

Abstract
Background Open reduction and internal fixation (ORIF) using a volar locking plate is a common method for treating displaced distal radius fractures. There is, however, the risk of extensor tendon rupture due to protrusion of the screw tips past the dorsal cortex, which cannot always be adequately seen on a lateral fluoroscopic view. We therefore wished to compare the sensitivity of an intraoperative fluoroscopic skyline view to a lateral fluorosocopic view in detecting past pointing of these screws.
Material and Methods Our series included 75 patients with an average age of 59 years who underwent volar locked plate fixation of a displaced distal radius fracture. Intraoperative anteroposterior (AP), lateral, and skyline fluoroscopic views were performed in each case. The number of screws that were seen to protrude past the dorsal cortex of the distal fracture fragment were recorded for both the lateral and skyline views. The number of screws that required exchange was also documented.
Results No screws were seen to protrude past the dorsal cortical bone on the lateral fluroscopic views. 15 of 300 screws (5%) were seen to protrude past the dorsal cortex by an average of 0.8 mm (range, 0.5 to 2 mm) and were exchanged for shorter screws in 11/75 patients.
Conclusion Our results demonstrate that the skyline is more sensitive than a lateral fluoroscopic view at demonstrating protrusion of the screws in the distal fracture fragment following volar locked plate fixation.
Level of Evidence IV
Keywords: distal radius, screw, skyline, tendon rupture, volar plate
Open reduction and internal fixation (ORIF) through a volar approach has become the “gold standard” in terms of surgical treatment of fractures of the distal radius.1 This technique can, however, be responsible for complications such as tendon rupture that are caused by screws passing through the dorsal cortex of the distal radius.2 3 4 A tangential X-ray view of the dorsal distal radius, or “skyline” view, has been described to detect the screws that are too long.5 The accuracy of this view has been validated by experimental studies.6 7 8 There are two published clinical series on the use of this view.9 10
The purpose of this article is to demonstrate the utility of the skyline fluoroscopic view in detecting screws that penetrate the dorsal cortex of the distal radius that are not apparent on AP and lateral fluoroscopic views.
Materials and Methods
We performed a retrospective chart review of all patients with a distal radius fracture who were treated with open reduction and volar locking plate fixation between November 2013 and April 2014. The series included 75 patients with a mean age of 59 years (19–93), including 59 women. Thirty-nine fractures involved the left wrist.
All patients underwent plate fixation using the same technique through the volar Henry approach, by five different surgeons, under locoregional anesthesia, using a tourniquet and the Henry approach with a volar locked plate (One Step, newClip Technics, The Fourrassière, France). A fluoroscope (XiScan4400, FMCONTROL, Alava, Spain) was covered with a sterile drape and placed on top of the arm table to perform intraoperative anteroposterior (AP), lateral, and skyline fluoroscopic views. The latter was obtained in two steps. The first step was to place the elbow in a 75° flexed position with the forearm in full supination and the wrist held in maximal flexion (Fig. 1). From this position, the second step was to change the position of the elbow a few degrees in flexion or extension, until an optimal position was obtained that enabled visualization of four anatomical landmarks: the radial styloid, the dorsal cortical bone of the radius in its entire width, Lister's tubercle, and the distal radioulnar joint (DRUJ) space. Screws crossing the dorsal cortical bone were changed, and new fluoroscopic views were taken.
Fig. 1.

Installation to achieve intraoperative fluoroscopic “skyline.”
Any changes in screw length or trajectory were made after reviewing all three fluoroscopic views. All such changes were recorded (Figs. 2 and 3).
Fig. 2.
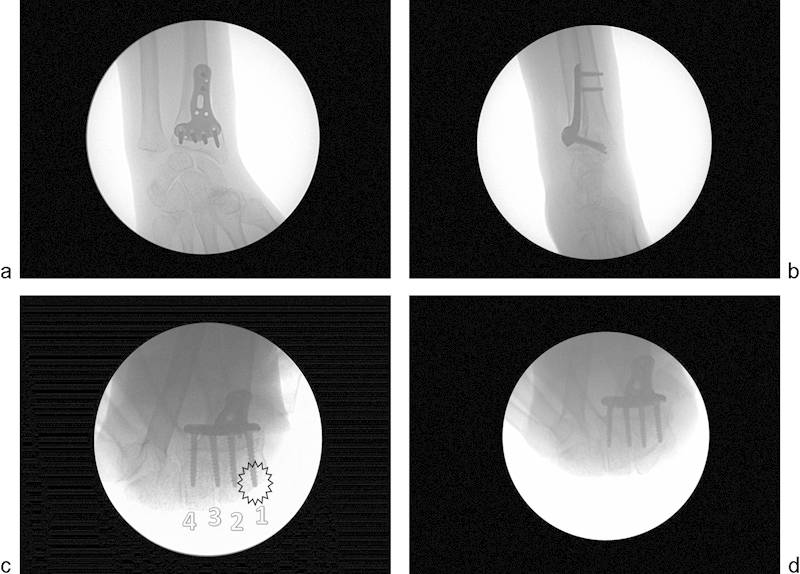
Intraoperative fluoroscopic control of a osteosynthesis of distal radius fracture by a volar plate (case No. 17). (a) AP view. The most distal ulnar screw does not cross the DRUJ. (b) Lateral view. No screws appear to cross the dorsal cortical bone of the distal radius. (c) Skyline view. The most distal radial screw crosses the dorsal cortical bone of the distal radius. (Screw 1: the most radial screw; Screw 2: the screw radial to Lister tubercle; Screw 3: the screw ulnar to Lister tubercle; Screw 4: the most ulnar screw). (d) Skyline view. After change of screws, the most distal radial screw does not cross the dorsal cortical bone of the the distal radius.
Fig. 3.
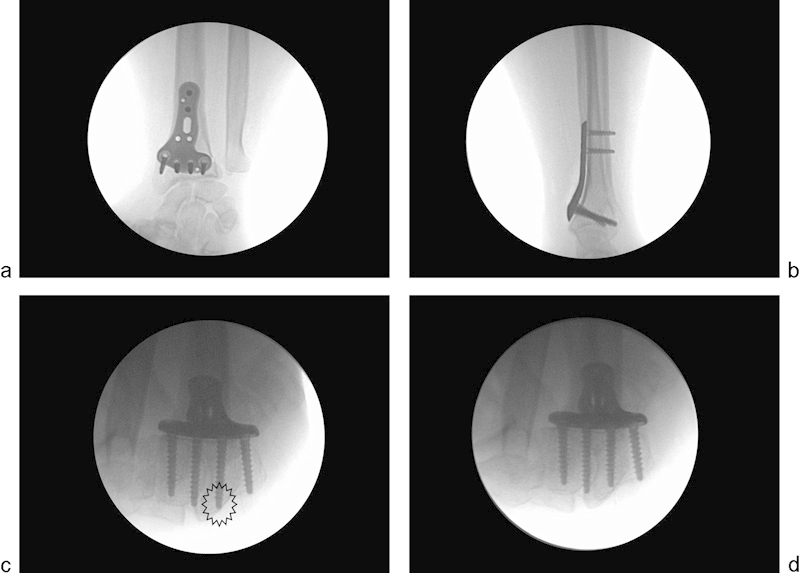
Intraoperative fluoroscopic control of a osteosynthesis of distal radius fracture by a volar plate (case No. 59). (a) AP view. The most distal ulnar screw does not cross the DRUJ. (b) Lateral view. No screws appear to cross the dorsal cortical bone of the distal radius. (c) Skyline view. The second distal radial screw crosses the dorsal cortical bone of the distal radius. (d) Skyline view. After change of screws, the second distal radial screw does not cross the dorsal cortical bone of the distal radius.
Results
No screws seemed to cross the dorsal cortical bone on the lateral views. Fifteen of 300, or 5%, of the screws that were inserted in the distal plate, however, were seen to penetrate through the dorsal cortex of the distal fragment on the skyline view and were exchanged for a shorter screw intraoperatively. The amount of screw protusion averaged 0.8 mm, with a range of 0.5 to 2 mm. The use of a skyline view changed the intraoperative management in 11 of 75 patients (14.66%) (Table 1).
Table 1. Number of screws crossing the dorsal cortex changed during osteosynthesis of distal radius fracture with volar plate after reading the intraoperative fluoroscopic projection/incidence on a series of 75 clinical cases.
| Case | Screw protrusion length (mm) | |||
|---|---|---|---|---|
| (N) | Screw 1 | Screw 2 | Screw 3 | Screw 4 |
| 10 | 1 | |||
| 14 | 2 | |||
| 17 | 0.5 | |||
| 25 | 0.5 | |||
| 27 | 2 | |||
| 39 | 0.5 | 0.5 | ||
| 48 | 0.5 | |||
| 57 | 1 | 1 | ||
| 59 | 1 | |||
| 72 | 0.5 | |||
| 73 | 1 | |||
| 75 | 0.5 | 0.5 | ||
Screw 1: the most radial screw.
Screw 2: the screw radial to the Lister tubercle.
Screw 3: the screw ulnar to the Lister tubercle.
Screw 4: the most ulnar screw.
Discussion
The most frequent complications after internal fixation performed through a volar approach of distal radius fractures are tendinitis and ruptures of the flexor and extensor tendons of the fingers at the wrist level.3 11 12 13 14
Intraoperatively and from the lateral radiographs, it is difficult to identify screws protruding from the dorsal cortical bone because the individual and combined height of the Lister tubercle and the depth of the groove for the extensor pollicus longus can vary between 4 and 10 mm, which makes it difficult to detect the presence and amount of protrusion of the distal screws.15 In a cadaver study on the ability of examiners to assess whether screws placed from volar to dorsal during distal radius plating had penetrated the dorsal cortex of the radius by more than 2 mm, using standard fluoroscopic imaging, evaluators with >3 years in practice were able to detect incorrect screw positions with 100% sensitivity in the most radial position, 90% in the central position, and 75% in the ulnar position. Inexperienced evaluators detected incorrect screw positioning with 70% sensitivity in the radial position, 61% centrally, and 56% ulnarly.16 To resolve this problem, several authors have tried to develop new, more sensitive radiological views or new imaging techniques. It is not possible to rely on a simple subtraction of the height of the Lister tubercle because of its anatomical variations on a lateral X-ray view. From a computed tomography (CT) study, some authors have shown that the height of the Lister tubercle ranges between 3.3 and 6.6 mm.17 Radiographs in pronation and supination better detect screws protruding the dorsal cortical bone than the standard lateral radiographs do, but unfortunately, those are difficult to standardize.18
Jacob proposed the skyline view to visualize the dorsal cortex of the distal radius.5 It is the opposite view to that of the carpal tunnel, which highlights the volar aspect of the distal radius.19 20 The carpal tunnel view is performed with the wrist in pronation and extension. The skyline radiographic view was described in supination and flexion of the wrist. It is also referred to as the dorsal horizon view9 or the dorsal tangential view of the wrist.10 Two skyline techniques have been described for the wrist: one with the forearm supinated and fluoroscope positioned vertically and aimed along the longitudinal axis of the forearm,5 6 the other with the forearm pronated and fluoroscope positioned horizontally.9 10 Regardless of the technique, the amount of elbow flexion and extension should be adjusted incrementally to avoid overlapping of the dorsal cortical bone of the radius with the dorsal edge of the carpal bones.7
The skyline view is the most sensitive X-ray view to detect protrusion of screws that are inserted through a volar locking plate past the dorsal cortical bone of the distal radius. In a study using a sawbones model, the sensitivity of the skyline view was 83% in detecting a screw crossing the dorsal cortical bone by up to 1 mm, while the sensitivity using an oblique pronation projection view was 77% and using a profile view 51%.6 Two clinical studies using the skyline view showed a change in screw length in 4 of 15 patients9 and 11 of 27 patients.10 In our study the screw length was changed in 11 of 75 patients. Even if the best X-ray view is the skyline, it does not have a sensitivity of 100%. In a clinical study of intraoperative CT fluoroscopy, the screws were changed in 31.3% of cases.22
The additional time associated with this technique was 6.7 minutes, and the irradiation was 19.3cGy/cm2. The dose of ionizing radiation needed to achieve an intraoperative skyline fluoroscopic view is on average 0.93 cGy/cm2 and is negligible compared with that of a conventional wrist radiography.8
In one study of 9 patients, ultrasound appeared to be useful for detecting dorsal screw protrusion, but no sensitivity analysis was performed.
Limitations of our study include the lack of direct visual inspection or sonographic or CT confirmation of the screw protrusion. There was no intra- or interobserver calculation, because the screws were changed intraoperatively based on the opinion of the operating surgeon.
Aknowledgment
Mickaël Schaeffer, Département d'Informatique Médicale, Strasbourg University Hospitals, Strasbourg, France
Footnotes
Conflict of Interest Philippe Liverneaux has a conflict of interest with Newclip Technics, Integra, Argomedical, iiN medical.
References
- 1.Downing N D, Karantana A. A revolution in the management of fractures of the distal radius? J Bone Joint Surg Br. 2008;90(10):1271–1275. doi: 10.1302/0301-620X.90B10.21293. [DOI] [PubMed] [Google Scholar]
- 2.Al-Rashid M, Theivendran K, Craigen M A. Delayed ruptures of the extensor tendon secondary to the use of volar locking compression plates for distal radial fractures. J Bone Joint Surg Br. 2006;88(12):1610–1612. doi: 10.1302/0301-620X.88B12.17696. [DOI] [PubMed] [Google Scholar]
- 3.Arora R, Lutz M, Hennerbichler A, Krappinger D, Espen D, Gabl M. Complications following internal fixation of unstable distal radius fracture with a palmar locking-plate. J Orthop Trauma. 2007;21(5):316–322. doi: 10.1097/BOT.0b013e318059b993. [DOI] [PubMed] [Google Scholar]
- 4.Benson E C, DeCarvalho A, Mikola E A, Veitch J M, Moneim M S. Two potential causes of EPL rupture after distal radius volar plate fixation. Clin Orthop Relat Res. 2006;451(451):218–222. doi: 10.1097/01.blo.0000223998.02765.0d. [DOI] [PubMed] [Google Scholar]
- 5.Clay J J. Re: Pichler et al. Computer tomography aided 3D analysis of the distal dorsal radius surface and the effects on volar plate osteosynthesis. J Hand Surg Eur. 2009, 34: 598–602. J Hand Surg Eur. 2010;35:335–336. doi: 10.1177/1753193409101471. [DOI] [PubMed] [Google Scholar]
- 6.Riddick A P, Hickey B, White S P. Accuracy of the skyline view for detecting dorsal cortical penetration during volar distal radius fixation. J Hand Surg Eur Vol. 2012;37(5):407–411. doi: 10.1177/1753193411426809. [DOI] [PubMed] [Google Scholar]
- 7.Haug L C, Glodny B, Deml C, Lutz M, Attal R. A new radiological method to detect dorsally penetrating screws when using volar locking plates in distal radial fractures. The dorsal horizon view. Bone Joint J. 2013;95-B(8):1101–1105. doi: 10.1302/0301-620X.95B8.31301. [DOI] [PubMed] [Google Scholar]
- 8.Vaiss L Ichihara S Ramirez D G Hendriks S Liverneaux P Facca S A comparative study about ionizing radiation emitted during radiological “skyline” view of the wrist in pronation versus supination Eur J Orthop Surg Traumatol 2014; [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 9.Joseph S J, Harvey J N. The dorsal horizon view: detecting screw protrusion at the distal radius. J Hand Surg Am. 2011;36(10):1691–1693. doi: 10.1016/j.jhsa.2011.07.020. [DOI] [PubMed] [Google Scholar]
- 10.Ozer K, Toker S. Dorsal tangential view of the wrist to detect screw penetration to the dorsal cortex of the distal radius after volar fixed-angle plating. Hand (NY) 2011;6(2):190–193. doi: 10.1007/s11552-010-9316-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.McKay S D, MacDermid J C, Roth J H, Richards R S. Assessment of complications of distal radius fractures and development of a complication checklist. J Hand Surg Am. 2001;26(5):916–922. doi: 10.1053/jhsu.2001.26662. [DOI] [PubMed] [Google Scholar]
- 12.Rozental T D, Blazar P E. Functional outcome and complications after volar plating for dorsally displaced, unstable fractures of the distal radius. J Hand Surg Am. 2006;31(3):359–365. doi: 10.1016/j.jhsa.2005.10.010. [DOI] [PubMed] [Google Scholar]
- 13.Kambouroglou G K, Axelrod T S. Complications of the AO/ASIF titanium distal radius plate system (pi plate) in internal fixation of the distal radius: a brief report. J Hand Surg Am. 1998;23(4):737–741. doi: 10.1016/S0363-5023(98)80063-4. [DOI] [PubMed] [Google Scholar]
- 14.Orbay J L, Fernandez D L. Volar fixation for dorsally displaced fractures of the distal radius: a preliminary report. J Hand Surg Am. 2002;27(2):205–215. doi: 10.1053/jhsu.2002.32081. [DOI] [PubMed] [Google Scholar]
- 15.Clement H, Pichler W, Nelson D, Hausleitner L, Tesch N P, Grechenig W. Morphometric analysis of Lister's tubercle and its consequences on volar plate fixation of distal radius fractures. J Hand Surg Am. 2008;33(10):1716–1719. doi: 10.1016/j.jhsa.2008.08.012. [DOI] [PubMed] [Google Scholar]
- 16.Thomas A D, Greenberg J A. Use of fluoroscopy in determining screw overshoot in the dorsal distal radius: a cadaveric study. J Hand Surg Am. 2009;34(2):258–261. doi: 10.1016/j.jhsa.2008.10.002. [DOI] [PubMed] [Google Scholar]
- 17.Pichler W, Windisch G, Schaffler G, Rienmüller R, Grechenig W. Computer tomography aided 3D analysis of the distal dorsal radius surface and the effects on volar plate osteosynthesis. J Hand Surg Eur Vol. 2009;34(5):598–602. doi: 10.1177/1753193409101471. [DOI] [PubMed] [Google Scholar]
- 18.Maschke S D, Evans P J, Schub D, Drake R, Lawton J N. Radiographic evaluation of dorsal screw penetration after volar fixed-angle plating of the distal radius: a cadaveric study. Hand (NY) 2007;2(3):144–150. doi: 10.1007/s11552-007-9038-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wilson J N. Profiles of the carpal canal. J Bone Joint Surg Am. 1954;36-A(1):127–132. [PubMed] [Google Scholar]
- 20.Carroll R E, Lakin J F. Fracture of the hook of the hamate: radiographic visualization. Iowa Orthop J. 1993;13:178–182. [PMC free article] [PubMed] [Google Scholar]