

Abstract
The 2014 American Diabetes Association guidelines denote four means of diagnosing diabetes. The first of these is a glycosylated hemoglobin (HbA1c) >6.5%. This literature review summarizes studies (n=47) in the USA examining the significance, strengths, and limitations of using HbA1c as a diagnostic tool for diabetes, relative to other available means. Due to the relatively recent adoption of HbA1c as a diabetes mellitus diagnostic tool, a hybrid systematic, truncated review of the literature was implemented. Based on these studies, we conclude that HbA1c screening for diabetes has been found to be convenient and effective in diagnosing diabetes. HbA1c screening is particularly helpful in community-based and acute care settings where tests requiring fasting are not practical. Using HbA1c to diagnose diabetes also has some limitations. For instance, HbA1c testing may underestimate the prevalence of diabetes, particularly among whites. Because this bias differs by racial group, prevalence and resulting estimates of health disparities based on HbA1c screening differ from those based on other methods of diagnosis. In addition, existing evidence suggests that HbA1c screening may not be valid in certain subgroups, such as children, women with gestational diabetes, patients with human immunodeficiency virus, and those with prediabetes. Further guidelines are needed to clarify the appropriate use of HbA1c screening in these populations.
Keywords: diabetes mellitus, diagnosis, glycosylated hemoglobin, USA
Introduction
The Centers for Disease Control and Prevention estimate that 18.8 million people in the USA over the age of 20 years have been diagnosed with diabetes and that another 7 million have diabetes but remain undiagnosed.1 The number of people with diabetes in the USA recently rose by 3 million over a 2-year period. Undiagnosed diabetes is particularly concerning, because careful management of diabetes, in terms of eating healthy, remaining active, and taking appropriate medications, has been shown to reduce the risk of adverse events, including myocardial infarction, cerebrovascular accident, end-stage renal disease, blindness, foot ulceration, and amputation.2
Until recently, the diagnosis of diabetes mellitus was determined solely by glucose concentration on the basis of the results of two tests: two fasting plasma glucose (FPG) tests, two oral glucose tolerance tests (OGTTs), or one of each performed on separate days close together in time. In 1993, the Diabetes Control and Complications Trial established the importance of HbA1c as an indicator of risk for microvascular complications of diabetes, such as blindness, kidney disease, and nerve damage; however, it was not until 2009 that the International Expert Committee recommended use of HbA1c for diagnosis of diabetes.3
The rationale for the use of HbA1c for diagnostic purposes is largely based upon data showing that the microvascular complications of diabetes (retinopathy, nephropathy, and neuropathy) tend to occur in patients with HbA1c ≥6.5%. The strength of the relationship between HbA1c and these complications is as strong as other definitions of diabetes, including FPG or OGTT. The consensus of the committee was that HbA1c screening should be used whenever possible to diagnose diabetes, in part due to its convenience.
The committee determined that an HbA1c ≥6.5% was the most reliable indicator of the presence of diabetes. Patients with an HbA1c between 6% and 6.4% were considered to be at high risk for developing diabetes. The committee acknowledged, however, that HbA1c cannot be used in patients with certain conditions, such as hemolytic anemia or in those with a recent blood transfusion. Moreover, as HbA1c screening may be considered costly in some settings, the FPG and OGTT tests can still be used in certain cases. The goal of this manuscript is to review existing literature on the role of HbA1c in diagnosing diabetes in the USA.
Methodology
A hybrid of a systematic and truncated review was implemented for the literature due to the relatively recent adoption of HbA1c as a diagnostic tool for diabetes mellitus. The systematic review worksheet created by the Memorial Sloan-Kettering Cancer Center was utilized to establish the parameters for this review, using the following parameters:
Patients/population or condition (diabetes mellitus patients in the USA)
Intervention or exposure (diagnosis test using HbA1c)
Comparison(s) (against other diagnostic tests for diabetes mellitus)
Outcome(s) (validity of HbA1c as a diagnostic tool for diabetes mellitus)
Sex (both)
Age groups (all)
Literature time frame (current year +10)
Language (English)
Publication types (clinical trials, comparative study, controlled clinical trial, evaluation study, government publications, guidelines, historical article, meta-analysis, observational study, pragmatic clinical trial, randomized controlled trials, research support retraction of publication, review, scientific integrity review, systematic review, technical report, validation studies)
Document types (primary research articles, review articles, editorials/opinion/commentary/perspectives, meetings or conference abstracts, white papers, gray literature, article comments [formal, reviewed], dissertations/thesis, technical papers)
Databases (PubMed, Medline, ClinicalTrials, PubMed Health, PubMed Central, Clinical Pharmacology, Cochrane Library, Facts and Comparisons, SciFinder)
Citation management tool (RefWorks)
PubMed search terms and strategies (diabetes mellitus/diagnosis [MeSH] AND hemoglobin A, glycated [MeSH] AND USA [ad]).
Related citations were also investigated for their relevance. The MeSH search strategy resulted in 521 articles within the National Center for Biotechnology Information, US National Library of Medicine databases. The additional filters of 10 years and humans reduced the results to 391. Similar search strategies were run through Clinical Queries and the above-mentioned databases, increasing the relevant articles to 408 for review. HWS performed the initial literature searches. HWS and DTJ then removed articles that did not seem relevant after reading the abstracts (n=361). The remaining 47 articles were divided between DTJ, RG, KMD, and CLM for review and article summary. The bibliographic manager RefWorks was utilized to maintain control of all citations and their abstracts for tracking, reconsideration, and dissemination. The selection and retention strategy is depicted in Figure 1.
Figure 1.
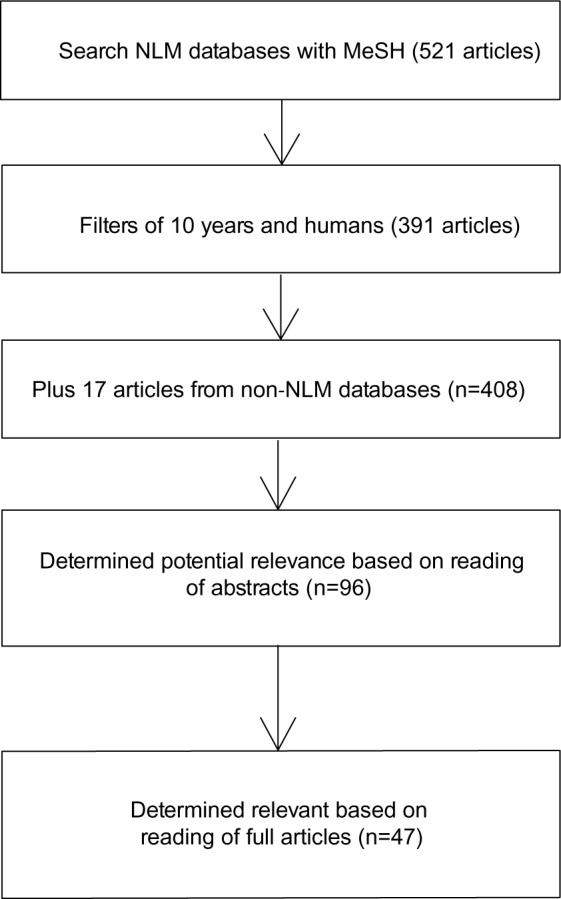
Article search and selection strategy.
Abbreviation: NLM, National Library of Medicine.
Measurement and standardization
HbA1c testing measures average blood glucose levels over the past 2–3 months in terms of the concentration of hemoglobin molecules that have glucose attached to them. It is reported as a percentage. The use of HbA1c for screening and diagnosis of patients with diabetes offers advantages in terms of ease of use over other tests as it does not require patients to fast overnight or for 2 hours after the administration of oral glucose.
In the past, a limitation of HbA1c screening in diagnosing diabetes was that diverse methods had been used in HbA1c assays and there was no standardization of the test. Hence, identifying a cut-off diagnostic HbA1c value was difficult to achieve.4 This shortcoming was addressed by the establishment of the National Glycohemoglobin Standardization Program (NGSP). NGSP standards stated that any local assay should be made traceable to the assay used by the Diabetes Control and Complications Trial.
Existing guidelines
The American Diabetes Association first published guidelines for diagnosing diabetes in 1997; however, they did not include HbA1c as a screening tool until 2010. Figure 2 summarizes the four recommended alternatives for diagnosing diabetes. The guidelines emphasized that HbA1c assays be standardized to the Diabetes Control and Complications Trial HbA1c assay, and certified by the NGSP.
Figure 2.
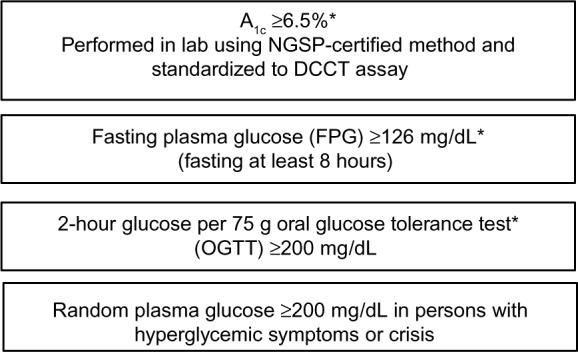
Four alternative means of diagnosing diabetes.
Notes: *Should be retested for confirmation in absence of unequivocal hyperglycemia.
Abbreviations: A1c, Hemoglobin A1c; DCCT, Diabetes Control and Complications Trial; NGSP, National Glycohemoglobin Standardization Program.
Screening criteria for diabetes remained unchanged. All patients with factors that put them at high risk should be screened regardless of age. For those without risk factors, screening should begin at age 45 years and be repeated every 3 years. The new American Diabetes Association guidelines also introduced a new category of intermediate dysglycemia, called the “increased-risk” group (HbA1c 5.7%–6.4%), to describe individuals with what is also known as “prediabetes.”
Subsequently, other organizations, including the American Association of Clinical Endocrinologists, the World Health Organization, the European Association for the Study of Diabetes, and the International Diabetes Federation, have endorsed HbA1c for the diagnosis of diabetes.
Usefulness of HbA1c as an effective diagnostic tool
Validity
Results of the National Health and Nutrition Examination Survey (NHANES) supported the recommendation by the International Expert Committee as well as the American Diabetes Association to implement use of HbA1c to diagnose diabetes, as HbA1c and FPG similarly classified diabetes 97.7% of the time.5
In another study, Eid and Pottala used a receiver operating curve to determine that an HbA1c ≥6.3% provided the most accurate cut-off measurement for diagnosing diabetes within a chronic disease management system, particularly within high-risk populations. This cut-off measurement was associated with a sensitivity of 70% and a specificity of 85%, showing strong diagnostic evidence for diabetes.6 Although measurement of HbA1c has the advantage of not being subject to the preanalytical variations that affect other blood glucose measurements, such as acute illness, short-term lifestyle modifications, food ingestion, or variations in the handling of samples, there are factors that may affect the validity of HbA1c measurements, including iron deficiency, altered hemoglobin structure or erythrocyte lifespan, and interracial variability in hemoglobin.7
Usefulness in the community
Due to its ease of use, several studies have found that HbA1c testing can identify patients in the community who might otherwise go undiagnosed. A study by Grant et al found that community-based HbA1c screening can be used to identify many patients at risk for diabetes or with undiagnosed diabetes at churches, group homes, shelters, community centers, and street corners.8 Similarly, Nam et al found that community-based point-of-care (POC) testing of Korean Americans, with reference-based follow-up, was an effective means of identifying diabetes in an otherwise hard-to-reach population.9
Acute setting
A number of other studies in the USA have found HbA1c screening to be a useful diagnostic tool in acute settings, which can be used to take advantage of the greater interest that some patients take in their health during times of acute illness. A study performed by Silverman et al found an HbA1c of 5.7% as the optimal screening cut-off for prediabetes, and 6.0% for optimal screening of diabetes in acute care settings. When used, these criteria effectively identified high-risk individuals who require referral for additional evaluation and management.10 A study examining usefulness of HbA1c screening in the emergency department found that assessment in the emergency setting did not differ substantially from that observed 45 days later in outpatient follow-up.11 Using POC HbA1c testing in an emergency department, Menchine et al found a high prevalence of undiagnosed diabetes in Hispanics (14%), African Americans (27%), and patients with body mass index ≥30 kg/m2 (22%).12 Moreover, Magee and Nassar found that POC HbA1c testing in the emergency department enabled the treating physician and educator to manage patients appropriately.13 This resulted in improved glycemic control at 2 weeks post initiation of treatment at the emergency department visit. Another study, however, found that only 38% of patients who screened positive on HbA1c tests for diabetes during an emergency department visit also tested positive on an OGTT during follow-up.14
As a predictor for future diabetes
A Department of Veterans Affairs Medical Center study concluded that patients with high–normal HbA1c values may require follow-up sooner than 3 years, especially overweight or obese patients. In this outpatient population, HbA1c was a stronger predictor than obesity of a future diagnosis of diabetes.15
Another historical analysis of data involving Veterans Affairs Medical Centers revealed that individuals with an elevated baseline HbA1c (≥5.0%) had a significant risk of developing diabetes over an 8-year follow-up period. Investigators found that the risk of developing diabetes yielded an odds ratio exceeding 16 in those with an HbA1c of 6.0%–6.4%, with an 80% cumulative incidence of diabetes.16 Moreover, Abdul-Ghani et al utilized the area under a receiver operating curve to determine that HbA1c was a significant predictor of a future diagnosis of diabetes, with an HbA1c cut-off of 5.65% yielding the greatest sensitivity and specificity, although HbA1c had a smaller area under the curve than the 1-hour plasma glucose concentration in a multivariate logistic model that included anthropometric parameters, lipid profile, and FPG.17 Given these results, a combination of dual HbA1c and FPG may be a better predictor of future diabetes. A study performed by Selvin et al concluded that dual HbA1c and FPG levels are strong predictors of risk and diagnosis of diabetes, demonstrating that an HbA1c cut-off of 6.5% was both highly specific and reasonably sensitive in linking HbA1c levels to the risk of long-term microvascular and macrovascular outcomes in nondiabetic adults.18
A recent opinion piece in the Journal of the American Medical Association concluded that HbA1c remains the only test that can predict the microvascular complications of diabetes and for which there are generally accepted therapeutic targets. HbA1c can be measured accurately in the majority of patients and provides valuable information to help guide treatment decisions.19
Limitations of HbA1c as a diagnostic tool
Results differ from other tests
When diagnosing prediabetes, a recent study by Gosmanov and Wan found that HbA1c testing had a low positive predictive value of 39% using a 75 g OGTT as the gold standard.20 In another study, Lipska et al compared HbA1c screening with FPG in an elderly cohort from the Health, Aging, and Body Composition study.21 Only 80 patients were found to have undiagnosed diabetes, and an equal number were identified solely by one method or simultaneously by both: 27.5% (n=22) only by FPG, 36.3% (n=29) only by HbA1c, and 36.3% (n=29) by both methods. They also found that elderly blacks and women were significantly more likely to be identified with diabetes by HbA1c than by FPG. Moreover, NHANES data revealed that the use of HbA1c in screening resulted in a one-third lower prevalence of undiagnosed diabetes than FPG or 2-hour glucose testing.22
In another study comparing HbA1c screening with both FPG and 2-hour glucose, HbA1c had low sensitivity and high specificity for identifying diabetes and prediabetes, and the authors concluded that the data supported greater use of the OGTT and both FPG and 2-hour glucose values for diagnosis of diabetes and prediabetes.23
Another study enrolled patients in a clinic-based diabetes prevention program and found that reliance on HbA1c alone to screen and enroll patients in the program would have missed one-third of eligible high-risk patients (HbA1c defined as 6.0%–6.4%) as compared with the OGTT.24 Similarly, Fajans et al reported that nearly one-third of subjects found to have prediabetes and impaired glucose tolerance via plasma glucose concentrations had an HbA1c <5.7%, indicating that HbA1c lacks sensitivity and reliability for diagnosing prediabetes or impaired glucose tolerance.25
Investigators wishing to determine the distribution of normal versus increased HbA1c levels in individuals who had undergone a 2-hour OGTT found that nearly two-thirds diagnosed with diabetes via OGTT had normal HbA1c levels.26 An analysis of Native American (46%) subjects from the Strong Heart Study demonstrated that HbA1c alone detected fewer cases of prevalent diabetes compared with FPG in the initial screening; however, neither test done alone will effectively identify diabetes, and the authors concluded that using both FPG and HbA1c together will identify a larger group at risk, since HbA1c might detect subjects who are missed by FPG and vice versa.27 A study that tested same-visit HbA1c at a family practice center compared with three laboratory HbA1c methods demonstrated that same-visit HbA1c results were significantly lower than those found with the three laboratory methods.28
Racial disparities
Not only do estimates of the prevalence of diabetes depend on which screening test is used, administering HbA1c instead of FPG affects estimates of the prevalence of diabetes differently in different racial or ethnic groups. In 2011, Getaneh et al found substantial discrepancies in prevalence by race and ethnicity when using HbA1c compared with FPG as a screening tool. Of patients diagnosed as having diabetes by FPG, HbA1c screening did not identify diabetes in 64.5% of white, 46.1% of Dominican, 44.0% of African-American, and 41.9% of Hispanic subjects.29 Similarly, a study by Vable et al using NHANES data found that the estimated prevalence of diabetes in non-Hispanic whites was halved when using HbA1c instead of FPG. In contrast, for Hispanics and non-Hispanic blacks, there was no significant change in the estimated prevalence.30
Additional NHANES data showed disproportionate differences using HbA1c criteria with respect to race; there was a two-fold increase in non-Hispanic blacks and Mexican-Americans versus non-Hispanic whites for diagnosed, undiagnosed, and both types of diabetes.22 However, a recent study by Tsugawa et al concluded that even though HbA1c levels are higher in blacks than in whites at any given glycemic level, the fact that the risk of retinopathy starts to increase at a lower HbA1c level in blacks than in whites suggests that the cut-off does not need to be changed for blacks.31
Another study found that factors associated with a diabetes diagnosis differed by type of screening. In a multiethnic middle-school cohort, high-risk HbA1c (5.7%–6.4%) was associated with non-Hispanic black race, a family history of diabetes, and higher measurements of body mass index, waist circumference, and fasting insulin levels, whereas impaired fasting glucose was associated with Hispanic ethnicity, and increased body mass index, waist circumference, and fasting insulin levels, as well as increased frequency of hypertension and hypertriglyceridemia.32 A study performed by Olson et al found discrepancies within white and black racial groups with regard to both the International Expert Committee and American Diabetes Association diagnostic criteria. Both criteria demonstrated limitations in their use in screening, as both had high specificity but low sensitivity.33
Among Filipino-Americans, Japanese-Americans and native Hawaiians, the use of HbA1c resulted in lower sensitivity and was estimated to have missed a diagnosis in 60% of those newly diagnosed with diabetes when compared with the OGTT.34
Gestational diabetes
Diagnosing gestational diabetes using HbA1c tests also raises some concerns. In a review article, Malkani and DeSilva noted that consensus on diagnostic criteria for gestational diabetes is sorely needed.35 While HbA1c is not routinely used to diagnose gestational diabetes, it has been used to determine the need for medication in expecting mothers. Clayton et al found that a POC HbA1c of 5.72% significantly indicated a need for medication; however, a very close mean POC HbA1c of 5.4% was associated with no need. A slight correlation was seen between POC HbA1c and FPG. Based on overlap of results, the large standard deviations, and the small sample size of their study, the authors were unable to determine a cut-off for POC HbA1c and concluded that larger trials are needed.36
Children
One retrospective study analyzed 206 children with diabetes and found that, in 10% of cases, the initial diabetes diagnosis was misclassified, with HbA1c being significantly higher in those initially misclassified as type 1 versus type 2. The authors concluded that the initial classification of diabetes on the basis of HbA1c may not be a reliable predictor of classification in children.37
Children are more frequently afflicted with type 1 diabetes, which is associated with more rapidly developed and transient hyperglycemia that might go undetected with an HbA1c test. A study performed by Vehik et al found that the diagnostic criterion of HbA1c >6.5% was not a sensitive indicator of type 1 diabetes in high-risk subjects younger than 21 years of age due to the sensitivity of the test. Decreasing the threshold and checking for an HbA1c increase over time may be a more appropriate indicator for type 1 diabetes.38 Another study performed by Sharma and Fleming comparing HbA1c with other prediabetic diagnostic tests in diagnosing prediabetes in high-risk African-American children concluded that HbA1c is not sensitive enough at a cut-off of 5.7% for prediabetes screening in children, when compared with either FPG or HOMA-IR (calculated homeostasis model assessment of insulin resistance). Additionally, no correlation was seen in HbA1c levels between obese and overweight children, nor any difference in HbA1c levels between boys and girls.39
A multiethnic cohort study conducted by Nowicka et al tested the sensitivity and specificity of HbA1c in the diagnosis of type 2 diabetes and prediabetes compared with the OGTT. Of the 1,156 obese children and adolescents without a diagnosis of diabetes, 77% had normal HbA1c (<5.7%), demonstrating that HbA1c would underestimate the diagnosis of prediabetes and type 2 diabetes due to the specificity and sensitivity of the test.40
In contrast with the previous studies, an analysis performed by Shah et al found that HbA1c was a good predictor of type 2 diabetes in obese children, particularly those with insulin resistance. HbA1c ≥6% demonstrated a sensitivity and specificity of 99% and 96%, respectively. However, the authors did acknowledge that the difficulties in standardizing HbA1c assays in the community may affect the applicability of their study.41
Women
A study by Pradhan et al attempted to determine if an elevated HbA1c level would be a good predictor of cardiovascular disease and type 2 diabetes in women. A study of 26,563 women showed that baseline HbA1c is a good predictor for type 2 diabetes, but not for cardiovascular health, in middle-aged and older women. The study also showed that the risk for diabetes increases even when levels of HbA1c were considered to be in the normal range. The authors emphasized that these findings cannot be generalized to different groups (eg, adolescents and men).42
Elderly
The NHANES data showed that when using the HbA1c test, the prevalence of undiagnosed diabetes or high-risk diabetes is strongly influenced by increasing age.22
Other considerations
Data from NHANES showed that in patients with high or low hemoglobin concentrations, HbA1c should be used with caution to diagnose diabetes or prediabetes, since changes in erythrocyte turnover may alter test results. HbA1c was higher in patients with iron deficiency anemia, who had HbA1c levels similar to those with normal hemoglobin and iron status. When groups of anemic and nonanemic patients with and without iron deficiency were studied individually, there was no difference in the relationship between FPG and HbA1c in this population.43
Human immunodeficiency virus
The usefulness of HbA1c as a screening tool for diabetes in patients with human immunodeficiency virus (HIV) is unclear. In one study of patients with HIV, HbA1c was a more accurate screening tool for diabetes than FPG, as without any confirmatory criterion, FPG was found to overestimate the incidence of diabetes in HIV patients.44 However, Eckhardt et al concluded that HbA1c values are insensitive, although highly specific, for diagnosing diabetes in patients with HIV. Additionally, HbA1c may be affected by current antiretroviral medications, with overestimation of HbA1c in those currently receiving protease inhibitors and underestimation in those currently receiving non-nucleoside reverse-transcriptase inhibitors, with the exception of tenofovir.45
Discussion
As the prevalence of diabetes continues to rise in the USA, means of screening high-risk and hard-to-reach populations has become increasingly important. Because HbA1c levels have been associated with an increased risk of diabetes-related complications, and HbA1c screening provides a convenient way to diagnose diabetes, guidelines have begun to advocate use of HbA1c to diagnose diabetes.46–48 Limitations include the prevalence of estimates based on HbA1c differing from those of other methods of diagnosis, particularly among white patients. Moreover, the usefulness and validity of HbA1c screening in certain populations has been questioned. Hence, for certain subgroups, multiple methods may be needed. For example, using FPG in addition to HbA1c may be the best method for screening for diabetes in HIV patients.45 Another disadvantage is that HbA1c screening has been found to be less cost-effective than a 2-hour OGTT, a 1-hour glucose challenge test, or random glucose testing.49 Hence, it might be useful to implement risk stratification, which has been shown to improve the predictive power of HbA1c screening for diabetes and may be more cost-effective than opportunistic screening.14
Acknowledgments
The contribution of DTJ to this article was supported in part by a grant (P20MD000173) from the National Institute for Minority Health and Health Disparities of the National Institutes of Health.
Footnotes
Disclosure
The authors report no conflicts of interest with this work.
References
- 1.Centers for Disease Control and Prevention . National Diabetes Fact Sheet: National Estimates and General Information on Diabetes and Prediabetes in the United States, 2011. Atlanta, GA, USA: Department of Health and Human Services, Centers for Disease Control and Prevention; 2011. [Google Scholar]
- 2.Boyle JP, Thompson TJ, Gregg EW, Barker LE, Williamson DF. Projection of the year 2050 burden of diabetes in the US adult population: dynamic modeling of incidence, mortality, and prediabetes prevalence. Popul Health Metr. 2010;8:29. doi: 10.1186/1478-7954-8-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.International Expert Committee International Expert Committee report on the role of the A1c assay in the diagnosis of diabetes. Diabetes Care. 2009;32:1327–1334. doi: 10.2337/dc09-9033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Little RR, Rohlfing CL, Wiedmeyer HM, et al. The national glycohemoglobin standardization program: a five-year progress report. Clin Chem. 2001;47:1985–1992. [PubMed] [Google Scholar]
- 5.Carson AP, Fox CS, McGuire DK, et al. Low hemoglobin A1c and risk of all-cause mortality among US adults without diabetes. Circ Cardiovasc Qual Outcomes. 2010;3:661–667. doi: 10.1161/CIRCOUTCOMES.110.957936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Eid WE, Pottala JV. Value of hemoglobin A1c in diagnosing diabetes mellitus within a chronic disease management system illustrated by the receiver operating characteristic curve. Endocr Pract. 2010;16:14–20. doi: 10.4158/EP09135.OR. [DOI] [PubMed] [Google Scholar]
- 7.Sacks DB, Arnold M, Bakris GL, et al. Guidelines and recommendations for laboratory analysis in the diagnosis and management of diabetes mellitus. Diabetes Care. 2011;34:e61–e99. doi: 10.2337/dc11-9998. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Grant T, Soriano Y, Marantz PR, et al. Community-based screening for cardiovascular disease and diabetes using HbA1c. Am J Prev Med. 2004;26:271–275. doi: 10.1016/j.amepre.2003.12.015. [DOI] [PubMed] [Google Scholar]
- 9.Nam S, Han HR, Song HJ, Song Y, Kim KB, Kim MT. Utility of a point-of-care device in recruiting ethnic minorities for diabetes research with community partners. J Health Care Poor Underserved. 2011;22:1253–1263. doi: 10.1353/hpu.2011.0117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Silverman RA, Thakker U, Ellman T, et al. Hemoglobin A1c as a screen for previously undiagnosed prediabetes and diabetes in an acute-care setting. Diabetes Care. 2011;34:1908–1912. doi: 10.2337/dc10-0996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Thakker U, Ellman T, Magleby R, Graff K, Kelson J, Silverman RA. The impact of acute illness on HbA(1c) determination of undiagnosed diabetes. Diabetes Metab Res Rev. 2012;28:603–607. doi: 10.1002/dmrr.2315. [DOI] [PubMed] [Google Scholar]
- 12.Menchine MD, Arora S, Camargo CA, Ginde AA. Prevalence of undiagnosed and suboptimally controlled diabetes by point-of-care HbA1c in unselected emergency department patients. Acad Emerg Med. 2011;18:326–329. doi: 10.1111/j.1553-2712.2011.01014.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Magee MF, Nassar C. Hemoglobin A1c testing in an emergency department. J Diabetes Sci Technol. 2011;5:1437–1443. doi: 10.1177/193229681100500615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ginde AA, Cagliero E, Nathan DM, Camargo CA., Jr Point-of-care glucose and hemoglobin A1c in emergency department patients without known diabetes: implications for opportunistic screening. Acad Emerg Med. 2008;15:1241–1247. doi: 10.1111/j.1553-2712.2008.00240.x. [DOI] [PubMed] [Google Scholar]
- 15.Edelman D, Olsen MK, Dudley TK, Harris AC, Oddone EZ. Utility of hemoglobin A1c in predicting diabetes risk. J Gen Intern Med. 2004;19:1175–1180. doi: 10.1111/j.1525-1497.2004.40178.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cheng P, Neugaard B, Foulis P, Conlin PR. Hemoglobin A1c as a predictor of incident diabetes. Diabetes Care. 2011;34:610–615. doi: 10.2337/dc10-0625. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Abdul-Ghani MA, Abdul-Ghani T, Muller G, et al. Role of glycated hemoglobin in the prediction of future risk of T2DM. J Clin Endocrinol Metab. 2011;96:2596–2600. doi: 10.1210/jc.2010-1698. [DOI] [PubMed] [Google Scholar]
- 18.Selvin E, Steffes MW, Gregg E, Brancati FL, Coresh J. Performance of A1c for the classification and prediction of diabetes. Diabetes Care. 2011;34:84–89. doi: 10.2337/dc10-1235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Saks DB, John WG. Interpretation of hemoglobin A1c values. JAMA. 2014;311:2271–2272. doi: 10.1001/jama.2014.6342. [DOI] [PubMed] [Google Scholar]
- 20.Gosmanov AR, Wan J. Low positive predictive value of hemoglobin A1c for diagnosis of prediabetes in clinical practice. Am J Med Sci. 2014;348:191–194. doi: 10.1097/MAJ.0000000000000223. [DOI] [PubMed] [Google Scholar]
- 21.Lipska KJ, De Rekeneire N, Van Ness PH, et al. Identifying dysglycemic states in older adults: implications of the emerging use of hemoglobin A1c. J Clin Endocrinol Metab. 2010;95:5289–5295. doi: 10.1210/jc.2010-1171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cowie CC, Rust KF, Byrd-Holt DD, et al. Prevalence of diabetes and high risk for diabetes using A1c criteria in the US population in 1988–2006. Diabetes Care. 2010;33:562–568. doi: 10.2337/dc09-1524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Guo F, Moellering DR, Garvey WT. Use of HbA1c for diagnoses of diabetes and prediabetes: comparison with diagnoses based on fasting and 2-hr glucose values and effects of gender, race, and age. Metab Syndr Relat Disord. 2014;12:258–268. doi: 10.1089/met.2013.0128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bersoux S, Cook CB, Wu Q, et al. Hemoglobin A1c testing alone does not sufficiently identify patients with prediabetes. Am J Clin Pathol. 2011;135:674–677. doi: 10.1309/AJCPJBG0WYRAHN0R. [DOI] [PubMed] [Google Scholar]
- 25.Fajans SS, Herman WH, Oral EA. Insufficient sensitivity of hemoglobin A1c determination in diagnosis or screening of early diabetic states. Metabolism. 2011;60:86–91. doi: 10.1016/j.metabol.2010.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Davidson MB, Schriger DL, Peters AL, Lorber B. Revisiting the oral glucose tolerance test criterion for the diagnosis of diabetes. J Gen Intern Med. 2000;15:551–555. doi: 10.1046/j.1525-1497.2000.08024.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Wang W, Lee ET, Howard BV, Fabsitz RR, Devereux RB, Welty TK. Fasting plasma glucose and hemoglobin A1c in identifying and predicting diabetes: The Strong Heart Study. Diabetes Care. 2011;34:363–368. doi: 10.2337/dc10-1680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Schwartz KL, Monsur JC, Bartoces MG, West PA, Neale AV. Correlation of same-visit A1c test with laboratory-based measurements: a MetroNet study. BMC Fam Pract. 2005;6:28. doi: 10.1186/1471-2296-6-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Getaneh A, Andres R, Brillon DJ, Findley SE. Hemoglobin A1c criterion for diabetes diagnosis among Hispanic and non-Hispanic populations. Endocr Pract. 2011;17:210–217. doi: 10.4158/EP10119.OR. [DOI] [PubMed] [Google Scholar]
- 30.Vable AM, Drum ML, Tang H, Chin MH, Lindau ST, Huang ES. Implications of the new definition of diabetes for health disparities. J Natl Med Assoc. 2011;103:219–223. doi: 10.1016/s0027-9684(15)30299-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Tsugawa Y, Mukamal KJ, Davis RB, Taylor WC, Wee CC. Should the hemoglobin A1c diagnostic cutoff differ between blacks and whites? A cross-sectional study. Ann Intern Med. 2012;157:153–159. doi: 10.7326/0003-4819-157-3-201208070-00004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Buse JB, Kaufman FR, Linder B, et al. Diabetes screening with hemoglobin A1c versus fasting plasma glucose in a multiethnic middle-school cohort. Diabetes Care. 2013;36:429–435. doi: 10.2337/dc12-0295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Olson DE, Rhee MK, Herrick K, Ziemer DC, Twombly JG, Phillips LS. Screening for diabetes and pre-diabetes with proposed A1c-based diagnostic criteria. Diabetes Care. 2010;33:2184–2189. doi: 10.2337/dc10-0433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Araneta MR, Grandinetti A, Chang HK. A1c and diabetes diagnosis among Filipino Americans, Japanese Americans, and Native Hawaiians. Diabetes Care. 2010;33:2626–2628. doi: 10.2337/dc10-0958. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Malkani S, DeSilva T. Controversies on how diabetes is diagnosed. Curr Opin Endocrinol Diabetes Obes. 2012;19:97–103. doi: 10.1097/MED.0b013e32835168c0. [DOI] [PubMed] [Google Scholar]
- 36.Clayton W, Jr, Agarwal N, Wang L, Jagasia S. Clinical markers implying the need for treatment in women with gestational diabetes mellitus. Endocr Pract. 2012;18:62–65. doi: 10.4158/EP11143.OR. [DOI] [PubMed] [Google Scholar]
- 37.Cakan N, Kizilbash S, Kamat D. Changing spectrum of diabetes mellitus in children: challenges with initial classification. Clin Pediatr (Phila) 2012;51:939–944. doi: 10.1177/0009922812441666. [DOI] [PubMed] [Google Scholar]
- 38.Vehik K, Cuthbertson D, Boulware D, et al. Performance of HbA1c as an early diagnostic indicator of type 1 diabetes in children and youth. Diabetes Care. 2012;35:1821–1825. doi: 10.2337/dc12-0111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Sharma S, Fleming SE. Use of HbA1c testing to diagnose pre-diabetes in high risk African American children: a comparison with fasting glucose and HOMA-IR. Diabetes Metab Syndr. 2012;6:157–162. doi: 10.1016/j.dsx.2012.09.004. [DOI] [PubMed] [Google Scholar]
- 40.Nowicka P, Santoro N, Liu H, et al. Utility of hemoglobin A1c for diagnosing prediabetes and diabetes in obese children and adolescents. Diabetes Care. 2011;34:1306–1311. doi: 10.2337/dc10-1984. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Shah S, Kublaoui BM, Oden JD, White PC. Screening for type 2 diabetes in obese youth. Pediatrics. 2009;124:573–579. doi: 10.1542/peds.2008-2949. [DOI] [PubMed] [Google Scholar]
- 42.Pradhan AD, Rifai N, Buring JE, Ridker PM. Hemoglobin A1c predicts diabetes but not cardiovascular disease in nondiabetic women. Am J Med. 2007;120:720–727. doi: 10.1016/j.amjmed.2007.03.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Ford ES, Cowie CC, Li C, Handelsman Y, Bloomgarden ZT. Iron-deficiency anemia, non-iron-deficiency anemia and HbA1c among adults in the US. J Diabetes. 2011;3:67–73. doi: 10.1111/j.1753-0407.2010.00100.x. [DOI] [PubMed] [Google Scholar]
- 44.Tien PC, Schneider MF, Cox C, et al. Association of HIV infection with incident diabetes mellitus: Impact of using hemoglobin A1c as a criterion for diabetes. J Acquir Immune Defic Syndr. 2012;61:334–340. doi: 10.1097/QAI.0b013e31826bfc32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Eckhardt BJ, Holzman RS, Kwan CK, Baghdadi J, Aberg JA. Glycated hemoglobin A1c as screening for diabetes mellitus in HIV-infected individuals. AIDS Patient Care STDS. 2012;26:197–201. doi: 10.1089/apc.2011.0379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.American Association of Clinical Endocrinologists Board of Directors. American College of Endocrinologists Board of Trustees American Association of Clinical Endocrinologists/American College of Endocrinology statement on the use of hemoglobin A1c for the diagnosis of diabetes. Endocr Pract. 2010;16:155–156. doi: 10.4158/EP.16.2.155. [DOI] [PubMed] [Google Scholar]
- 47.The Endocrine Society The Endocrine Society statement on the use of A1c for diabetes diagnosis and risk estimation. [Accessed September 4, 2014]. Available from: http://www.endocrinologia.org.mx/descargas/guias_endos/The%20Endocrine%20Society%20Statement%20on%20A1c%20use.pdf.
- 48.World Health Organization . Abbreviated report of a WHO consultation. Geneva, Switzerland: World Health Organization; 2011. [Accessed October 1, 2013]. Use of glycated haemoglobin (HbA1c) in the diagnosis of diabetes mellitus. Available from: http://www.who.int/diabetes/publications/report-hba1c_2011.pdf. [PubMed] [Google Scholar]
- 49.Wu EL, Kazzi NG, Lee JM. Cost-effectiveness of screening strategies for identifying pediatric diabetes mellitus and dysglycemia. JAMA Pediatr. 2013;167:32–39. doi: 10.1001/jamapediatrics.2013.419. [DOI] [PMC free article] [PubMed] [Google Scholar]