammatory and spindle cell subtypes[7]. Well- differentiated liposarcomas have a risk for local recurrence but no potential for metastasis. Myxoid liposarcomas are characterized by a myxoid matrix and considered to be low to intermediate grade lesions. In round cell type, there is an excessive proliferation of small rounded cells. Pleomorphic liposarcoma is a highly malignant lesion characterized by increased mitotic activity and hemorrhage as well as necrosis[8]. The term dedifferentiated liposarcoma has been used to refer to lesions that appear to begin as low-grade lesions but progress to high grade tumors and show evidence of nonlipogenic differentiation[9].
The relation between the histopathological type and CT findings is evident in such a way that well-differentiated liposarcomas show the classic heterogeneous density, myxoid type shows liquid cystic changes and round cell and pleomorphic types are characterized by a nonspecific solid structure[1,5].
Differential diagnosis of gastric liposarcoma includes peritoneal liposarcoma, carcinoma engulfing perivisceral fat, gastric stromal tumors, hepatic metastases adjacent to the stomach, peritoneal carcinomatosis, lymphoma and primary tumor of the omentum[10].
In conclusion, whenever a large exophytic mass originating from the gastric wall is revealed at computed tomography in the absence of secondary organ and peritoneal involvement. The diagnosis of a gastric liposarcoma should be considered, the treatment of choice is surgical removal.
Footnotes
S- Editor Zhu LH L- Editor Wang XL E- Editor Yin DH
References
- 1.Ferrozzi F, Bova D, Garlaschi G. Gastric liposarcoma: CT appearance. Abdom Imaging. 1993;18:232–233. doi: 10.1007/BF00198110. [DOI] [PubMed] [Google Scholar]
- 2.Orita K, Kokumai Y, Kawada K, Takagi S, Kawahara T. Liposarcoma of stomach: report of a case. Acta Med Okayama. 1968;22:167–173. [PubMed] [Google Scholar]
- 3.Shokouh-Amiri MH, Hansen CP, Moesgaard F. Liposarcoma of the stomach. A case report. Acta Chir Scand. 1986;152:389–391. [PubMed] [Google Scholar]
- 4.Laky D, Stoica T. Gastric liposarcoma. A case report. Pathol Res Pract. 1986;181:112–117. doi: 10.1016/S0344-0338(86)80202-3. [DOI] [PubMed] [Google Scholar]
- 5.López-Negrete L, Luyando L, Sala J, López C, Menéndez de Llano R, Gomez JL. Liposarcoma of the stomach. Abdom Imaging. 1997;22:373–375. doi: 10.1007/s002619900213. [DOI] [PubMed] [Google Scholar]
- 6.Jelinek JS, Kransdorf MJ, Shmookler BM, Aboulafia AJ, Malawer MM. Liposarcoma of the extremities: MR and CT findings in the histologic subtypes. Radiology. 1993;186:455–459. doi: 10.1148/radiology.186.2.8421750. [DOI] [PubMed] [Google Scholar]
- 7.Laurino L, Furlanetto A, Orvieto E, Dei Tos AP. Well-differentiated liposarcoma (atypical lipomatous tumors) Semin Diagn Pathol. 2001;18:258–262. [PubMed] [Google Scholar]
- 8.Einarsdóttir H, Skoog L, Söderlund V, Bauer HC. Accuracy of cytology for diagnosis of lipomatous tumors: comparison with magnetic resonance and computed tomography findings in 175 cases. Acta Radiol. 2004;45:840–846. doi: 10.1080/02841850410008180. [DOI] [PubMed] [Google Scholar]
- 9.Dei Tos AP. Liposarcoma: new entities and evolving concepts. Ann Diagn Pathol. 2000;4:252–266. doi: 10.1053/adpa.2000.8133. [DOI] [PubMed] [Google Scholar]
- 10.Ferrozzi F, Tognini G, Bova D, Pavone P. Lipomatous tumors of the stomach: CT findings and differential diagnosis. J Comput Assist Tomogr. 2000;24:854–858. doi: 10.1097/00004728-200011000-00006. [DOI] [PubMed] [Google Scholar]