

Abstract
A potential association between Alzheimer’s disease (AD) and chronic glaucoma has been suggested but results of epidemiological studies have been inconsistent. Therefore, we performed a systematic review and critical appraisal of this literature. We searched systematically in PubMed from December 1964 to September 2013 and identified 239 articles potentially relevant for abstract and full-text review. Statistical heterogeneity (variability) across studies was evaluated using the Cochran Q test and the I2 statistic, and the Newcastle-Ottawa score was used to assess study quality. Ten studies were finally selected. Compared to non-demented participants, patients with AD had a statistically significant decreased risk of glaucoma but the results were very heterogeneous, and thus summary estimates were not reported (I2, 89%; Pheterogeneity, <0.001). The study results ranged from large positive relative risks identified in small and poorly-conducted studies to weak inverse associations or null estimates observed in some cohort and record-linkage studies, but the summary estimates were essentially driven by a large retrospective cohort using medical claims that may be afflicted by underdiagnosis bias. There was also evidence for substantial publication bias (Egger’s P≤0.01). The association of AD and glaucoma is heterogeneous and most studies are small and inadequately designed. Large prospective studies with long follow-ups are warranted to clarify this association.
Keywords: systematic review, Alzheimer disease, neurodegenerative diseases, glaucoma
Introduction
Recent evidence has suggested a potential association between Alzheimer’s disease (AD) and chronic glaucoma. Glaucoma is a group of optic neuropathies that are characterized by progressive neurodegeneration of retinal ganglion cells and their axons, resulting in structural changes of the optic nerve and visual field defects.1 Elevated intraocular pressure is a major risk factor of glaucoma,2 and open-angle glaucoma is its most prevalent form worldwide.3 Dementia is also a group of neurodegenerative disorders that occurs in the elderly and leads to impaired cognition. AD is the most common type of dementia4 and is characterized by the presence of extracellular amyloid plaques and intracellular neurofibrillary tangles consisted of hyperphosphorylated tau protein.5
Therefore, it has been suggested that AD and glaucoma are indirectly associated via common pathophysiological mechanisms or risk factors.6–12 Neuro-inflammation may be an important mechanism for the development of both AD and glaucoma.6 The complement component 1q is upregulated in AD, as well as in mouse and monkey glaucoma models.7,8 Elevated tumor necrosis factor-α concentrations contribute to the neurodegeneration process in AD and glaucoma.9,10 In addition, some studies have shown similar levels of both amyloid β1–42 and tau protein in the cerebrospinal fluid of AD patients and in the vitreous fluid of glaucoma patients.11,12
However, it is unclear if the AD and glaucoma association is causal. Some epidemiological studies have reported a higher risk of glaucoma in patients with AD or a higher risk of AD in patients with glaucoma,13–18 whereas other studies reported null or even inverse associations.19–22 The reasons underlying these heterogeneous findings need to be investigated, but no formal evaluation of this literature has been published. Therefore, we performed a systematic review to describe and critically appraise the findings of the AD and chronic glaucoma literature.
Materials and methods
Study identification
We searched systematically in PubMed from December 1964 through September 2013 to identify observational studies that investigated the association between AD or dementia with chronic glaucoma using the following algorithm: “(glaucoma or primary open-angle glaucoma or pseudoexfoliation glaucoma) and (dementia or Alzheimer’s disease or vascular dementia)”. No language restrictions were imposed. We excluded articles that did not have glaucoma or dementia as the outcome, that had no human or original data, and that did not have a control group. We also excluded screening and case-report studies. Our search identified 239 studies potentially relevant for abstract review (Figure 1). There were 100 studies claimed for full-text review based on information in the abstracts. Of these, ten articles were established as pertinent.13–22 Abstract and full-text review was conducted independently by two investigators (AGT and KKT) and discrepancies were resolved by consensus. The methodological quality of the included studies was assessed independently by AGT and KKT using the Newcastle-Ottawa scale, which accords a maximum of nine points to each study, with five or less points indicating a high risk of bias.23 Data on each study, including location, population, design, number of cases and controls, method of assessment of glaucoma and AD, mean age, percentage of males, type of statistical analysis, relative risk (RR) and 95% confidence interval (CI), matching and adjustment factors were independently abstracted into a standardized form. We further systematically searched for relevant articles in EMBASE and the COCHRANE databases, but no further articles were deemed eligible.
Figure 1.

Flow diagram of the study selection process.
Notes: We further systematically searched for relevant articles in EMBASE and the COCHRANE databases, but no further articles were deemed eligible.
Statistical analysis
We abstracted the maximally adjusted RR estimates and 95% CIs for the association of AD or dementia and glaucoma. The eligible studies reported odds ratios, hazard ratios (HRs) or standardized incidence ratios, which were considered equivalent given that AD and glaucoma are relatively rare except in populations over 80 years.24,25 Some studies did not provide RR estimates in the publication, and we calculated matched or unmatched odds ratios from 2×2 tables.13–16,18 Bayer et al published two small case-control studies in 2002 with insufficient information as to whether they used independent samples.14,15 Further information was requested from the authors but no details were supplied, and the samples were assumed independent for this meta-analysis.
The statistical synthesis was performed using the fixed effects method with each RR estimate weighted by the inverse of its variance. We did not conduct a random effects synthesis, because it tends to be overtly inflated in the presence of small study effects, as the small studies receive increased relative weight in random effects calculations.26 We performed a meta-analysis for the association between AD and glaucoma (eight studies) and separately for dementia and glaucoma (nine studies), but the results were very heterogeneous and were therefore not reported in detail in the text or in tables and figures.
Subgroup analyses were also performed to investigate potential sources of heterogeneity. We repeated the fixed effects synthesis after omitting one study at a time. The association of dementia and glaucoma was assessed by study location (Europe, USA, Asia), design (cohort, record linkage, case-control), number of cases (≥100, <100), use of matching or adjustment (for at least one factor, crude) and mean age of the study population at recruitment (≥75, <75 years). To test whether the summary estimates differed between strata of the latter characteristics, we conducted meta-regression analyses.
Statistical heterogeneity (variability) across studies was evaluated using the Cochran Q test and the I2 statistic27,28 with its corresponding 95% CIs.29 An I2 value of 0% implies lack of heterogeneity, whereas values of 25%, 50% and 75% imply low, medium, and high heterogeneity respectively. Publication bias (bias against the publication of negative results or publication of those results after considerable delay) was quantified from the visual inspection of a funnel plot,30 from the Begg rank correlation method31 and the Egger’s regression asymmetry test (publication bias considered present if P≤0.10).30 A nonparametric “trim and fill” method that accounts for publication bias was also applied.32 All statistical analyses were performed with STATA software version 12 (StataCorp LP, College station, TX, USA), and all tests were two-sided.
Results
Ten studies were selected according to our inclusion criteria (Figure 1, Tables 1 and 2). Six studies were conducted in Europe,14,15,17,19,20,22 two in the United States13,21 and two in Asia.16,18 Five reports were case-control studies,13–16,18 of which two used prevalent cases,14,15 two were record-linkage studies20,22 and another three were cohort studies,17,19,21 of which one was a retrospective cohort.21 All studies used patients with open angle glaucoma, a form of glaucoma that has been hypothesized to have neurodegenerative elements. The number of cases with glaucoma in these studies ranged between 21 and 63,325. Participants had a mean age at recruitment that ranged from 64 to 83 years. Most case-control studies had less than 350 total participants14–16,18 except for one study using death certificates that had more than 20,000 participants but very few exposed cases,13 and all observed large positive and strongly significant RRs for the association between AD or dementia and glaucoma. In contrast, the large retrospective cohort study with 63,325 cases of glaucoma observed a statistically significant inverse association,21 whereas other prospective cohort and record-linkage studies reported mixed results.17,19,20,22 One study was further excluded from the meta-analysis, because it did not identify any case with AD, and thus calculated a zero RR.22
Table 1.
Study characteristics of the ten eligible studies on dementia and glaucoma risk
| Study | Location/population | Design | Cases/controls | Exposure/outcome | Assessment of glaucoma | Assessment of AD/dementia |
|---|---|---|---|---|---|---|
| Chandra et al, 198613 | USA/general population | Case-control | 7,195/14,390 | OAG/AD | Death certificate | Death certificate |
| Bayer et al, 200214,# | Germany/nursing homes | Prevalent case-control | 49/186 | OAG/AD | Glaucomatous VFD, CDR ≥0.8 | NR |
| Bayer et al, 200215,# | Germany/nursing homes | Prevalent case-control | 112/116 | OAG/AD | Glaucomatous VFD, CDR ≥0.8 | NINCDS-ADRDA |
| Tamura et al, 200616 | Japan/hospitals | Case-control | 172/176 | OAG/AD | ACAW, VCDR >0.7, VCDRD >0.2 | NINCDS-ADRDA |
| Kessing et al, 200720 | Denmark/general population | Record-linkage | 11,721* | AD/OAG | ICD-8, ICD-10 | ICD-8, ICD-10 |
| Bach-Holm et al, 201122 | Denmark/hospital | Record-linkage | 69* | OAG/AD | Glaucomatous VFD, IOP ≤24 mmHg | ICD-8, ICD-10 |
| Ou et al, 201221 | USA/medicare beneficiaries | Retrospective cohort‡ | 63,325/63,325 | OAG/AD | ICD-9 | ICD-9 |
| Cumurcu et al, 201318 | Turkey/hospital | Case-control | 21/67 | AD/OAG | IOP ≥21mmHg, glaucomatous ODD/VFD | DSM-IV (2000) |
| Helmer et al, 201317 | France/study volunteers | CohortIII | 41/771 | AD/OAG | VCDR ≥0.65, MRDR ≤0.1, VCDRD >0.2 | DSM-IV (1994) |
| Ekstrom and Kilander, 201319 | Sweden/study volunteers | Cohort¶ | 174/949 | AD/OAG | IOP, VFD | NINCDS-ADRDA |
Notes:
Patients with glaucoma compared to glaucoma prevalence or incidence rates from the general population of each country
it is not clear if these studies used independent samples
14 years of follow-up
3 years of follow-up
over 25 years of follow-up.
Abbreviations: ACAW, anterior chamber’s angle width; AD, Alzheimer’s disease; CDR, cup-to-disc ratio; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders, fourth edition; ICD, International Statistical Classification of Diseases and related health problems; IOP, intraocular pressure; MRDR, minimal rim to disc ratio; NINCDS-ADRDA, National Institute of Neurological and Communicative Disorders and Stroke – Alzheimer’s Disease and Related Disorders Association; NR, not reported; OAG, open-angle glaucoma; ODD, optic disc damage; VCDR, vertical cup-to-disc ratio; VCDRD, vertical cup-to-disc ratio difference; VFD, visual field defect.
Table 2.
Population characteristics of the ten eligible studies on dementia and glaucoma risk
| Study | Matching criteria | Mean age, years (cases/controls) |
% males (cases/controls) |
Statistical analysis | RR (95% CI) (AD and OAG) |
RR (95% CI) (non-AD dementia and OAG) |
RR (95% CI) (dementia and OAG) |
Adjustment factors |
|---|---|---|---|---|---|---|---|---|
| Chandra et al, 198613 | Age, sex, race, year, and county of death† | 80.1/79.8 | 40.6/NR | Matched OR* | 2.60 (1.06–6.43) | NR | NR | None |
| Bayer et al, 200214 | Age, sex, fam hx of glaucoma, myopia, systemic disease‡ | 72.9/68.4 | 38.8/43.5 | Crude OR* | 4.70 (1.95–11.4) | NR | NR | None |
| Bayer et al, 200215 | Age, sex, fam hx of glaucoma, myopia, systemic disease‡ | 71.8/68.2 | 33.9/34.5 | Crude OR* | 6.41 (2.56–16.1) | NR | NR | None |
| Tamura et al, 200616 | Age, sex‡ | 80.9/81.9 | 20.3/23.9 | Crude OR* | 3.13 (1.67–5.85) | NR | NR | None |
| Kessing et al, 200720 | None | 70.9 | 46.6 | SIR | 0.76 (0.56–1.05) | 0.95 (0.85–1.07) | 1.08 (0.97–1.20) | Age, sex |
| Bach-Holm et al, 201122 | None | 64.0 | 27.5 | SIR | 0 (0–4.06) | 0.20 (0.01–1.11) | NR | Age, sex |
| Ou et al, 201221 | Age, sex, race, CCIII | 78.5/78.5 | 36.0/34.0 | HR | 0.91 (0.88–0.93) | NR | 0.93 (0.91–0.95) | Age, sex, race, CCI, ophthalmic diseases¶ |
| Cumurcu et al, 201318 | Age, sex, education‡ | NR/70.9 | NR/71.6 | Crude OR* | 5.44 (1.88–15.6) | NR | NR | None |
| Helmer et al, 201317 | None | 83.2/79.5 | 21.9/36.1 | OR | NR | NR | 3.90 (1.50–10.4) | Age, sex, education, fam hx of glaucoma, vascular diseases, Apoe4 |
| Ekstrom and Kilander, 201319 | None | NR | NR | HR | 1.09 (0.69–1.74) | NR | NR | Age, sex |
Notes:
The point estimates and 95% confidence intervals of the relative risks were not reported in these publications, and were thus calculated from 2×2 tables. Crude odds ratios were calculated in four studies because frequency matching was performed.
Individual matching was used
frequency matching was most likely used
propensity score matching was used
macular degeneration, diabetic retinopathy, vitreous hemorrhage, cataract, pseudophakia/aphakia.
Abbreviations: AD, Alzheimer’s disease; Apoe4, apolipoprotein e4; CCI, Charlson comorbidity index; CI, confidence internal; fam hx, family history; HR, hazard ratio; NR, not reported; OAG, open-angle glaucoma; OR, odds ratio; RR, relative risk; SIR, standardized incidence ratio.
The median Newcastle-Ottawa quality score was 4 with an interquartile range (IQR) from 4 to 7 (Tables S1 and S2). The five case-control studies13–16,18 scored poorly in the quality scale (median, 4; IQR, 2–4) because most studies did not independently validate the case definition; they did not use population-based controls, and did not control for important potential confounders. The four cohort and record-linkage studies17,19–21 had a median quality score of 7 (IQR, 5.5–7), and all but one20 had scores of 7.
Compared to non-demented participants, patients with AD (eight studies; RR, 0.92; 95% CI, 0.89–0.94; I2, 89%; Pheterogeneity, <0.001) or with dementia (nine studies; RR, 0.94; 95% CI, 0.92–0.96; I2, 89.4%; Pheterogeneity, <0.001) had a statistically significant decreased risk of glaucoma, respectively (Figures 2 and 3). The study results were very heterogeneous and tended to follow the finding of the largest study in our sample.21 After excluding the Ou et al21 study, the findings changed to a statistically significant positive association, but they were still very heterogeneous.
Figure 2.
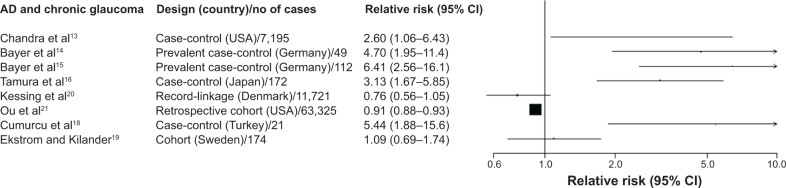
Study-specific relative risks and 95% confidence intervals (CI) for the association of Alzheimer’s disease (AD) and chronic glaucoma.
Notes: We decided not to report the statistical synthesis of the results from the eight eligible studies because of the substantial heterogeneity (I2, 89%; Pheterogeneity, <0.001).
Figure 3.
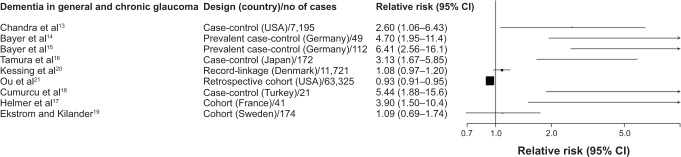
Study-specific relative risks and 95% confidence intervals (CI) for the association of dementia in general and chronic glaucoma.
Notes: We decided not to report the statistical synthesis of the results from the nine eligible studies because of the substantial heterogeneity (I2, 89%; Pheterogeneity, <0.001).
Funnel plots and statistical tests (AD and glaucoma: Egger’s Pheterogeneity, 0.01; Dementia and glaucoma: Egger’s Pheterogeneity, <0.001) provided evidence for substantial publication bias, as there were several very small studies with large and positive RRs.14–18 When we attempted to correct for publication bias using the non-parametric trim and fill method, the results of the meta-analysis remained identical, as adding several small studies with strong inverse associations to the funnel plot did not leverage the results of the large Ou et al study. In meta-analyses performed by study location, design, number of cases, use of adjustments for confounders and mean age, dementia was associated with a lower risk of glaucoma in the subgroups where the Ou et al study belonged (studies in USA, cohorts, number of cases ≥100, adjusted results, and mean age ≥75 years), whereas the summary results were significantly positive in all other subgroups (Table S3).
Discussion
In this systematic review, we critically appraised ten studies for the association between AD or dementia and chronic glaucoma. The findings of the ten studies were extremely heterogeneous and ranged from large positive RRs identified in small and poorly-conducted case-control studies to weak inverse associations or null estimates observed in some cohort and record-linkage studies. The summary estimate was identical to the result of the large Ou et al retrospective cohort study, which reported an inverse association between AD and glaucoma but this study used medical claims to infer about diagnosis of dementia and glaucoma and it may be afflicted by underdiagnosis bias.
It is unclear pathophysiologically why there should be an inverse association between AD and glaucoma. Although the literature has not provided potential mechanistic clues for an inverse association, many researchers have suggested mechanisms explaining a positive association between the two diseases. It has been shown that patients with AD exhibit a cerebrospinal fluid stasis due to decreased secretion and increased resistance to cerebrospinal fluid outflow,33–36 resulting in reduced clearance of the toxic molecules in the subarachnoid space of the optic nerve and a low cerebrospinal fluid pressure, which may lead to an abnormal high trans-lamina cribrosa pressure difference and to a larger cup-to-disc ratio followed by glaucomatous damage.37–40 However, other studies have suggested that even though an abnormal high trans-lamina cribrosa pressure difference is created, there is no observable alteration in the lamina cribrosa resulting in no optic disc cupping,41 which does not support an association between AD and glaucoma. Several factors should be considered for the interpretation of our findings. AD and chronic glaucoma are both age-related neurodegenerative diseases that may very well co-exist in the elderly due to common risk factors or pathophysiological mechanisms. However, to infer a direct and causal association between them, prospective designs are warranted where chronic glaucoma is evaluated many years after the diagnosis of AD (or vice versa) in participants who are free of glaucoma (or any early signs of it) at the start of the study. Sensitivity analyses where the first 2–5 years of follow-up are discarded may assist in identifying a potential causal effect.
However, half of the studies that were included in this systematic review had a case-control design that precludes a valid assessment of the association between AD and glaucoma, as both diseases were evaluated cross-sectionally at recruitment.13–16,18 The study sample also included one record-linkage20 and three cohort studies.17,19,21 The retrospective cohort by Ou et al used Medicare data to identify 63,325 participants with glaucoma and 63,325 participants without glaucoma who had no AD or other dementia at recruitment, and were followed up for 14 years.21 This was by far the largest study in our sample, and found a statistically significant inverse association between glaucoma and AD (HR, 0.91; 95% CI, 0.88–0.93). The use of administrative data in this study may lead to misclassification of the diagnoses of glaucoma and/or dementia and to potential underdiagnosis bias. Patients with cognitive decline are perhaps less likely to undergo formal ophthalmologic testing and this could cause the non-glaucoma group to contain a larger proportion of individuals who are subsequently diagnosed with dementia. The French cohort by Helmer et al studied 812 volunteers and identified 41 cases of dementia in 3 years of total follow-up.17 They observed a strong statistically significant positive association between dementia and glaucoma (HR, 3.90; 95% CI, 1.50–10.4). Although this study was prospective and excluded demented participants at recruitment, its short follow-up led to a small number of incident dementia cases who most likely had brain pathology at least at a mild level at baseline. The third cohort study was conducted in Sweden among 1,123 city residents; it identified 174 new cases of AD in a maximum follow-up of 25 years and reported a non-significant HR of 1.09 (95% CI, 0.69–1.74) between AD and chronic glaucoma.19
High heterogeneity was ubiquitous in all of our analyses. Heterogeneity may be introduced because of the methodologic or demographic differences among studies. However, we were unable to identify the exact sources of heterogeneity in our systematic review, because the summary results were always driven by the large Ou et al study, even though we performed subgroup and meta-regression analyses on several factors. However, even when we reran the meta-analysis after excluding the Ou et al study, the results remained heterogeneous. Therefore, we decided not to report in detail the summary RRs.
Meta-analyses of observational studies are also vulnerable to residual confounding inherent in the original studies. The Ou et al and Helmer et al studies both adjusted for a range of confounders that included age, sex, race, education, family history of glaucoma, and comorbidities.17,21 The case-control studies adjusted only for age and/or sex, whereas some studies did report frequency matching for a wider set of confounders;14–16,18 however, RRs were not reported in these studies and had to be calculated crudely from 2×2 tables, which may explain at least partially why the authors observed strong positive associations, as some comorbidities and the black race are positively associated with both AD and glaucoma and could cause the overestimation of the unadjusted results.
Conclusion
In summary, the association of AD and chronic glaucoma is heterogeneous in the literature and most studies are small and inadequately designed. Large and high-quality prospective studies with long follow-ups are needed to clarify the existence, magnitude, and natural history of this potential association.
Supplementary materials
Table S1.
Newcastle-Ottawa scale for the quality assessment of five case-control studies on dementia and glaucoma risk
| Quality assessment criteria | Acceptable | Chandra et al13 | Bayer et al14 | Bayer et al15 | Tamura et al16 | Cumurcu et al18 |
|---|---|---|---|---|---|---|
| Selection | ||||||
| Is the case definition adequate? | Yes, with independent validation | – | – | – | – | – |
| Representativeness of cases? | Consecutive or obviously representative cases | √ | √ | √ | – | – |
| Selection of controls? | Community controls | √ | – | – | – | – |
| Definition of controls? | No history of AD/glaucoma* | – | √ | √ | √ | – |
| Comparability | ||||||
| Study controls for age and sex? | Yes# | √ | – | – | – | – |
| Study controls for additional factors? | Race, comorbidities‡ | – | – | – | – | – |
| Exposure | ||||||
| Ascertainment of exposure? | Secure record or structured interview blinded to case/control status | – | √ | √ | – | – |
| Same method of ascertainment of cases/controls? | Yes | √ | √ | √ | √ | √ |
| Non-response rate? | Same for both groups | √ | – | – | – | – |
Notes:
Depending on whether AD or glaucoma was the outcome in each case-control study
some case-control studies15–17,19 did report frequency matching for age and sex, but these studies did not report relative risks in the text and they had to be calculated crudely from 2×2 tables
some case-control studies15,16 did report frequency matching for comorbidities, but these studies did not report relative risks in the text and they had to be calculated crudely from 2×2 tables.
Abbreviation: AD, Alzheimer’s disease.
Table S2.
Newcastle-Ottawa scale for the quality assessment of four cohort and record-linkage studies on dementia and glaucoma risk
| Quality assessment criteria | Acceptable | Kessing et al*,20 | Ou et al#,21 | Helmer et al#,17 | Ekstrom and Kilander#,19 |
|---|---|---|---|---|---|
| Selection | |||||
| Representativeness of exposed cohort? | Representative of average adult in community | √ | √ | – | – |
| Selection of non-exposed cohort? | Drawn from same community as exposed cohort | √ | √ | √ | √ |
| Ascertainment of exposure? | Secure records or structured interview | – | – | √ | √ |
| Demonstration that outcome of interest was not present at start of study? | – | √ | √ | √ | |
| Comparability | |||||
| Study controls for age and sex? | Yes | √ | √ | √ | √ |
| Study controls for additional risk factors? | Race, comorbidities | – | √ | √ | – |
| Outcome | |||||
| Assessment of outcome? | Independent blind assessment or record linkage | – | – | √ | √ |
| Was follow-up long enough for outcome to occur? | Follow-up >5 years | √ | √ | – | √ |
| Adequacy of follow-up of cohorts? | Complete follow-up or subjects lost to follow-up unlikely to introduce bias | – | √ | √ | √ |
Notes:
Record-linkage study
cohort study.
Table S3.
Summary fixed-effects relative risks (RR) and 95% confidence intervals (CI) for the association of dementia in general and glaucoma in subgroups
| Outcome measures | No of studies | Summary RR (95% CI) | Pheterogeneity* |
|---|---|---|---|
| Study location | |||
| Europe | 514,15,17,19,20 | 1.14 (1.03–1.27) | <0.01 |
| USA | 213,21 | 0.93 (0.91–0.95) | 0.03 |
| Asia | 216,18 | 3.61 (2.11–6.20) | 0.38 |
| Study design | |||
| Cohort | 317,19,21 | 0.93 (0.91–0.95) | 0.01 |
| Record-linkage | 120 | 1.08 (0.97–1.20) | <0.01 |
| Case-control | 513–16,18 | 3.94 (2.71–5.72) | 0.57 |
| Number of cases | |||
| <100 | 314,17,18 | 4.60 (2.64–8.02) | 0.90 |
| ≥100 | 613,15,16,19–21 | 0.94 (0.92–0.96) | <0.01 |
| Matching or adjustment | |||
| For at least one factor | 513,17,19–21 | 0.94 (0.92–0.96) | <0.01 |
| Crude | 414–16,18 | 4.29 (2.84–6.48) | 0.59 |
| Mean age | |||
| <75 years | 514,15,18–20 | 1.14 (1.03–1.27) | <0.01 |
| ≥75 years | 413,16,17,21 | 0.93 (0.91–0.95) | <0.01 |
Note:
Evaluated in each subgroup using the Cochran Q test.
Author contributions
All authors (AGT, KKT, S-HP, GK) contributed to the conception and design of the study. AGT and KKT acquired the data for the systematic review, performed the statistical analysis, and wrote the paper. S-HP and GK contributed critically to the revisions of the paper and had valuable input to the clinical interpretation of the discussion. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
None of the authors had financial support related to this study. The authors declare that there is no conflict of interests regarding the publication of this paper. This submission has not been published elsewhere previously and it is not currently under consideration by another journal.
References
- 1.Boland MV, Ervin AM, Friedman D, et al. Treatment for Glaucoma: Comparative Effectiveness. Rockville (MD): Agency for Healthcare Research and Quality (US); 2012. [PubMed] [Google Scholar]
- 2.Nickells RW, Howell GR, Soto I, John SW. Under pressure: cellular and molecular responses during glaucoma, a common neurodegeneration with axonopathy. Annu Rev Neurosci. 2012;35:153–179. doi: 10.1146/annurev.neuro.051508.135728. [DOI] [PubMed] [Google Scholar]
- 3.Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262–267. doi: 10.1136/bjo.2005.081224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Reitz C, Brayne C, Mayeux R. Epidemiology of Alzheimer disease. Nat Rev Neurol. 2011;7(3):137–152. doi: 10.1038/nrneurol.2011.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bossy-Wetzel E, Schwarzenbacher R, Lipton SA. Molecular pathways to neurodegeneration. Nat Med. 2004;10(Suppl):S2–S9. doi: 10.1038/nm1067. [DOI] [PubMed] [Google Scholar]
- 6.McKinnon SJ. The cell and molecular biology of glaucoma: common neurodegenerative pathways and relevance to glaucoma. Invest Ophthalmol Vis Sci. 2012;53(5):2485–2487. doi: 10.1167/iovs.12-9483j. [DOI] [PubMed] [Google Scholar]
- 7.Fonseca MI, Chu SH, Berci AM, et al. Contribution of complement activation pathways to neuropathology differs among mouse models of Alzheimer’s disease. J Neuroinflammation. 2011;8(1):4. doi: 10.1186/1742-2094-8-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stasi K, Nagel D, Yang X, et al. Complement component 1Q (C1Q) upregulation in retina of murine, primate, and human glaucomatous eyes. Invest Ophthalmol Vis Sci. 2006;47(3):1024–1029. doi: 10.1167/iovs.05-0830. [DOI] [PubMed] [Google Scholar]
- 9.Tezel G. TNF-alpha signaling in glaucomatous neurodegeneration. Prog Brain Res. 2008;173:409–421. doi: 10.1016/S0079-6123(08)01128-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tobinick E. Tumour necrosis factor modulation for treatment of Alzheimer’s disease: rationale and current evidence. CNS Drugs. 2009;23(9):713–725. doi: 10.2165/11310810-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 11.Engelborghs S, De Vreese K, Van de Casteele T, et al. Diagnostic performance of a CSF-biomarker panel in autopsy-confirmed dementia. Neurobiol Aging. 2008;29(8):1143–1159. doi: 10.1016/j.neurobiolaging.2007.02.016. [DOI] [PubMed] [Google Scholar]
- 12.Yoneda S, Hara H, Hirata A, Fukushima M, Inomata Y, Tanihara H. Vitreous fluid levels of beta-amyloid(1–42) and tau in patients with retinal diseases. Jpn J Ophthalmol. 2005;49(2):106–108. doi: 10.1007/s10384-004-0156-x. [DOI] [PubMed] [Google Scholar]
- 13.Chandra V, Bharucha NE, Schoenberg BS. Conditions associated with Alzheimer’s disease at death: case-control study. Neurology. 1986;36(2):209–211. doi: 10.1212/wnl.36.2.209. [DOI] [PubMed] [Google Scholar]
- 14.Bayer AU, Keller ON, Ferrari F, Maag KP. Association of glaucoma with neurodegenerative diseases with apoptotic cell death: Alzheimer’s disease and Parkinson’s disease. Am J Ophthalmol. 2002;133(1):135–137. doi: 10.1016/s0002-9394(01)01196-5. [DOI] [PubMed] [Google Scholar]
- 15.Bayer AU, Ferrari F, Erb C. High occurrence rate of glaucoma among patients with Alzheimer’s disease. Eur Neurol. 2002;47(3):165–168. doi: 10.1159/000047976. [DOI] [PubMed] [Google Scholar]
- 16.Tamura H, Kawakami H, Kanamoto T, et al. High frequency of open-angle glaucoma in Japanese patients with Alzheimer’s disease. J Neurol Sci. 2006;246(1–2):79–83. doi: 10.1016/j.jns.2006.02.009. [DOI] [PubMed] [Google Scholar]
- 17.Helmer C, Malet F, Rougier MB, et al. Is there a link between open-angle glaucoma and dementia? The Three-City-Alienor Cohort. Ann Neurol. 2013;74(2):171–179. doi: 10.1002/ana.23926. [DOI] [PubMed] [Google Scholar]
- 18.Cumurcu T, Dorak F, Cumurcu BE, Erbay LG, Ozsoy E. Is there any relation between pseudoexfoliation syndrome and Alzheimer’s type dementia? Semin Ophthalmol. 2013;28(4):224–229. doi: 10.3109/08820538.2013.793726. [DOI] [PubMed] [Google Scholar]
- 19.Ekstrom C, Kilander L. Pseudoexfoliation and Alzheimer’s disease: a population-based 30-year follow-up study. Acta Ophthalmol. 2014;92(4):355–358. doi: 10.1111/aos.12184. [DOI] [PubMed] [Google Scholar]
- 20.Kessing LV, Lopez AG, Andersen PK, Kessing SV. No increased risk of developing Alzheimer disease in patients with glaucoma. J Glaucoma. 2007;16(1):47–51. doi: 10.1097/IJG.0b013e31802b3527. [DOI] [PubMed] [Google Scholar]
- 21.Ou Y, Grossman DS, Lee PP, Sloan FA. Glaucoma, Alzheimer disease and other dementia: a longitudinal analysis. Ophthalmic Epidemiol. 2012;19(5):285–292. doi: 10.3109/09286586.2011.649228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Bach-Holm D, Kessing SV, Mogensen U, Forman JL, Andersen PK, Kessing LV. Normal tension glaucoma and Alzheimer disease: comorbidity? Acta Ophthalmol. 2012;90(7):683–685. doi: 10.1111/j.1755-3768.2011.02125.x. [DOI] [PubMed] [Google Scholar]
- 23.Ottawa Hospital Research Institute [homepage on the Internet] Wells GA, Shea B, O’ Connell D, Peterson J, Welch V, Losos M, Tugwell P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. [Accessed October 2, 2013]. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.
- 24.Ferri CP, Prince M, Brayne C, et al. Global prevalence of dementia: a Delphi consensus study. Lancet. 2005;366(9503):2112–2117. doi: 10.1016/S0140-6736(05)67889-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Friedman DS, Wolfs RC, O’ Colmain BJ, et al. Prevalence of open-angle glaucoma among adults in the United States. Arch Ophthalmol. 2004;122(4):532–538. doi: 10.1001/archopht.122.4.532. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Higgins J, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions. England: Chichester: The Cochrane Collaboration and John Wiley & Sons Ltd; 2008. [Google Scholar]
- 27.Cochran WG. The combination of estimates from different experiments. Biometrics. 1954;10(1):101–129. [Google Scholar]
- 28.Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med. 2002;21(11):1539–1558. doi: 10.1002/sim.1186. [DOI] [PubMed] [Google Scholar]
- 29.Ioannidis JP, Patsopoulos NA, Evangelou E. Uncertainty in heterogeneity estimates in meta-analyses. BMJ. 2007;335(7626):914–916. doi: 10.1136/bmj.39343.408449.80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088–1101. [PubMed] [Google Scholar]
- 32.Duval S, Tweedie R. A nonparametric “trim and fill” method of accounting for publication bias in meta-analysis. Journal of the American Statistical Association. 2000;95:89–98. [Google Scholar]
- 33.Serot JM, Bene MC, Faure GC. Choroid plexus, aging of the brain, and Alzheimer’s disease. Front Biosci. 2003;8:s515–s521. doi: 10.2741/1085. [DOI] [PubMed] [Google Scholar]
- 34.Silverberg GD, Heit G, Huhn S, et al. The cerebrospinal fluid production rate is reduced in dementia of the Alzheimer’s type. Neurology. 2001;57(10):1763–1766. doi: 10.1212/wnl.57.10.1763. [DOI] [PubMed] [Google Scholar]
- 35.Serot JM, Zmudka J, Jouanny P. A possible role for CSF turnover and choroid plexus in the pathogenesis of late onset Alzheimer’s disease. J Alzheimers Dis. 2012;30(1):17–26. doi: 10.3233/JAD-2012-111964. [DOI] [PubMed] [Google Scholar]
- 36.Silverberg GD, Mayo M, Saul T, Rubenstein E, McGuire D. Alzheimer’s disease, normal-pressure hydrocephalus, and senescent changes in CSF circulatory physiology: a hypothesis. Lancet Neurol. 2003;2(8):506–511. doi: 10.1016/s1474-4422(03)00487-3. [DOI] [PubMed] [Google Scholar]
- 37.Wostyn P, Audenaert K, De Deyn PP. An abnormal high trans-lamina cribrosa pressure difference: a missing link between Alzheimer’s disease and glaucoma? Clin Neurol Neurosurg. 2008;110(7):753–754. doi: 10.1016/j.clineuro.2008.05.019. [DOI] [PubMed] [Google Scholar]
- 38.Wostyn P, Audenaert K, De Deyn PP. Alzheimer’s disease and glaucoma: is there a causal relationship? Br J Ophthalmol. 2009;93(12):1557–1559. doi: 10.1136/bjo.2008.148064. [DOI] [PubMed] [Google Scholar]
- 39.Wostyn P, Audenaert K, De Deyn PP. More advanced Alzheimer’s disease may be associated with a decrease in cerebrospinal fluid pressure. Cerebrospinal Fluid Res. 2009;6:14. doi: 10.1186/1743-8454-6-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Wostyn P, De Groot V, Van Dam D, Audenaert K, De Deyn PP. Senescent changes in cerebrospinal fluid circulatory physiology and their role in the pathogenesis of normal-tension glaucoma. Am J Ophthalmol. 2013;156(1):5–14. doi: 10.1016/j.ajo.2013.03.003. [DOI] [PubMed] [Google Scholar]
- 41.Hayreh SS. Cerebrospinal fluid pressure and glaucomatous optic disc cupping. Graefes Arch Clin Exp Ophthalmol. 2009;247(6):721–724. doi: 10.1007/s00417-008-0984-3. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1.
Newcastle-Ottawa scale for the quality assessment of five case-control studies on dementia and glaucoma risk
| Quality assessment criteria | Acceptable | Chandra et al13 | Bayer et al14 | Bayer et al15 | Tamura et al16 | Cumurcu et al18 |
|---|---|---|---|---|---|---|
| Selection | ||||||
| Is the case definition adequate? | Yes, with independent validation | – | – | – | – | – |
| Representativeness of cases? | Consecutive or obviously representative cases | √ | √ | √ | – | – |
| Selection of controls? | Community controls | √ | – | – | – | – |
| Definition of controls? | No history of AD/glaucoma* | – | √ | √ | √ | – |
| Comparability | ||||||
| Study controls for age and sex? | Yes# | √ | – | – | – | – |
| Study controls for additional factors? | Race, comorbidities‡ | – | – | – | – | – |
| Exposure | ||||||
| Ascertainment of exposure? | Secure record or structured interview blinded to case/control status | – | √ | √ | – | – |
| Same method of ascertainment of cases/controls? | Yes | √ | √ | √ | √ | √ |
| Non-response rate? | Same for both groups | √ | – | – | – | – |
Notes:
Depending on whether AD or glaucoma was the outcome in each case-control study
some case-control studies15–17,19 did report frequency matching for age and sex, but these studies did not report relative risks in the text and they had to be calculated crudely from 2×2 tables
some case-control studies15,16 did report frequency matching for comorbidities, but these studies did not report relative risks in the text and they had to be calculated crudely from 2×2 tables.
Abbreviation: AD, Alzheimer’s disease.
Table S2.
Newcastle-Ottawa scale for the quality assessment of four cohort and record-linkage studies on dementia and glaucoma risk
| Quality assessment criteria | Acceptable | Kessing et al*,20 | Ou et al#,21 | Helmer et al#,17 | Ekstrom and Kilander#,19 |
|---|---|---|---|---|---|
| Selection | |||||
| Representativeness of exposed cohort? | Representative of average adult in community | √ | √ | – | – |
| Selection of non-exposed cohort? | Drawn from same community as exposed cohort | √ | √ | √ | √ |
| Ascertainment of exposure? | Secure records or structured interview | – | – | √ | √ |
| Demonstration that outcome of interest was not present at start of study? | – | √ | √ | √ | |
| Comparability | |||||
| Study controls for age and sex? | Yes | √ | √ | √ | √ |
| Study controls for additional risk factors? | Race, comorbidities | – | √ | √ | – |
| Outcome | |||||
| Assessment of outcome? | Independent blind assessment or record linkage | – | – | √ | √ |
| Was follow-up long enough for outcome to occur? | Follow-up >5 years | √ | √ | – | √ |
| Adequacy of follow-up of cohorts? | Complete follow-up or subjects lost to follow-up unlikely to introduce bias | – | √ | √ | √ |
Notes:
Record-linkage study
cohort study.
Table S3.
Summary fixed-effects relative risks (RR) and 95% confidence intervals (CI) for the association of dementia in general and glaucoma in subgroups
| Outcome measures | No of studies | Summary RR (95% CI) | Pheterogeneity* |
|---|---|---|---|
| Study location | |||
| Europe | 514,15,17,19,20 | 1.14 (1.03–1.27) | <0.01 |
| USA | 213,21 | 0.93 (0.91–0.95) | 0.03 |
| Asia | 216,18 | 3.61 (2.11–6.20) | 0.38 |
| Study design | |||
| Cohort | 317,19,21 | 0.93 (0.91–0.95) | 0.01 |
| Record-linkage | 120 | 1.08 (0.97–1.20) | <0.01 |
| Case-control | 513–16,18 | 3.94 (2.71–5.72) | 0.57 |
| Number of cases | |||
| <100 | 314,17,18 | 4.60 (2.64–8.02) | 0.90 |
| ≥100 | 613,15,16,19–21 | 0.94 (0.92–0.96) | <0.01 |
| Matching or adjustment | |||
| For at least one factor | 513,17,19–21 | 0.94 (0.92–0.96) | <0.01 |
| Crude | 414–16,18 | 4.29 (2.84–6.48) | 0.59 |
| Mean age | |||
| <75 years | 514,15,18–20 | 1.14 (1.03–1.27) | <0.01 |
| ≥75 years | 413,16,17,21 | 0.93 (0.91–0.95) | <0.01 |
Note:
Evaluated in each subgroup using the Cochran Q test.