

Audience
Interventionalists, and those interested in atherosclerosis and intravascular MR imaging.
Purpose
Current speeds for intravascular (IV) MRI and MRI endoscopy1 are limited to ∼2frames/s at 3T, rendering high-resolution (∼100μm) images susceptible to degradation by physiological motion on the order of mm/ms. Here, using projection reconstruction we: (A) reduce sensitivity to motion from the time-scale of individual images, to the time-frame of each projection (TR) by frame-shifting each projection to the antenna, prior to reconstruction. In addition: (B) we apply compressed sensing to provide acceleration factors of up to four-fold. We present data acquired in phantoms (fruit), human vessel specimens and/or apply the methods to retro-actively acquired data as we move toward prospective acquisitions in vivo.
Methods
IV MRI with and without mechanical motion, is performed on a Philips 3T scanner using a 2mm diameter 3T loopless antenna receiver, and radial k-space traversal. For motion correction (A), we note that in each projection, there is intense signal surrounding the probe, but the probe itself produces no signal. Further, there is a phase reversal that occurs at the probe (Fig. 1 a, d). These amplitude and phase singularities at the probe's location are detected using a signal derivative algorithm, and used to align all the projections (Fig. 1f). Images reconstructed from these, always have the probe at the center of the field-of-view. Compressed sensing (B), is performed on projection images using uniform under-sampling2, while variable-density random under-sampling is used on previously-acquired in vivo Cartesian data1. Images are reconstructed using “ℓ1-norm” minimization and wavelet transform2,3.
Figure 1.
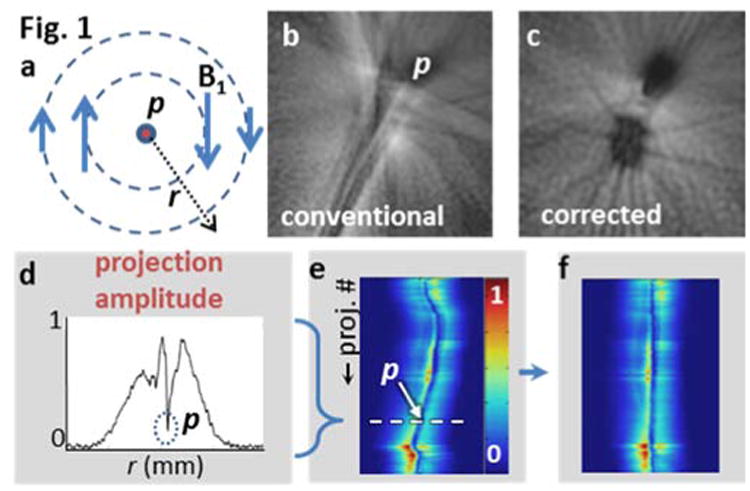
(a) Transverse field of a loopless antenna detector p shows decreasing B1 with r and azimuthal variation in phase. (b) MRI of an orange shaken ± 3mm (2D radial GRE; 200 spokes spanning 180°; 250μm in-plane resolution; TR/TE=15/6 ms) shows debilitating motion artifacts. (c) Projection shifting all but removes streaking, revealing the fruit's underlying structure. A 1/r intensity filter has been applied to aid visualization. (d-f) The motion correction algorithm consists of re-aligning every azimuthal projection on p.
Results
Motion correction significantly reduces motion artefact compared to conventional reconstruction (Fig. 1b vs. 1c). Radial and Cartesian compressed sensing produced virtually indistinguishable images with only 1/4th to 1/3rd of the original data (Fig. 2, 3). Since the motion correction algorithm acts on each projection, it was also applied to a radially under-sampled data set (not shown).
Figure 2.
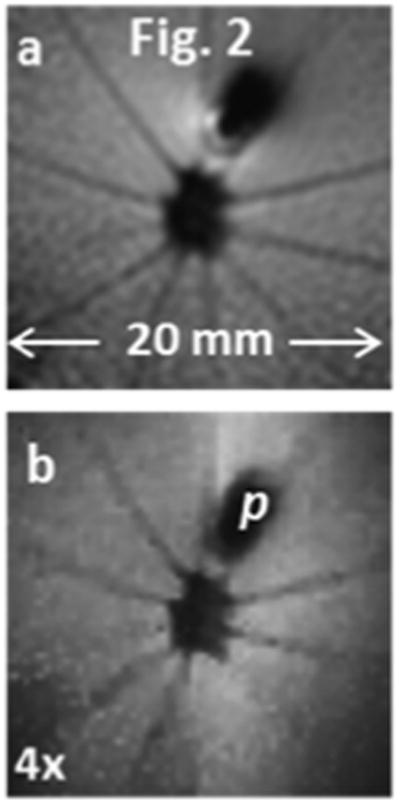
Fruit morphology using the complete data set (a), is retained in a four-fold under-sampled radial-compressed sense reconstruction (b).
Figure 3.
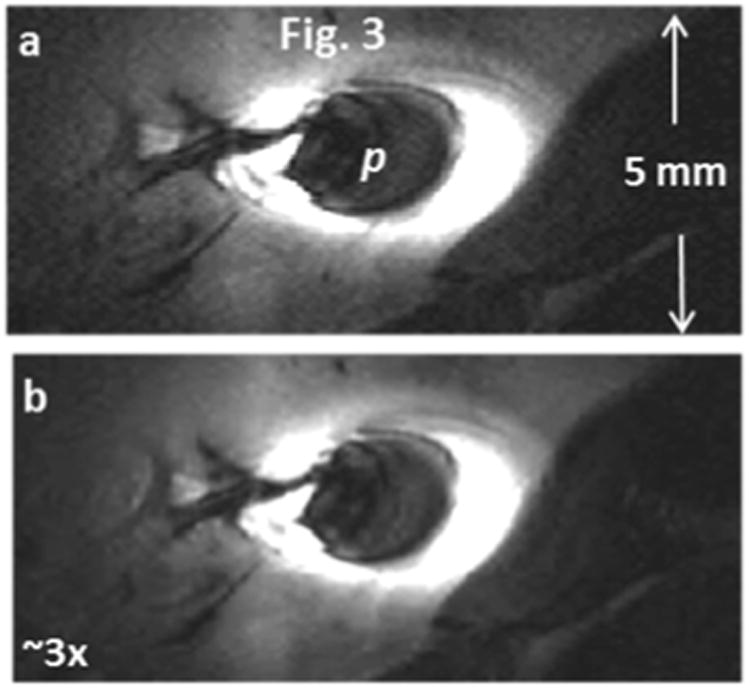
(a) Regular Cartesian MRI endoscopy of a rabbit aorta in vivo (3D GRE; TR/TE=250/12 ms; in-plane resolution 80μm; 3.1 min/5 contiguous slices). (b) Three-fold under-sampling yields a virtually indistinguishable image (cropped for visualization) after compressed-sense reconstruction.
Conclusions
3T IV MRI detectors are ideally suited to compressed sensing and motion correction strategies based on their intrinsically radial and sparsely-localized sensitivity profiles and high signal-to-noise ratios. The benefits are much faster IV MRI–approaching real-time (∼10 fr/s) and reduced motion sensitivity, while retaining the high-resolution (80-300μm) image information.
Acknowledgments
Support: NIH R01 HL090728.
References
- 1.Sathyanarayana S, et al. JACC Cardiovasc Imaging. 2010;3(11):1158–1165. doi: 10.1016/j.jcmg.2010.08.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Block, et al. Magn Reson Med. 2007;57:1086–1098. doi: 10.1002/mrm.21236. [DOI] [PubMed] [Google Scholar]
- 3.Lustig, et al. Magn Reson Med. 2007;58(6):1182–1195. doi: 10.1002/mrm.21391. [DOI] [PubMed] [Google Scholar]