

Abstract
Real-time strain elastography is not routinely performed in clinical practice for characterizing gastrointestinal tract diseases, and there are few studies in the literature on the subject. The recent EFSUMB guidelines suggest the use of this method in the diagnosis of neoplastic lesions and in the characterization of bowel strictures in patients with Crohn’s disease. The purpose of this pictorial essay is to evaluate the feasibility of strain elastography in some pathologies of the colon frequently encountered in daily clinical practice and to compare elastography images with corresponding endoscopic and radiographic images. In our opinion, strain elastography is useful for characterizing diseases of the colon as it can add valuable diagnostic information to grayscale ultrasound imaging. However, diagnostic accuracy and clinical relevance of this information should be confirmed by further prospective research-targeted studies.
Keywords: Colon, Ultrasonography, Real time elastography, Gastrointestinal elastography
Sommario
L’ elastografia strain non viene attualmente utilizzata nella pratica clinica per la caratterizzazione delle patologie del tubo digerente ed anche in Letteratura gli studi sull’argomento sono pochi. Le recenti Linee Guida EFSUMB suggeriscono la metodica per la diagnosi delle neoplasie del tubo gastroenterico e per la caratterizzazione dei tratti intestinali stenotici nel morbo di Crohn. Lo scopo di questo Pictorial Esssay è di valutare la “feasibility” dell’ elastografia in alcune comuni patologie del colon e confrontare le immagini elastografiche con le corrispondenti endoscopiche o radiologiche. E’ nostra opinione che la elastografia “strain” sia utile per la caratterizzazione delle patologie del colon in quanto fornisce informazioni aggiuntive all’ ecografia in scala dei grigi. Peraltro l’accuratezza diagnostica e la rilevanza clinica della metodica devono essere ancora confermate con studi prospettici mirati.
Introduction
Ultrasound (US) imaging is the first-line investigation in patients with abdominal symptoms, as this method also provides a satisfactory depiction of the gastrointestinal tract thereby allowing diagnosis of neoplastic or inflammatory disorders.
One of the more recent US techniques, strain elastography, has aroused a great deal of interest as it provides a real-time qualitative measurement of the elasticity of the lesions compared to the surrounding reference tissue. The recently published EFSUMB guidelines recommend the use of strain elastography in the field of gastroenterology for the characterization of focal lesions of the gastrointestinal tract and differentiation between inflammatory and fibrotic strictures in patients with Crohn’s disease (2013 [1]).
The aim of this study was to evaluate the feasibility of strain elastography in certain disorders of the colon and compare the images with corresponding endoscopic or radiological images.
With regard to the physical principles underlying the method and how to carry out the examination, please see the recent EFSUMB guidelines [2].
Strain elastography shows the elasticity/stiffness of the intestinal wall in a color scale ranging from blue to red (blue indicates maximum stiffness, green intermediate stiffness and red maximum elasticity). The evaluation is qualitative and subjective unless special software is used to calculate the stiffness ratio between the lesion and the surrounding reference tissue.
In order to obtain a better reproducibility and comparability of the observations, the outcome of strain elastography is classified according to a colorimetric classification method already proposed in the literature [3, 4]. Havre and colleagues noted a fair interobserver agreement, when this three-level visual categorical classification was applied to evaluate elastographic video files in their study [4].
The lesions are categorized according to the distribution of colors appearing on the images: category 1 = the intestinal wall appears homogeneous in a predominant color (blue = A, green = B, red = R); category 2 = inhomogeneous appearance in 2–3–4 colors in various patterns, but not fragmented; category 3 = inhomogeneous appearance in a “honeycomb” pattern due to fragmentation of the color (in our experience, this pattern rarely appears in diseases affecting the colon).
Normal bowel wall thickness is <3 mm and the strain elastography color map will show predominantly green; it is therefore classified 1B (Fig. 1 a). In the presence of bowel disease, the bowel wall is usually thickened, and strain elastography color map will show various shades, mainly blue and turquoise if the bowel wall is stiffer than normal, whereas the color map will show various shades from yellow to red if the bowel wall is more elastic than normal (Fig. 1b–d).
Fig. 1.

a Normal bowel wall classified 1B (predominantly green, arrowhead). b Diseased bowel wall (Crohn’s disease) classified 1A (predominantly blue). c Diseased bowel wall (ulcerative colitis) classified 2BA (mixed green and blue with a slight predominance of green). d Diseased bowel wall (sigmoid colon cancer) classified 2BAR (mixed color pattern with a predominance of green)
Grayscale US imaging of the colon and strain elastography were performed with Mylab Alpha (Esaote Biomedica Genoa, Italy) and a linear probe (SL 1543, 13–4 MHz) after overnight fast; the US operator (AG) has 15 years experience in bowel US.
Strain elastography of malignant and benign tumors of the colon
Increased stiffness of a focal lesion is caused by a desmoplastic stromal response and is suggestive of malignancy.
There are few data in the literature regarding strain elastography of neoplastic lesions of the gastrointestinal tract. Havre et al. [4] examined adequately prepared surgical specimens from 27 patients (18 sections of adenocarcinomas, 4 sections of adenomas and 16 sections of stenotic lesions from patients with Crohn’s disease) and found that adenocarcinomas and stenotic lesions from patients with Crohn’s disease were stiffer than adenomas and the surrounding intestinal wall. Adenocarcinomas appeared mainly in shades of blue and green (11 cases: blue > green, 6 cases: green > blue), whereas adenomas were mainly shown as homogeneously green or in an inhomogeneous color pattern of green and blue (green > blue).
Waage et al. [5] studied rectal lesions using strain elastography and an endorectal probe. They reported a diagnostic accuracy of 94 % in differentiating adenomas of the rectum (n = 23) from carcinomas (n = 45).
We present strain elastography images of five different neoplastic malignancies (Figs. 2, 3), two benign polypoid lesions (Fig. 4) and one lipoma of the colon (Fig. 5) with the corresponding endoscopic or radiological images.
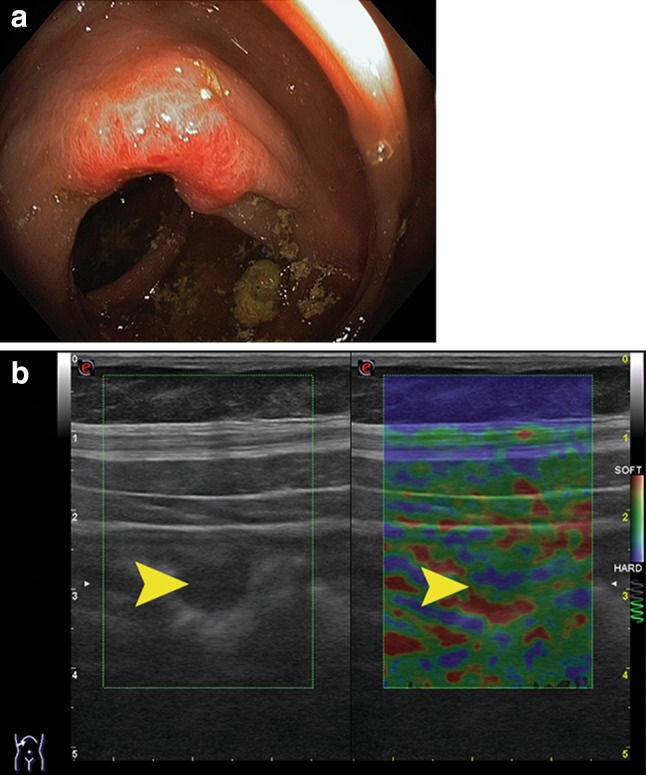
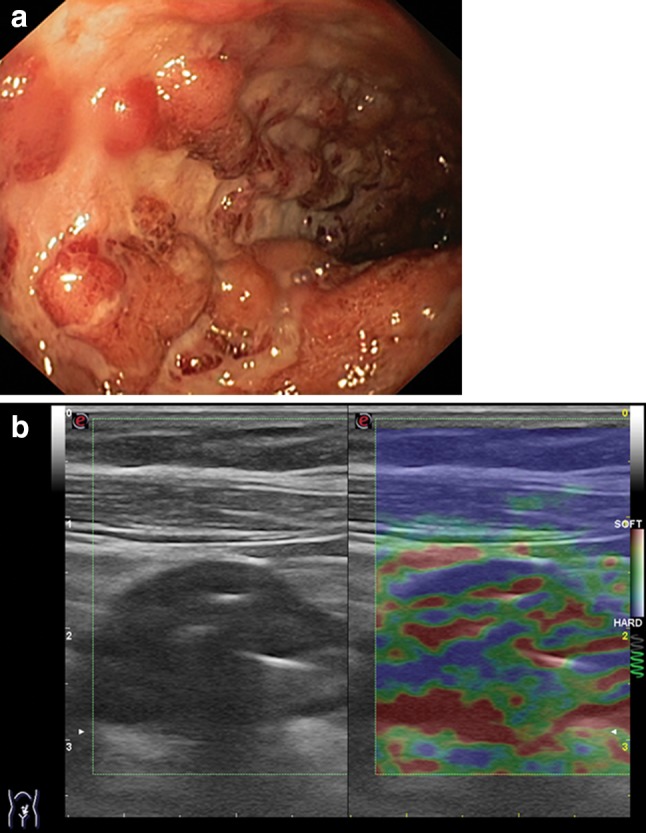
Fig. 2.

a Endoscopy shows stenosing neoplasm of the sigmoid colon; diagnosis was histologically confirmed. b Strain elastography shows increased stiffness of the lesion classified 1A (homogeneously stiff, arrowhead). a1 Endoscopy reveals a vegetating neoplastic lesion of the ascending colon; diagnosis was histologically confirmed. b1 Strain elastography shows increased stiffness of the lesion classified 1A (homogeneously stiff, arrowhead); imaging of the deep lying structures is inadequate due to loss of signal strength. a2 Contrast-enhanced CT shows synchronous cancer of the sigmoid colon: a vegetating mass (arrow) and a stenosing lesion (arrowhead); diagnosis was histologically confirmed. b2 Strain elastography shows the vegetating mass characterized by an array of colors classified 2BRA (green > red > blue, arrowhead). c2 Strain elastography shows neoplasm with increased wall stiffness classified 2AB (blue > green, arrowhead)
Fig. 3.
a Endoscopy shows neoplasm arising in a fold of the transverse colon, histologically confirmed. b Strain elastography shows a small tumor classified 2BA (green > blue arrowhead); in this early stage a neoplastic lesion is difficult to differentiate from the surrounding tissue at strain elastography
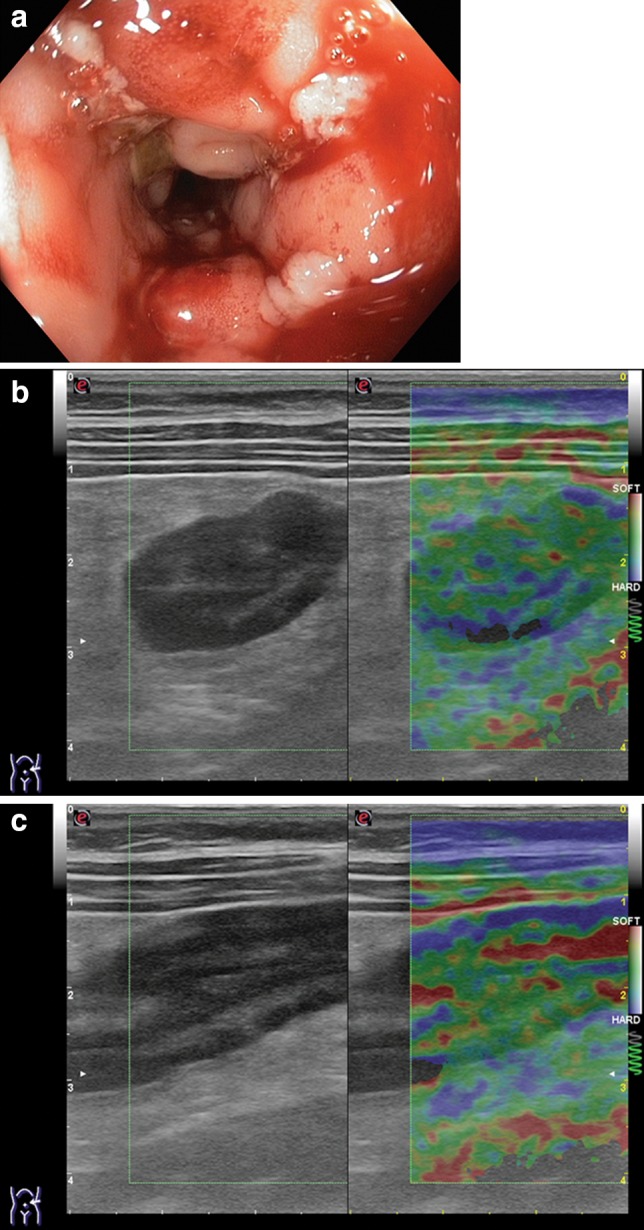
Fig. 4.

a Endoscopy reveals a sessile polyp of the distal ascending colon classified 01 s (Paris Classification [6]); histological outcome was tubulovillous adenoma with severe dysplasia. b Strain elastography shows the polyp, which appears inhomogeneous, classified 2BAR (mix of colors, green > blue > red). a1 Endoscopy shows a polyp of the descending colon (granular laterally spreading tumor); histological outcome was tubulovillous adenoma with mild dysplasia. b1 Strain elastography shows the polyp, which appears relatively homogeneous, classified 2BR (green > red)
Fig. 5.
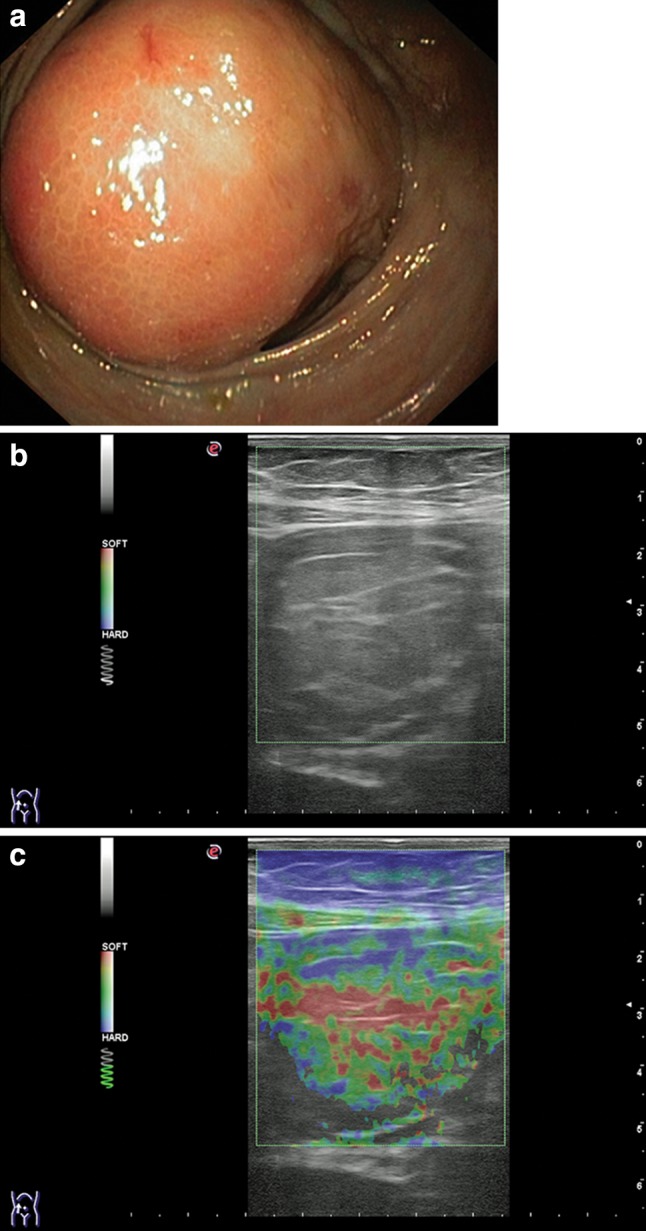
a Endoscopy reveals lipoma of the ascending colon. b Grayscale US shows the lipoma with thin hyperechoic septa. c Strain elastography shows the lipoma, which appears relatively homogeneous classified 2BR (green > red)
Strain elastography of the colonic wall: ulcerative colitis
The literature contains few data on the use of strain elastography in ulcerative colitis.
Ishikawa and colleagues published a paper [7] in which they compared the outcome of strain elastography and endoscopy performed in 37 patients with ulcerative colitis; they found that the two methods correlated in the classification of colonic disease activity. The authors described four strain elastography patterns: “normal” (thin walls and green color pattern) and “homogeneous” (thickened walls and green color pattern) correlated with normal or slightly abnormal endoscopic images (mucosal edema or erosions), whereas “random pattern” (thickened walls and a mosaic of colors) correlated with endoscopic images of moderate-severe colitis (punctate or deep ulcers). Finally, the “hard elastography pattern” correlated with endoscopic images showing fulminant ulcerative colitis (extensive ulceration and wide mucosal defects) or mucosal atrophy in case of inactive disease.
We present images of three cases: the first is a mild form of ulcerative sigmoiditis treated with mesalazine (Fig. 6), the second case is in clinical remission after infliximab therapy (Fig. 7), and the third case shows lack of clinical response to infliximab therapy (Fig. 8).
Fig. 6.
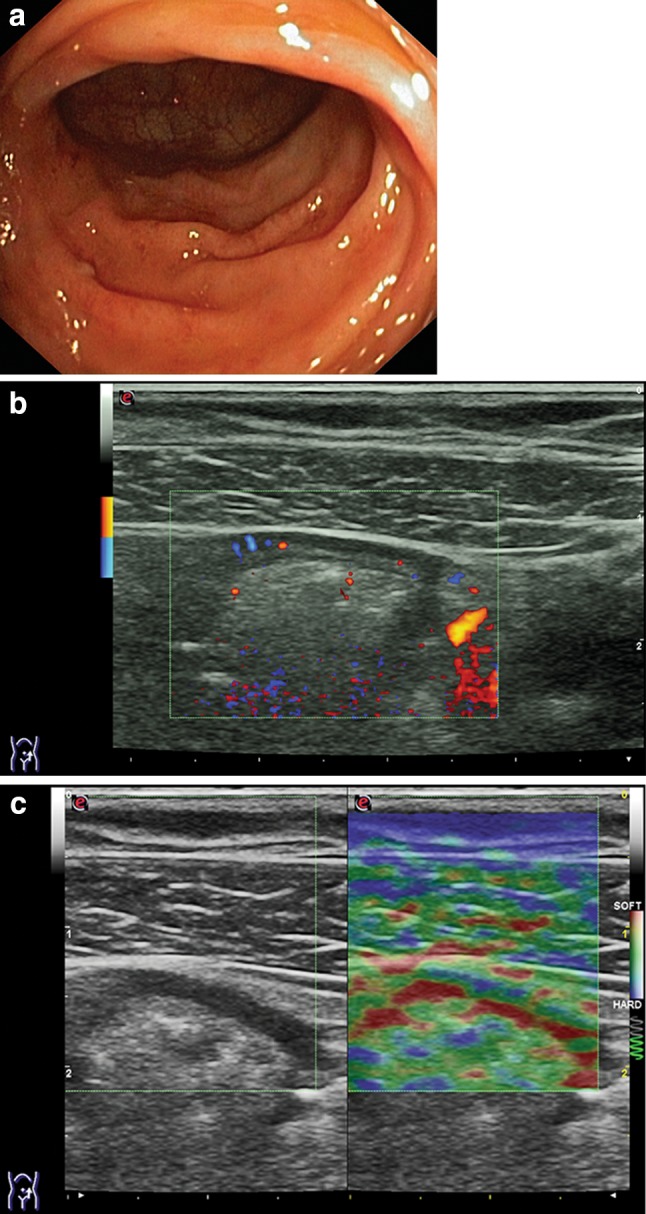
a Endoscopy shows sigmoid colon edema and mild hyperemia (Mayo endoscopic score 1); upstream the sigmoid colon presents with a regular mucosal vascular pattern. b Color Doppler image of the sigmoid colon shows wall thickness 2.4 mm, preserved echotexture, and blood flow signals in the colonic wall. c Strain elastography image of the same portion of the sigmoid colon with persistent abnormal elastographic appearance, classified 2BR (green > red)
Fig. 7.
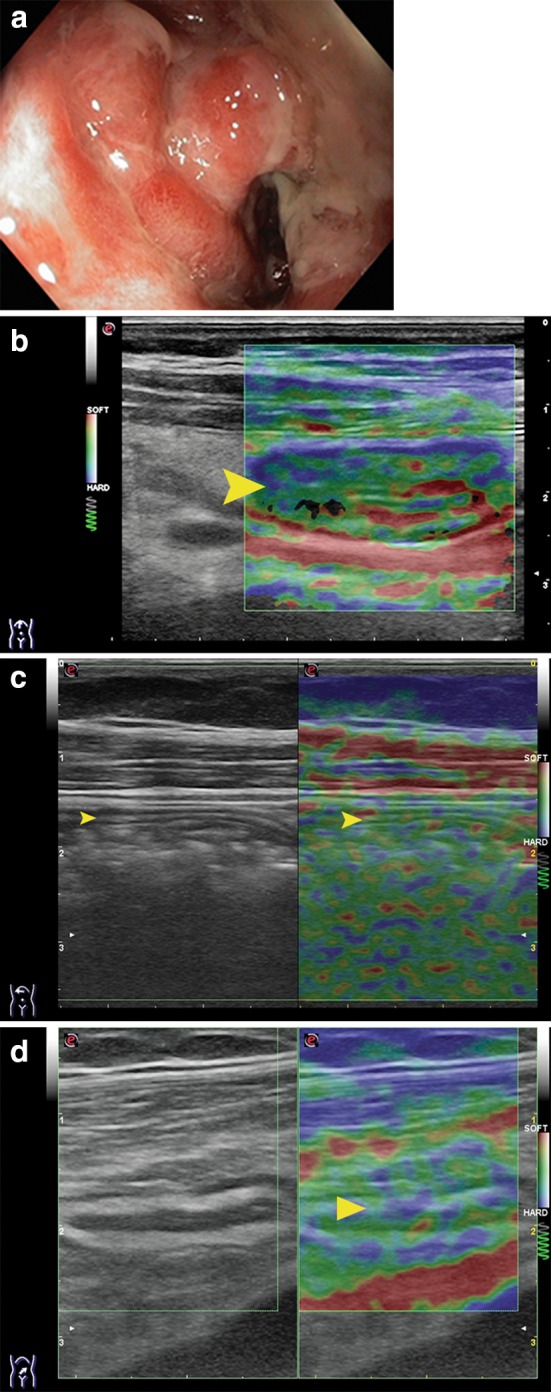
a Endoscopy of the transverse colon shows edema, mucosal erosion and ulceration (Mayo endoscopic score 3); examination performed before administration of infliximab therapy. b Corresponding strain elastography of the transverse colon shows moderate wall thickening, classified 2 BAR (green > blue > red, arrowhead). c Strain elastography of the transverse colon after 4 months of infliximab therapy shows normal colonic wall thickness and elasticity, classified 1B, arrowhead. d Strain elastography of the sigmoid colon after 4 months of infliximab therapy shows normal wall thickness (2.4 mm) and persistent abnormal elastographic appearance [classified 2BA (green > blue, arrowhead]
Fig. 8.
a Endoscopy shows the sigmoid colon with areas of congested mucosa separated by deep ulcerations (Mayo endoscopic score 3). b Corresponding strain elastography image of the sigmoid colon showing moderate wall thickening and abnormal elastographic appearance, classified 2BAR (mix of colors: green > blue > red) compatible with the endoscopic image showing very severe disease
Strain elastography of the colonic wall: Crohn’s disease
There are few data in the literature reporting on the use of strain elastography in Crohn’s disease. Havre et al. [4] carried out strain elastography on adequately prepared surgical specimens from patients with Crohn’s disease and found that the affected portions were stiffer than the surrounding colonic wall; these results were consistent with the histological findings of wall fibrosis.
Stidham et al. [8] showed that strain elastography can differentiate inflammatory from fibrotic intestine in rat models. Strain elastography was also carried out in seven patients with bowel stenosis in Crohn’s disease evidencing increased stiffness of the affected portion of the bowel as compared to the surrounding reference tissues.
We present images of persistent colitis in Crohn’s disease (over 10 years) during flare-up; the disease is affecting the sigmoid (Fig. 9), the descending and the transverse colon causing partial occlusion of the proximal portion of the transverse colon (Fig. 10).
Fig. 9.
a Endoscopy shows the sigmoid colon with extensive mucosal defects, marked edema, cobblestone appearance, bleeding on probing. b, c Strain elastography image of the sigmoid colon classified 2BAR (green > blue with small yellow and red spots) and the distal descending colon classified 2BRA (green > red > blue) these strain elastography patterns correlate with the acute phase of the disease as evidenced by endoscopy
Fig. 10.
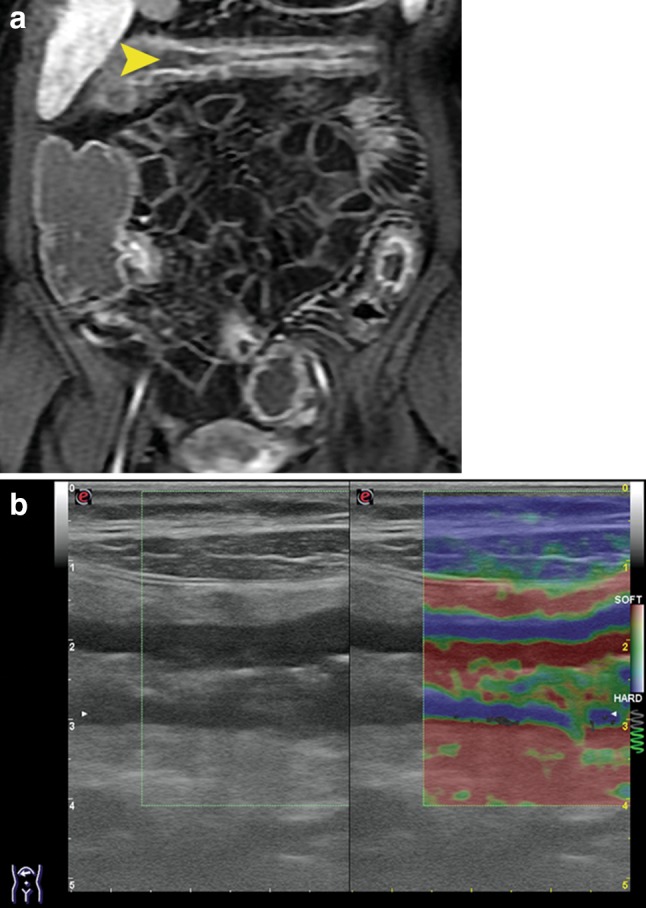
Same patient as Fig. 9. a Contrast enhanced MRI: the transverse colon presents localized enhancement mainly in the tunica mucosa and submucosa, arrowhead (suggesting that the disease is in the acute phase [9] ), there is luminal distension of the ascending colon due to partial occlusion of the proximal transverse colon. b Strain elastography of the proximal transverse colon: the appearance of the colonic wall suggests concomitant fibrosis/thickening of the muscular layer (predominantly blue) and inflammation of the mucosa and submucosa (green and red)
Strain elastography of the colonic wall: ischemic colitis
To the best of our knowledge, there are no data in the literature regarding the use of strain elastography in ischemic colitis. Ischemic colitis is a common cause of lower gastrointestinal tract bleeding. Reduced blood flow may be caused by changes in the systemic circulation or insufficient local blood supply. Ischemic injury varies depending on the extent and duration of insufficient blood supply and ranges from mild reversible mucous membrane involvement to transmural infarction.
We present two cases of ischemic colitis: one case is severe caused by hemorrhagic shock (Fig. 11a–c), and the other is a mild case caused by sigmoid volvulus followed by spontaneous remission (Fig. 11a1, b1). In these two cases, strain elastography was performed on the affected portion of the colon.
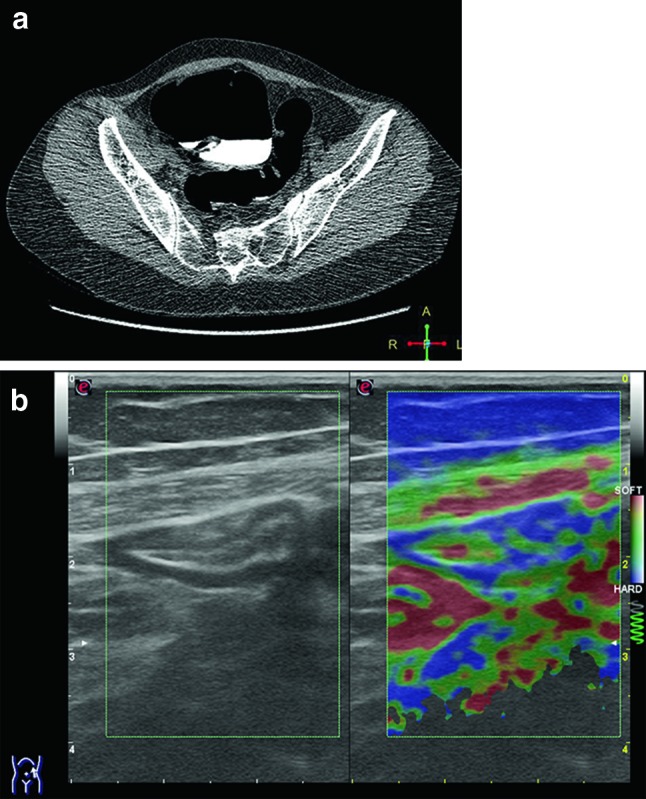
Fig. 11.

a Contrast-enhanced CT image showing the transverse colon and the splenic flexure (arrowhead) with thickened walls and hypoperfusion. b US image of the splenic flexure with thickened walls and loss of physiological echotexture. c Strain elastography image of the colon at the splenic flexure classified 2RBA (red > green > blue) suggestive of acute colitis. a1 Endoscopy shows the mucosa of the sigmoid colon, which appears diffusely hyperemic, fragile, eroded and bleeding on probing. b1 Corresponding strain elastography image classified 2BRA (green > red > blue, arrowhead)
Strain elastography of the colonic wall: diverticulosis and diverticulitis
To the best of our knowledge, there are no data in the literature regarding the use of strain elastography in colonic diverticulosis and diverticulitis. From a clinical point of view, diverticulosis may remain entirely asymptomatic. However, it can also cause pain in the lower abdomen without causing further complications or it may develop inflammatory complications ranging from diverticulitis to peridiverticular abscess. We present images of three cases of diverticular disease (Fig. 12a: asymptomatic, a1: symptomatic with mild diverticulitis, a2: acute diverticulitis which required hospitalization and intensive medical therapy). In these cases strain elastography completed grayscale US examination.
Fig. 12.

a Endoscopy show the sigmoid colon with distensible lumen and normal mucosa in addition to a diverticular orifice, also with normal mucosa. b Strain elastography image of the sigmoid colon showing normal thickness and elasticity (classified 1B, homogeneous green pattern, arrow); also the diverticulum (arrowhead) is predominantly green (1B). a1 Grayscale US and strain elastography of the sigmoid colon shows increased wall thickness and abnormal elasticity of the colonic wall, classified 2ARB (blue > red > green) and a diverticulum (hypoechoic at grayscale US, arrowhead) classified 2RBA (red > green > blue, arrowhead) at strain elastography. a2 Contrast-enhanced CT of the sigmoid colon shows wall thickening, edema and perivisceral phlegmon, arrowhead. b2 Corresponding strain elastography image of the sigmoid colon shows wall thickening and increased elasticity in the acute phase, classified 2BRA (green > red > blue). c2 Strain elastography of the sigmoid colon after 10 days of antibiotic therapy shows wall thickening classified 2ABR (blue > green > red) due to concomitant increased elasticity of the mucosa and submucosa (inflammation) with increased stiffness of the muscle layer (hyperplasia and fibrosis)
Abnormal strain elastography of the normal sigmoid colon wall
We present images of the sigmoid colon: virtual colonoscopy and strain elastography performed in a patient with constipation, lower abdominal pain and normal outcome of colonoscopy (Fig. 13).
Fig. 13.
a Virtual CT colonoscopy shows a thin-walled normal sigmoid colon, the dilated caecum is situated in the mid-abdomen. b Greyscale US: the sigmoid colon presents normal wall thickness with prevalence of the second hypoechoic layer (muscularis); strain elastography image is classified 2AB (blue > green), as the examined portion appears stiffer than normal
These images suggest that strain elastography may be influenced by the intrinsic contractile activity of the colonic wall. This may lead to diagnostic errors if changes in “functional” elasticity linked to hypertonic bowel movements are misdiagnosed as pathological phenomena of a different nature.
Conclusions
The aim of this pictorial essay is to provide a preliminary documentation of the “feasibility” of strain elastography in some frequent diseases affecting the colon.
Strain elastography of the gastrointestinal tract presents additional difficulties compared to more traditional applications (breast, thyroid) as the bowels are thin-walled cylindrical structures, which contain gas and present contracting motility. Furthermore, the effect of the pressure exerted with the probe is progressively reduced in the deeper lying tissues and the strain is therefore measurable only up to a few centimeters under the skin.
Bowels affected by disorders present thickened walls in the absence of motility and no intraluminal contents, so strain elastography of the affected portion is simpler than imaging of the normal portion of the gastrointestinal tract.
It goes without saying that further prospective research-targeted studies are required to evaluate the diagnostic accuracy and clinical relevance of the method. However, already at this stage it is clear that strain elastography permits visible distinction between normal and pathological elasticity of the colonic wall by characterizing it as more rigid or more flexible than normal.
Differentiation between the most frequent diseases of the colon with strain elastography and the visual classification is not possible as similar elastographic images are common to several diseases, such as ulcerative colitis, Crohn’s colitis, ischemic colitis, diverticular colitis as well as benign and malignant neoplasm.
This was confirmed by Havre et al. [4] who performed strain elastography to characterize adequately prepared surgical specimens from patients operated for malignant or benign colorectal lesions or Crohn’s disease [4].
In our opinion, strain elastography is very useful in clinical practice as it provides additional information required to characterize the intestinal wall in connection with chronic diseases, such as inflammatory bowel disease, diverticulosis and diverticulitis which all necessitate a prolonged follow-up. Indeed, assessment of the elasticity of the bowel wall (even if only qualitative) allows an indirect monitoring of inflammation or reparative fibrosis.
According to our initial experience, the different elastographic patterns seem to correlate with abnormalities evidenced at endoscopy in ulcerative colitis or Crohn’s colitis. In Crohn’s disease, it is also important to identify increased wall stiffness as an indirect indication of fibrosis. In one of the presented cases (Fig. 10), elastography seems to provide a good differentiation between increased stiffness affecting the tunica muscularis (suggestive of fibrosis) and increased elasticity of the submucosa and mucosa (suggestive of acute inflammation).
Finally in the presence of desmoplastic stromal response, strain elastography provides an accurate differential diagnosis between benign and malignant tumors of the colon.
Conflict of interest
Andrea Giannetti, Marco Biscontri and Marco Matergi have no conflict of interest.
Informed Consent
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2000 (5). All patients provided written informed consent to enrolment in the study and to the inclusion in this article of information that could potentially lead to their identification.
Human and animal studies
The study described in this article does not contain studies with human or animal subjects performed by any of the authors.
References
- 1.Cosgrove D, Piscaglia F, Bamber J, et al. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 2: clinical application. Ultraschall Med. 2013;34(3):238–253. doi: 10.1055/s-0033-1335375. [DOI] [PubMed] [Google Scholar]
- 2.Bamber J, Cosgrove D, Dietrich CF, et al. EFSUMB guidelines and recommendations on the clinical use of ultrasound elastography. Part 1: basic principles and technology. Ultraschall Med. 2013;34(2):169–184. doi: 10.1055/s-0033-1335205. [DOI] [PubMed] [Google Scholar]
- 3.Janssen J, Schlörer E, Greiner L. EUS elastography of the pancreas: feasibility and pattern description of the normal pancreas, chronic pancreatitis, and focal pancreatic lesions. Gastrointest Endosc. 2007;65(7):971–978. doi: 10.1016/j.gie.2006.12.057. [DOI] [PubMed] [Google Scholar]
- 4.Havre RF, Leh S, Gilja OH, et al. Strain assessment in surgically resected inflammatory and neoplastic bowel lesions. Ultraschall Med. 2014;35(2):149–158. doi: 10.1055/s-0032-1325535. [DOI] [PubMed] [Google Scholar]
- 5.Waage JE, Havre RF, Ødegaard S, et al. Endorectal elastography in the evaluation of rectal tumours. Colorectal Dis. 2011;13:1130–1137. doi: 10.1111/j.1463-1318.2010.02440.x. [DOI] [PubMed] [Google Scholar]
- 6.Participants in the Paris Workshop The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon. Gastrointest Endosc. 2003;58(6 suppl):s5–s43. doi: 10.1016/s0016-5107(03)02159-x. [DOI] [PubMed] [Google Scholar]
- 7.Ishikawa Daisuke, Ando Takafumi, Watanabe Osamu, et al. Images of colonic real-time tissue sonoelastography correlate with those of colonoscopy and may predict response to therapy in patients with ulcerative colitis. BMC Gastroenterol. 2011 doi: 10.1186/1471-230X-11-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Stidham Ryan W, Jingping Xu, Johnson Laura A, et al. Ultrasound elasticity imaging for detecting intestinal fibrosis and inflammation in rats and Humans with Crohn’s disease. Gastroenterology. 2011;141:819–826. doi: 10.1053/j.gastro.2011.07.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Cristina Stasi, Massimo Falchini, Stefano Milani (2012) Review article imaging modalities for the noninvasive assessment of fibrosis in Crohn’s disease. Sci World J. doi: 10.1100/2012/450151 [DOI] [PMC free article] [PubMed]