

Abstract
Dystonia is a common movement disorder. A number of monogenic causes have been identified. However, the majority of dystonia cases are not explained by single gene defects. Cervical dystonia is one of the commonest forms without genetic causes identified. This pilot study aimed to identify large effect-size risk loci in cervical dystonia. A genomewide association study (GWAS) was performed. British resident cervical dystonia patients of European descent were genotyped using the Illumina-610-Quad. Comparison was made with controls of European descent from the Wellcome Trust Case Control Consortium using logistic regression algorithm from PLINK. SNPs not genotyped by the array were imputed with 1000 Genomes Project data using the MaCH algorithm and minimac. Postimputation analysis was done with the mach2dat algorithm using a logistic regression model. After quality control measures, 212 cases were compared with 5173 controls. No single SNP passed the genomewide significant level of 5 × 10−8 in the analysis of genotyped SNP in PLINK. Postimputation, there were 5 clusters of SNPs that had P value <5 × 10−6, and the best cluster of SNPs was found near exon 1 of NALCN, (sodium leak channel) with P = 9.76 × 10−7. Several potential regions were found in the GWAS and imputation analysis. The lowest P value was found in NALCN. Dysfunction of this ion channel is a plausible cause for dystonia. Further replication in another cohort is needed to confirm this finding. We make this data publicly available to encourage further analyses of this disorder.
Keywords: cervical dystonia, GWAS, imputation, sodium leaking channel, NALCN
Dystonia is a “syndrome of sustained muscle contractions, frequently causing twisting and repetitive movements or abnormal postures.”1 It is a common movement disorder with an estimated prevalence of 430 per million in the Northern England survey.2,3 The Epidemiological Study of Dystonia in Europe (ESDE) Collaborative Group showed crude annual prevalence rate of 152 per million across 8 European countries.4 The real frequency may be higher as this study might have underestimated the prevalence secondary to underascertainment of cases. An American study online survey on cervical dystonia suggested a prevalence of up to 0.28%.5
Clinical presentation of dystonia is heterogeneous, from focal involvement such as cervical dystonia to generalized torsional dystonia. At present, there are over 20 dystonia loci named, DYT1 to DYT25. Among these, DYT1, DYT3, DYT5, DYT6, DYT8, DYT10, DYT11, DYT12, DYT16, DYT18, CIZ1 (DYT23), ANO3 (DYT24), and GNAL (DYT25) have been cloned.6–10
Cervical dystonia is the most common form of dystonia.3,5,11 A recent Dutch study on focal primary torsion dystonia reported a positive family history in 25% but only 2.4% had Mendelian inheritance pattern among their primary torsion dystonia cases.11 Sixty-four percent (64%) of focal dystonia cases in this Dutch study were cervical dystonia. The majority of cervical dystonia are transmitted in non-Mendelian pattern, which suggests cervical dystonia is likely a complex disease rather than monogenic form. Hitherto, there has been no report of a high-density genomewide association study (GWAS) to identify the loci associated with non-Mendelian dystonia. This study was a pilot attempt to identify any large effect-size loci.
Patients and Methods
Focal cervical dystonia cases were recruited from 2 movement disorders clinics in UK: (1) National Hospital for Neurology and Neurosurgery, London; and (2) Salford Royal Foundation Trust, Manchester. Only cases that remained focal involvement were recruited and most of them were followed up in Botulinum Toxin Clinic. Cases were reviewed by movement disorder specialists, and only presumptive primary cases were recruited, with secondary causes like Wilson’s disease or other neurodegenerative disease ruled out where clinically appropriate. Cases suggestive of Mendelian inheritance were excluded. DYT1 was excluded where necessary. Because of small sample size, subclassification according to family history of movement disorders and age of onset was not attempted. Only cases of assumed European descent were recruited. All patients gave informed consent to the study, approved by the respective local ethics committee. DNA was extracted locally from blood and genotyped in the University College London Genomics Microarray Centre, using Illumina Human 610-Quad BeadChip (Illumina, San Diego, CA, USA).
Control data of European descent was drawn from the Wellcome Trust Case Control Consortium (WTCCC) data set as previously reported.12 A total of 2930 samples from 1958 Birth Cohort and 2737 samples from National Blood Services were genotyped in Illumina 1.2 M Duo array by the Wellcome Trust Sanger Institute. Quality control measure was performed both before and after merging with the cases as detailed in the Supporting Materials.
Genotyped data from cervical dystonia cases was assembled in GenomeStudio (v2011.1) per the manufacturer’s suggestion (Illumina). Postassembly quality control was performed in GenomeStudio and PLINK (version 1.07).13 In brief, genotyping quality of the sample and single-nucleotide polymorphisms (SNPs) were controlled for in GenomeStudio (Illumina). Further checking for gender mismatch, sample relatedness (identity-by-descent, excluding piHat >0.125) (Pi-Hat — a parameter in PLINK using estimates of pairwise IBD to find pairs of individuals who are possibly related.), Hardy-Weinberg equilibrium (excluding P < 1× 10−4), allele frequency (excluding minor allele frequency [MAF] <0.01), nonrandom missingness (missingness-by-haplotype, excluding P <1 × 10−4; missingness-by-genotype, excluding P <1 × 10−4) and population substructure (excluding 6 SD from combined mean of Northern and Western European ancestry (CEU) and Toscani in Italia (TSI) in multidimensional scaling [MDS] component 1 or 2) were performed in PLINK13 (details in Supporting Materials).
The dystonia sample data was merged with the Wellcome Trust Case Control Consortium (WTCCC), and association analysis was performed using logistic regression in the PLINK package.13 Three covariates were used in the regression: gender and the first 2 components of PLINK MDS analysis to adjust for gender and genetic variation. Because of our relatively small sample size, we did not perform separate analysis that looked specifically at known loci.
Imputation for autosomal chromosome was performed with MaCH14 and minimac,15 in chunks of 10 megabases with 1 megabase overlapping at both ends. Other parameters were as suggested by authors (details in the Supporting Materials). Postimputation association was done in mach2dat16 excluding imputed SNPs with r squared (RSQR) <0.3 as suggested. SNPs with MAF <0.03 were not entered into the final analysis. A higher cutoff was chosen as the small sample size in this study contributed to false-positive association in SNPs with low MAF.17 Reference for imputation was taken from the 1000 Genomes Project 2010 August release and composed of 283 individuals from the European continental group.18
Further statistical analysis and plotting were done in R (version 2.11.1).19 Plots of the identified regions were made with Locus Zoom.20
Results
A total of 233 cases were genotyped and 212 cases (66 M, 146 F, mean age 60.6 years, SD 10.9 years) remained after quality control and 494 k SNPs had MAF >0.01 (exclusion breakdown in Supporting Tables 1 and 2). The cases were clustered around the CEU-TSI controls in the MDS plot confirming European descent (Supporting Fig. 1a-c). These were compared with 5173 controls (2609 M, 2564 F) from WTCCC. Quantile-quantile (QQ) plot did not deviate from the expected (Supporting Fig. 3) and lambda was 1.02. No single SNP had reached a genomewide significant association (defined as P < 5 × 10−8). The best signal was rs9416795 (P = 2.00 × 10−6), located in an intergenic region on chromosome 10. This was followed by rs1338041 on chromosome 13, intron region of NALCN, coding for sodium leak channel, nonselective (Fig. 1A, Supporting Table 3).
Figure 1.
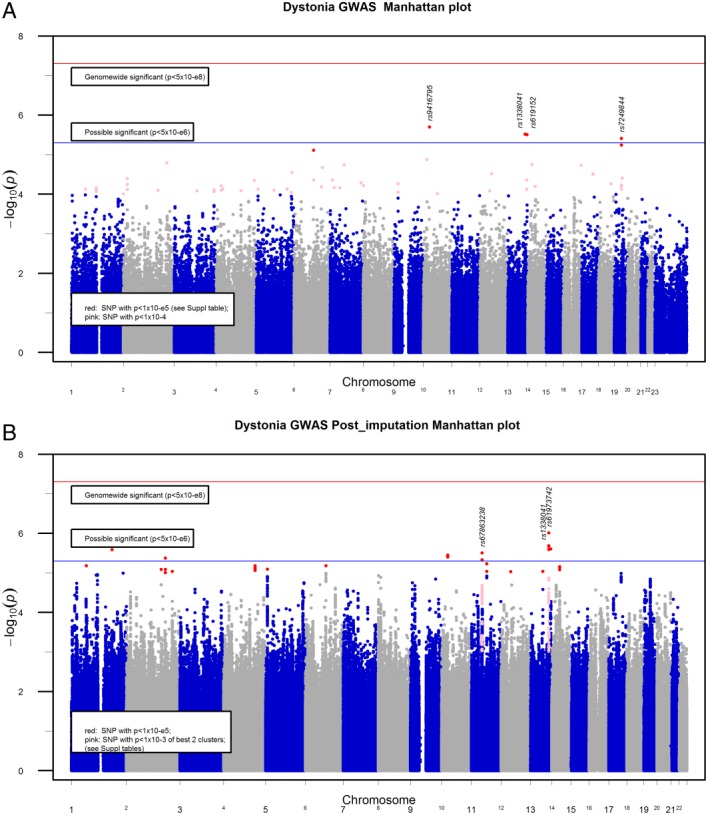
(A) Manhattan plot of GWAS. (B) Manhattan plot of imputed result. The SNPs with P < 0.001 in the best 2 regions were labeled in pink, showing clustering of SNPs around the regions. GWAS, genomewide association study; SNP, single-nucleotide polymorphism. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
After imputation and quality controls (RSQR >0.3 and MAF ≥0.03), there were 5.67 million SNPs available in chromosomes 1 to 22. These had satisfactory genomewide coverage, except a few regions, mainly telomeric and centromeric regions (Manhattan plot, Fig. 1B). The regions not well covered with GWAS and imputation are listed in Supporting Table 7. There were no SNPs with genomewide significance (defined as P < 5 × 10−8). A few clusters of possible associations (defined as P < 5 × 10−6) were found and shown in the Manhattan plot (Fig. 1B, Table 1).
Table 1.
Postimputation SNPs with P value <5 × 10−6
| SNP | CHR | Position | Major allele | Frequency of major allele | RSQRa | Effect 1 | OR | SEM | LR chi square | P value of LR | Symbol | Predicted function | Splice distance |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| rs61973742 | 13 | 102083273 | A | 0.9384 | 0.8881 | 1.579 | 4.848 | 0.415 | 23.9755 | 9.76E-07 | NALCN | 5′ Upstream | |
| rs1338051 | 13 | 102062341 | G | 0.6595 | 0.9932 | −0.481 | 0.618 | 0.1 | 22.5497 | 2.05E-06 | NALCN | Intronic | 6323 |
| rs9518385 | 13 | 102060280 | A | 0.6597 | 0.9947 | −0.48 | 0.618 | 0.1 | 22.5411 | 2.06E-06 | NALCN | Intronic | 8384 |
| rs9518384 | 13 | 102059871 | C | 0.6597 | 0.9951 | −0.48 | 0.619 | 0.1 | 22.5246 | 2.08E-06 | NALCN | Intronic | 8355 |
| rs1338041b | 13 | 102058862 | A | 0.6597 | 0.9955 | −0.48 | 0.619 | 0.1 | 22.4931 | 2.11E-06 | NALCN | Intronic | 7346 |
| rs619152b | 13 | 110939497 | G | 0.6437 | 0.9328 | −0.489 | 0.614 | 0.103 | 22.1724 | 2.49E-06 | COL4A1 | Intronic | 19794 |
| rs3916908 | 13 | 102058054 | A | 0.6602 | 0.9949 | −0.477 | 0.621 | 0.1 | 22.1374 | 2.54E-06 | NALCN | Intronic | 6538 |
| rs12132318 | 1 | 183797688 | T | 0.9376 | 0.3209 | −1.422 | 0.241 | 0.28 | 22.0992 | 2.59E-06 | RGL1 | Intronic | 19012 |
| rs67863238 | 11 | 48267856 | G | 0.9439 | 0.8808 | 1.608 | 4.994 | 0.442 | 21.7354 | 3.13E-06 | OR4X2 | 3′ Downstream | |
| rs1249277 | 10 | 28720076 | G | 0.8497 | 0.9894 | −0.574 | 0.563 | 0.118 | 21.5017 | 3.54E-06 | Intergenic | ||
| rs1249281 | 10 | 28716177 | G | 0.8505 | 0.9956 | −0.572 | 0.564 | 0.118 | 21.3706 | 3.79E-06 | Intergenic | ||
| rs9416795b | 10 | 28709550 | G | 0.8508 | 0.9998 | −0.57 | 0.565 | 0.118 | 21.2877 | 3.95E-06 | Intergenic | ||
| rs10930717 | 2 | 176742322 | G | 0.9524 | 0.9092 | −0.896 | 0.408 | 0.177 | 21.1596 | 4.23E-06 | KIAA1715 | 3′ Upstream | |
| rs35875350 | 11 | 48230490 | G | 0.9433 | 0.9333 | 1.513 | 4.538 | 0.421 | 20.9828 | 4.63E-06 | OR4B1 | 5′ Upstream | |
Quality measure of imputation, from 0 to 1, with values <0.3 suggestive of poorly imputed.
SNP also found in the nonimputed genotype platform.
SNP, single-nucleotide polymorphism; CHR, chromosome; RSQR, r squared (r2); OR, odds ratio; SEM, standard error of the mean; LR, likelihood ratio.
With imputation, the best signals found clustered around NALCN with best P value of 9.8 × 10−7 in rs61973742 and 5 more SNPs in the same gene just short of the best P value. NALCN protein is a sodium leaking channel. The majority of the associated SNPs were found in the first intron between the first and second exon. The remaining were within a few kilobases of the 5′ region of exon 1 and 5′ untranslated region (UTR) (Fig. 2A, Supporting Table 6). The second cluster with peak P at 3.1 × 10−6 was found in rs67863238, chromosome 11 base position 48,267,856 (hg19). This cluster codes for a number of olfactory receptors (OR4X1, OR4X2, OR4S1, and OR4B1) (Fig. 2B, Supporting Table 5).
Figure 2.
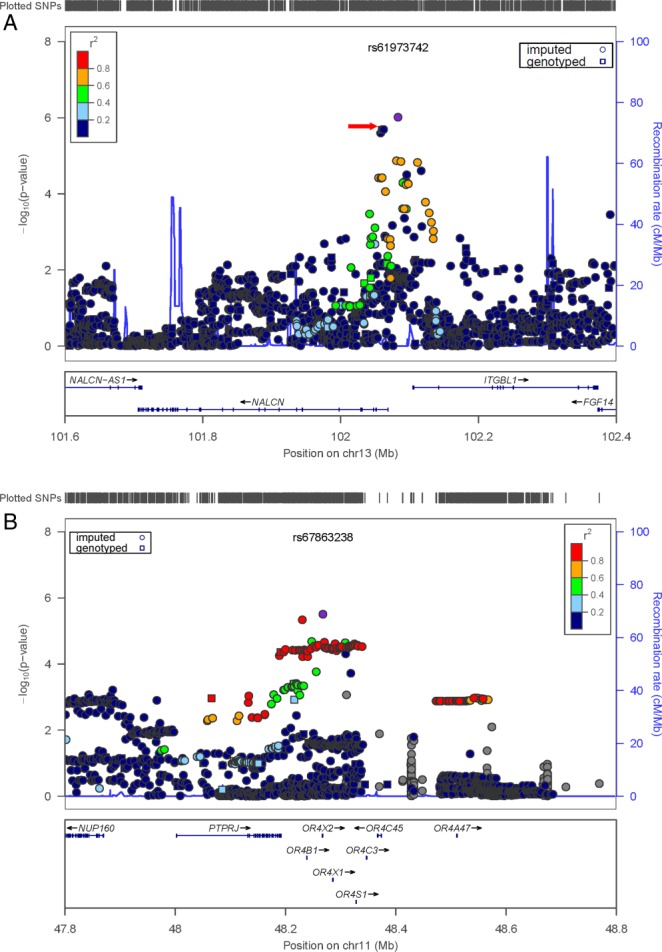
(A) Local association plot with LD of NALCN region (Locus Zoom). There is a cluster of imputed SNPs with P value suggesting possible association. Red arrow is the best GWAS hit (rs1338041) in this region. (B) Local association plot with LD at Chr 11. Tightly linked imputed SNPs suggest possible association of cervical dystonia with an uncommon haplotype in the region that was not well tagged by common SNPs in GWAS. LD, linkage disequilibrium; GWAS, genomewide association study; Chr, chromosome; SNP, single-nucleotide polymorphism. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Remaining imputed SNPs that passed the possible associations were found on chromosome (Chr) 1 RGL1, Chr 2 intergenic 3′ of KIAA1715, Chr 10 intergenic, and Chr 11 COL4A1. The SNPs and local plots of these regions are shown in Supporting Table 4 and Supporting Figures 4 and 5.
Discussion
In this cervical dystonia GWAS, no loci reached a statistically significant association with dystonia. No common SNPs or loci with large effect size were found in dystonia. The most crucial limitation was the small sample size, which was underpowered to detect loci with a smaller disease effect. Assuming MAF of 0.4, odds ratio 1.3, additive model, and prevalence of 430 per million in dystonia, it would need more than 1800 cases to achieve an 80% power.21 If the odds ratio was as high as with the Complement Factor H in macular degeneration,22 the cohort of 212 cases with same assumptions would have a power of almost 100% to detect the SNP. Hence, we conclude that a common SNP with large effect-size is unlikely to be present in idiopathic cervical dystonia, at least in Chr 1 to 22 as shown in Manhattan plot (Fig. 1) and within the regions that were usually genotyped by microarray (Supporting Table 7 for uncovered regions).
The imputation results showed a few clusters of potential significance. The top hit found in NALCN region is interesting. Dysfunction of a sodium channel is a biologically feasible candidate in dystonia. Allelic mutation of SCN8A in mice can present with dystonia.23 Our group has also recently identified mutations in anoctamin (ANO3-DYT23), a calcium-gated chloride channel gene, leading to autosomal dominant craniocervical dystonia.9 This strongly supports an ion channel as a plausible candidate gene for dystonia. Such channels are also potentially pharmacologically modifiable.
NALCN protein is a member of 4 × 6 transmembrane voltage-independent, nonselective, noninactivating ion channel found in all animals studied and universally expressed in mouse brain and spinal cord.24 Our UK Brain Expression Consortium data shows NALCN is universal expressed in brain25 (Supporting Fig. 3). In schizophrenia, the associated SNP in NALCN was rs2044117, located at the last intron.26 The C-terminal end of the protein is the important site in coupling with UNC79 and UNC80 proteins.27 This complex senses calcium level and results in alteration of leaking current and neuronal excitability, comparable to ANO3 as a calcium-gated chloride channel. Mice with exon 1 knocked out die from disrupted respiratory neuronal firing in the brainstem,24 suggesting regions other than the C-terminal are also critical. Our SNPs were clustered around the exon 1 both at 5′ and within the first intron. They may not necessarily be the pathogenic variants but just tagged SNPs. There are a few synonymous and nonsynonymous SNPs found in the exon 1 (rs144447052, rs145910377, rs74707055, rs76774740, rs75606652, rs77203309, rs188237867, rs79047578, and rs9557636). These SNPs are very rare, with MAF well below 0.01 and not included in the imputation and analysis. These may be pathogenic but unidentified rare pathogenic variants tagged to our SNPs are also possible.
Local plot of postimputation SNPs (Fig. 2A, Supporting Table 6) showed multiple SNPs with possible P value identified. This gives support for possible association of this region with cervical dystonia. The best SNP from imputation (rs61973742) has a low r2 with the best SNP rs1338041 in GWAS. There is a great discrepancy of the MAF, 0.062 in rs61973742 and 0.34 in rs1338041. A discrepancy in MAF can lead to low r2 (VanLiere and Rosenberg28 and Wray29). These 2 SNPs have a |D′| = 0.88 despite its low r2 (0.05) in 1000 Genomes 378 European population. Alternatively, there may be a few haplotypes in the region that are pathogenic. GWAS common SNPs tag to 1 haplotype and others discovered through imputation.
The next potential cluster was in Chr 11. It was not found in the initial GWAS, but multiple SNPs with borderline P value were identified from imputation (Supporting Table 5). If replicated, this represents the power of finding new associations that are not well tagged by common SNPs and are identified through haplotypes inferred during imputation. This group of associations, namely OR4X1, OR4X2, OR4S1, and OR4B1, is interesting (Fig. 2B). They belong to the olfactory receptor, family 4, a type of G-protein-coupled receptors (GPCRs). Olfactory function may seem unrelated to dystonia. Recently Fuchs et al.10 reported the association of GNAL mutation with primary torsion dystonia, and the predominant clinical feature in these patients is cervical dystonia. GNAL, coding an olfactory G protein [G(olf)] is found highly expressed in striatum and coupled with the expression of dopamine D1 receptor (DRD1).30 It is located at chromosome 18p. 18p-deletion was reported to be associated with DYT7.31,32 This association was recently challenged.33 The 4 olfactory genes (OR4X1, OR4X2, OR4S1, and OR4B1) are universally expressed in brain and ORB1 is highly expressed in striatum as well (Allen Brain Atlas34).
The GWAS and imputation association analysis employed 2 different algorithms. This may lead to slightly different P values in GWAS and imputation for the same SNP. The 3 other hits found in GWAS were located at intergenic at Chr 6 92 Mb, Chr 10 28 Mb, and Chr 19 29 Mb. The local plots of postimputation SNPs in these regions are shown in Supporting Figure 4. The sparse imputed SNPs around Chr 10 suggested that might be a false-positive result, as were the imputation finding at Chr 1 183 Mb and Chr 2 176 Mb (Supporting Figure 4). The extra SNPs found with imputation at Chr 6 92 Mb and Chr 19 29 Mb suggested potential association. The P value was lower than the best 2 clusters in NALCN and OR4X1 and the functional role within an intergenic region is difficult to predict. Given the recent findings from ENCODE, intergenic region may still play a significant function in transcription.35
In summary, we found a plausible association, though not statistically confirmed, of cervical dystonia with SNPs in the NALCN region. Replication on another cohort of cervical dystonia cases would be essential to confirm the association. As dystonia GWAS is relatively understudied, we make all these data publicly available to encourage further analyses of the problem.
Acknowledgments
We thank the patients for donating their samples in this study.
Supporting Information
References
- Fahn S, Bressman SB, Marsden CD. Classification of dystonia. Adv Neurol. 1998;78:1–10. [PubMed] [Google Scholar]
- Defazio G, Abbruzzese G, Livrea P, Berardelli A. Epidemiology of primary dystonia. Lancet Neurol. 2004;3:673–678. doi: 10.1016/S1474-4422(04)00907-X. [DOI] [PubMed] [Google Scholar]
- Butler AG, Duffey PO, Hawthorne MR, Barnes MP. An epidemiologic survey of dystonia within the entire population of northeast England over the past nine years. Adv Neurol. 2004;94:95–99. [PubMed] [Google Scholar]
- ESDE-Collaborative. A prevalence study of primary dystonia in eight European countries. J Neurol. 2000;247:787–792. doi: 10.1007/s004150070094. [DOI] [PubMed] [Google Scholar]
- Jankovic J, Tsui J, Bergeron C. Prevalence of cervical dystonia and spasmodic torticollis in the United States general population. Parkinsonism Relat Disord. 2007;13:411–416. doi: 10.1016/j.parkreldis.2007.02.005. [DOI] [PubMed] [Google Scholar]
- Fuchs T, Ozelius LJ. Genetics of dystonia. Semin Neurol. 2011;31:441–448. doi: 10.1055/s-0031-1299783. [DOI] [PubMed] [Google Scholar]
- Chen WJ, Lin Y, Xiong ZQ, et al. Exome sequencing identifies truncating mutations in PRRT2 that cause paroxysmal kinesigenic dyskinesia. Nat Genet. 2011;43:1252–1255. doi: 10.1038/ng.1008. [DOI] [PubMed] [Google Scholar]
- Xiao J, Uitti RJ, Zhao Y, et al. Mutations in CIZ1 cause adult onset primary cervical dystonia. Ann Neurol. 2012;71:458–469. doi: 10.1002/ana.23547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Charlesworth G, Plagnol V, Holmström KM, et al. Mutations in Ano3 cause dominant craniocervical dystonia: ion channel implicated in pathogenesis. Am J Hum Genet. 2012;91:1041–1050. doi: 10.1016/j.ajhg.2012.10.024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fuchs T, Saunders-Pullman R, Masuho I, et al. Mutations in GNAL cause primary torsion dystonia. Nat Genet. 2012;45:88–92. doi: 10.1038/ng.2496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Groen JL, Kallen MC, van de Warrenburg BP, et al. Phenotypes and genetic architecture of focal primary torsion dystonia. J Neurol Neurosurg Psychiatry. 2012;83:1006–1011. doi: 10.1136/jnnp-2012-302729. [DOI] [PubMed] [Google Scholar]
- Wellcome Trust Case Control Consortium. Genome-wide association study of 14,000 cases of seven common diseases and 3,000 shared controls. Nature. 2007;447:661–678. doi: 10.1038/nature05911. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Purcell S, Neale B, Todd-Brown K, et al. PLINK: a tool set for whole-genome association and population-based linkage analyses. Am J Hum Genet. 2007;81:559–575. doi: 10.1086/519795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li Y, Willer CJ, Ding J, Scheet P, Abecasis GR. MaCH: using sequence and genotype data to estimate haplotypes and unobserved genotypes. Genet Epidemiol. 2010;34:816–834. doi: 10.1002/gepi.20533. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howie B, Fuchsberger C, Stephens M, Marchini J, Abecasis GR. Fast and accurate genotype imputation in genome-wide association studies through pre-phasing. Nat Genet. 2012;44:955–959. doi: 10.1038/ng.2354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Li Y, Abecasis G. mach2dat v1.0.18.tgz. Available at URL: http://www.sph.umich.edu/csg/yli/mach/download/mach2dat.source.1.0.18.tgz. Accessed Feb 2011.
- Weale M. Quality control for genome-wide association studies. In: Barnes MR, Breen G, editors. Genetic Variation: Methods and Protocols. Vol. 628. New York: Springer Science + Business Media; 2010. Series: Methods in Molecular Biology. [Google Scholar]
- University of Michigan Center for Statistical Genetics. 1000 Genomes (v 2010-08) Download. Available at URL: http://www.sph.umich.edu/csg/abecasis/MaCH/download/1000G-2010-08.html, Accessed March 2011.
- R Development Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2008. [Google Scholar]
- Pruim RJ, Welch RP, Sanna S, et al. LocusZoom: regional visualization of genome-wide association scan results. Bioinformatics. 2010;26:2336–2337. doi: 10.1093/bioinformatics/btq419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skol AD, Scott LJ, Abecasis GR, Boehnke M. Joint analysis is more efficient than replication-based analysis for two-stage genome-wide association studies. Nat Genet. 2006;38:209–213. doi: 10.1038/ng1706. [DOI] [PubMed] [Google Scholar]
- Klein RJ, Zeiss C, Chew EY, et al. Complement factor H polymorphism in age-related macular degeneration. Science. 2005;308:385–389. doi: 10.1126/science.1109557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meisler MH, Plummer NW, Burgess DL, Buchner DA, Sprunger LK. Allelic mutations of the sodium channel SCN8A reveal multiple cellular and physiological functions. Genetica. 2004;122:37–45. doi: 10.1007/s10709-004-1441-9. [DOI] [PubMed] [Google Scholar]
- Lu B, Su Y, Das S, Liu J, Xia J, Ren D. The neuronal channel NALCN contributes resting sodium permeability and is required for normal respiratory rhythm. Cell. 2007;129:371–383. doi: 10.1016/j.cell.2007.02.041. [DOI] [PubMed] [Google Scholar]
- Trabzuni D, Ryten M, Walker R, et al. Quality control parameters on a large dataset of regionally dissected human control brains for whole genome expression studies. J Neurochem. 2011;119:275–282. doi: 10.1111/j.1471-4159.2011.07432.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang KS, Liu XF, Aragam N. A genome-wide meta-analysis identifies novel loci associated with schizophrenia and bipolar disorder. Schizophr Res. 2010;124(1-3):192–199. doi: 10.1016/j.schres.2010.09.002. [DOI] [PubMed] [Google Scholar]
- Lu B, Zhang Q, Wang H, Wang Y, Nakayama M, Ren D. Extracellular calcium controls background current and neuronal excitability via an UNC79-UNC80-NALCN cation channel complex. Neuron. 2010;68:488–499. doi: 10.1016/j.neuron.2010.09.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- VanLiere JM, Rosenberg NA. Mathematical properties of the r2 measure of linkage disequilibrium. Theor Popul Biol. 2008;74:130–137. doi: 10.1016/j.tpb.2008.05.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wray NR. Allele frequencies and the r2 measure of linkage disequilibrium: impact on design and interpretation of association studies. Twin Res Hum Genet. 2005;8:87–94. doi: 10.1375/1832427053738827. [DOI] [PubMed] [Google Scholar]
- Herve D, Levi-Strauss M, Marey-Semper I, et al. G(olf) and Gs in rat basal ganglia: possible involvement of G(olf) in the coupling of dopamine D1 receptor with adenylyl cyclase. J Neurosci. 1993;13:2237–2248. doi: 10.1523/JNEUROSCI.13-05-02237.1993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leube B, Rudnicki D, Ratzlaff T, Kessler KR, Benecke R, Auburger G. Idiopathic torsion dystonia: assignment of a gene to chromosome 18p in a German family with adult onset, autosomal dominant inheritance and purely focal distribution. Hum Mol Genet. 1996;5:1673–1677. doi: 10.1093/hmg/5.10.1673. [DOI] [PubMed] [Google Scholar]
- Klein C, Page CE, LeWitt P, et al. Genetic analysis of three patients with an 18p- syndrome and dystonia. Neurology. 1999;52:649–651. doi: 10.1212/wnl.52.3.649. [DOI] [PubMed] [Google Scholar]
- Winter P, Kamm C, Biskup S, et al. DYT7 gene locus for cervical dystonia on chromosome 18p is questionable. Mov Disord. 2012;27:1820–1822. doi: 10.1002/mds.25219. [DOI] [PubMed] [Google Scholar]
- Hawrylycz MJ, Lein ES, Guillozet-Bongaarts AL, et al. An anatomically comprehensive atlas of the adult human brain transcriptome. Nature. 2012;489:391–399. doi: 10.1038/nature11405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Djebali S, Davis CA, Merkel A, et al. Landscape of transcription in human cells. Nature. 2012;489:101–108. doi: 10.1038/nature11233. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.