

Abstract
Objectives:
To determine the oral health related behavior, knowledge, attitudes, and practices of pre-university students of Mysore city.
Design:
A cross-sectional descriptive study was conducted among 1000 pre-university students of Mysore city.
Results:
Statistical tests such as percentage distribution and Chi-square were used. P values <0.05 were considered statistically significant. Most of the students (88%, n = 880) knew that dental health reflects on the general health. Eighty-nine percent (n = 890) of students were aware that sweets and sticky food cause dental decay. Majority of the students (90%, n = 900) agreed that they visited dentist only when they had pain and cleaned their teeth once daily using toothbrush and tooth paste in vertical and horizontal motion.
Conclusion:
The study showed that the students had good knowledge about the basic oral health measures necessary to maintain proper oral health, but their attitude and practices toward oral health was relatively poor.
Keywords: Attitude, knowledge, oral health, practice, pre-university college students
INTRODUCTION
Oral health is significantly related to oral health behaviors and their knowledge. Oral health knowledge contributes to good oral health, but unless attitudes and habits are developed and put into practice, little will be gained.[1] It is important to review the knowledge, attitude, and practices of the oral health of adolescents, even though they are educated, with the objectives of inculcating healthy lifestyles practices to last for a lifetime. Individuals who hold favorable oral health related beliefs over time have better oral health in their later years than those who do not. This implies that changing beliefs should result in changes in behaviors.[2]
Many studies have been conducted on perceived oral health, but have mostly concentrated on adults and old people.[3] The time trends, both for society and dental diseases, necessitate a focus on the period of adolescence when many habits that continue throughout life are initiated.
Adolescence has been identified as a time when personal oral health behaviors may be internalized and become habits, as parents become increasingly less directly involved in their children's care. Their increased autonomy may also mean that they fail to practice adequate oral home health care. They may tend to consume more snacks, and beverages between meals. Oral care during adolescence is important for several reasons, including the eruption of permanent dentition which increases the number of tooth surfaces that may decay and also results in increased early periodontal disease.[4] Thus, adolescents may be at greater risk for dental disease during a developmental period when they are establishing oral care habits.
Hence, the study was conducted with an aim to assess the oral health related knowledge, attitude, and practice among the 16–18-year-old pre-university college (PUC) students of Mysore city.
MATERIALS AND METHODS
The cross-sectional questionnaire-based survey was conducted among pre-university students of Mysore city during the period from December 2009 to March 2010.
As per the information obtained from the Deputy Director of Pre-University Education, Mysore, there were 15 PUCs distributed in five sectors in Mysore city. By using stratified simple random sampling, PUCs were selected from each sector by lottery method. For a population of 15,000 students, with a confidence level of 95% and a confidence interval of 5, the minimum sample size required was 375. However, the researcher studied 1000 students for higher accuracy. From each sector, 200 students were selected randomly to make up the sample size of 1000. Ethical clearance was obtained from the ethical committee of JSS Dental College and Hospital, Mysore.
Prior to the study, permission was obtained from the respective college principals and consent was taken from each student. The students were assessed using a structured questionnaire comprising closed-ended questions which included questions regarding the participants’ demographic details (age, gender, and place), oral health related knowledge, attitudes, and practices. A pilot study was conducted on 25 students to assess the validity of the questionnaire and they were not included in the actual study. Questions were explained whenever necessary, and the participants were given assurance regarding confidentiality of their responses and were requested to mark their answers and complete it individually. This procedure was carried out by an examiner and an assistant under the supervision of a staff member. The assistant helped the examiner in distributing the questionnaire, and the examiner gave instructions to the students regarding the questionnaire. Student's knowledge, attitude, and practices were assessed by using a questionnaire which included the following:
-
I
General information: About their parents’ education, socioeconomic status, etc
-
II
Knowledge: Oral health related knowledge on matters like causes and prevention of dental caries and gum disease, dietary habits (especially sugar consumption), fluoride, sources of dental health information and their perception of prosthetic appliances, malocclusion, misconceptions regarding oral health and its treatment, etc
-
III
Attitude: Attitude toward the prevention of oral diseases, dental visits, importance of dental care, etc., A 3-point Likert scale in which the responses were favorable attitude, average, and unfavorable attitudes was used
-
IV
Practices: Oral hygiene practices, mainly brushing and rinsing habits, frequency of dental visits, services received at the last visit, etc.
The collected data were coded and analyzed using SPSS 16 software. Appropriate statistical tests such as descriptive analysis and Chi-square were used to derive any significant differences among the responses given by students. P values <0.05 were considered statistically significant. For the purpose of analysis, the individual scores were summed up to yield a total score. The mean scores were obtained and an ordinal scale was developed for knowledge, attitude, and practices.
RESULTS
The study population consisted of 47.8% (n = 478) boys and 52.2% (n = 522) girls, with a mean age of 17 ± 2 years. Most of their parents (40%) were educated till their secondary school level and 56% of the parents were doing business [Figure 1].
Figure 1.
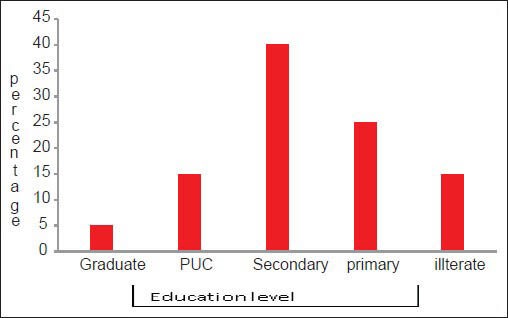
The bar diagram showing the distribution of the study population according to their parents’ education
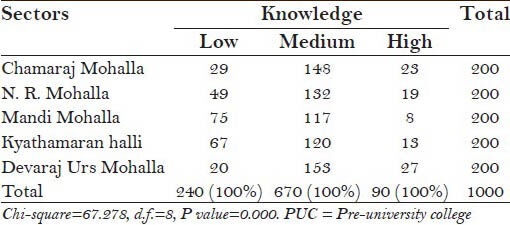
Most of the students (88%) knew that dental health is a major part of general health. Eighty-seven percent of the students considered that teeth are important for esthetics. Eighty-nine percent (n = 890) of the students were aware that sweets and sticky food cause dental decay. Majority of the students (90%, n = 900) considered consuming alcohol, smoking, and chewing gutkha as harmful to dental health and causing cancer. Eighty-eight percent (n = 880) of the students knew that brushing properly prevents dental caries and gum problems. Majority of the students (77%, n = 770) were unaware of the availability of treatment for bleeding gums, and 82% (n = 820) considered replacement of teeth as being important to maintain good oral health. Most of the students (92%, n = 920) had no knowledge about the role of fluoride in prevention of dental caries. Only 4% (n = 40) of the students had knowledge regarding other oral hygiene aids like dental floss and mouth rinse. Most of the participants (52%, n = 520) believed that bad breath is caused by poor oral hygiene and is treated by proper tooth and tongue brushing. Thirty-seven percent (n = 370) of the students said that soft drinks cause harm to teeth. Regarding the overall knowledge, 24% of the students had low level of knowledge, 67% had medium level of knowledge, and 9% had high level of knowledge. We found significantly higher levels of knowledge in Chamaraja Mohalla and Devraj Mohalla and lesser level in Mandi Mohalla [Table 1].
Table 1.
Oral health related knowledge among the PUC students of different sectors
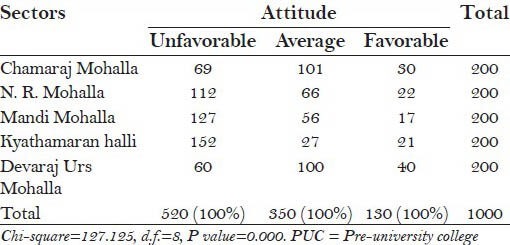
Majority of the students (90%, n = 900) agreed that they visited dentist only when they had pain. Most of the students thought that dental treatment is painful (88%, n = 880) and expensive (78%, n = 780). Also, 70% (n = 700) of the students agreed that extraction of upper teeth causes blindness and 68% (n = 680) thought that scaling causes loosening of teeth. Regarding overall attitude, 52% (n = 520) of the students had an unfavorable attitude, 35% (n = 350) had an average attitude, and 13% (n = 130) had a favorable attitude. We found significantly favorable attitude in Devraj Urs Mohalla and Chamaraj Mohalla compared to other mohallas [Table 2].
Table 2.
Oral health related attitude among the PUC students of different sectors
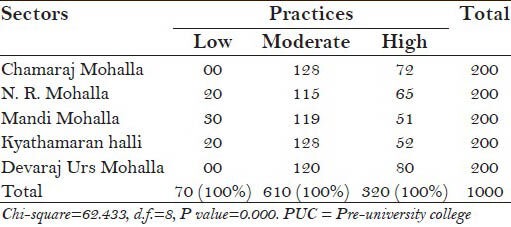
Only 30% (n = 300) of the students visited dentists regularly. Majority of the students (90%, n = 900) cleaned their teeth once daily using toothbrush and tooth paste in vertical and horizontal motion. There was no statistically significant difference between regular brushing practice and the study subjects’ parents’ occupation (P < 0.05). Also, 79% (n = 790) of the students had the habit of snacking in between meals. 68.7% (n = 679) of the students did not use to rinse their mouth after eating. Table 3 shows the frequency of changing tooth brush among students. Television advertisements were the popular mode of gaining knowledge regarding oral health among most of the students and seeing these advertisements, students selected tooth brush and paste [Figure 2]. None of the students used interdental aids for maintaining oral hygiene. Regarding the overall practices, 7% (n = 70) of the students had low level of practices, 61% (n = 610) had moderate level of practices, and 32% (n = 320) had a high level of practices. We found significant healthy practices in Devraj Urs Mohalla and Chamaraj Mohalla compared to other mohallas [Table 4].
Table 3.
Distribution of students based on the frequency of changing their tooth brush
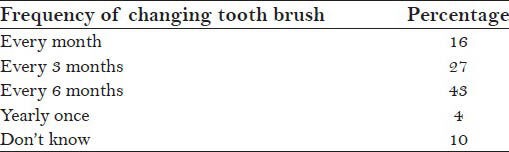
Figure 2.
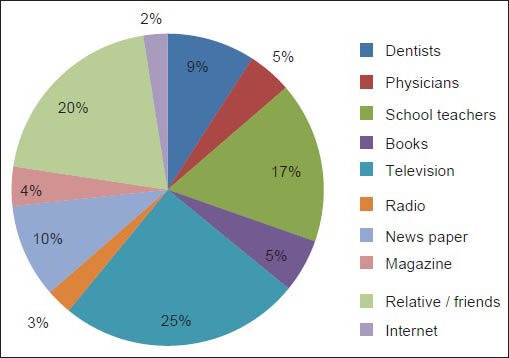
The distribution of students according to their sources of information regarding oral health
Table 4.
Oral health related practices among the PUC students of different sectors
DISCUSSION
In the present study, students demonstrated high awareness of the link between oral health and general health. It is important to mention that emphasizing on the link between oral health and the well-being of the rest of body might help in promoting oral health care and oral self-care practice among students, though a majority of the students knew that oral health contributes to esthetics. This finding is in agreement with that of a study conducted by Nagesh.[2]
In the present study, most of the students knew at least the basic causes and prevention of dental caries and gum diseases. But knowledge regarding fluoride, interdental aids, malocclusion, and harmful effects of soft drinks was low. These results are in agreement with other studies.[5,6,7,8,9] This could be a result of the oral health knowledge that they had acquired either at primary school level or through the media. Adequate knowledge on the causes, prevention, and signs of dental caries and gum disease depicts that students can retain and recall the acquired knowledge as they grow. Similar to the findings of this study, a high proportion of students with adequate level of knowledge on cigarette smoking as a cause of oral cancer were also reported in Tanzania,[5] Kenya,[10] and UK.[11]
Only 30% students visited dentist when they had dental pain. This is similar to the result of Kikwilu et al.'s[12] study, whereas the study results of Carneiro et al.[5] are not in agreement with our study. Gómez et al.,[13] in their report, highlight the importance of early detection as a cornerstone to improve survival.
Majority of the students thought that dental treatment is costlier and painful, which might be due to fear. It has been suggested that the modification of attitude allows a change in the behavior, which further causes attitude modification in most of the students who complained that dental treatment was painful and costly.
Certain oral diseases, such as chronic periodontitis and caries, that are considered as public health problems may be alleviated by effective and regular self tooth brushing. The study results revealed once-a-day tooth brushing practiced by majority of the participants. Similar results were obtained in other studies.[14,15,16,17]
Tooth brush and tooth paste were commonly used for brushing among the study population, which is in agreement with the findings of other studies.[5,18,19] In the present study, students did not use any interdental aids, whereas most of the students in Tanga Region, Tanzania[5] used interdental aids, mainly tooth pick, to maintain their oral hygiene.
CONCLUSION
The students had good knowledge on the basic oral health measures necessary to maintain proper oral health, but their attitude and practices toward oral health were relatively poor. The study showed that students who had knowledge and positive attitudes of oral health involved themselves in good practices of oral health maintenance. Factors like culture, education level of parents, socioeconomic status, etc., influence the knowledge, attitude, and practices.[20] Oral health education programs should be conducted with reinforcement, so that students can close the gap between knowledge and practice by changing their attitude from negative to positive one. In this study, we assessed the need for oral health education and treatment programs at Mandi Mohalla, N. R. Mohalla, and Kyathasandra. Students should be motivated to get regular dental checkups done. Television can be used as a medium to impart oral health related knowledge.
ACKNOWLEDGEMENT
Dr. Sunitha S and All the students who have participated in the study.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.McGrath C, Sham AS, Ho DK, Wong JH. The impact of dental neglect on oral health: A population based study in Hong Kong. Int Dent J. 2007;57:3–8. doi: 10.1111/j.1875-595x.2007.tb00111.x. [DOI] [PubMed] [Google Scholar]
- 2.Nagesh H. Oral Health related knowledge, attitude and practice [KAP] among 16-18 yr old students of 4 pre-university colleges in Bangalore south India. RGUHS J Dent Sci. 2008;2:12–8. [Google Scholar]
- 3.Ostberg AL, Jarkman K, Lindblad U, Halling A. Adolescents’ perceptions of oral health and influencing factors: A qualitative study. Acta Odontol Scand. 2002;60:167–73. doi: 10.1080/000163502753740197. [DOI] [PubMed] [Google Scholar]
- 4.Coolidge T, Heima M, Johnson EK, Weinstein P. The dental neglect scale in adolescents. BMC Oral Health. 2009;9:2. doi: 10.1186/1472-6831-9-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Carneiro L, Kabulwa M, Makyao M, Mrosso G, Choum R. Oral health knowledge and practices of secondary school students, Tanga, Tanzania. Int J Dent 2011. 2011:806258. doi: 10.1155/2011/806258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Masanja IM, Mumghamba EG. Knowledge on gingivitis and oral hygiene practices among secondary school adolescents in rural and urban Morogoro, Tanzania. Int J Dent Hyg. 2004;2:172–8. doi: 10.1111/j.1601-5037.2004.00096.x. [DOI] [PubMed] [Google Scholar]
- 7.Kahabuka FK, Mbawalla HS. Oral health knowledge and practices among Dar es Salaam institutionalized former street children aged 7-16 years. Int J Dent Hyg. 2006;4:174–8. doi: 10.1111/j.1601-5037.2006.00215.x. [DOI] [PubMed] [Google Scholar]
- 8.Al-Ansari J, Honkala E, Honkala S. Oral health knowledge and behavior among male health sciences college students in Kuwait. BMC Oral Health. 2003;3:2. doi: 10.1186/1472-6831-3-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Al-Omiri MK, Al-Wahadni AM, Saeed KN. Oral health attitudes, knowledge, and behavior among school children in North Jordan. J Dent Educ. 2006;70:179–87. [PubMed] [Google Scholar]
- 10.Komu P, Dimba EA, Macigo FG, Ogwell AE. Cigarette smoking and oral health among healthcare students. East Afr Med J. 2009;86:178–82. doi: 10.4314/eamj.v86i4.46948. [DOI] [PubMed] [Google Scholar]
- 11.Warnakulasuriya KA, Harris CK, Scarrott DM, Watt R, Gelbier S, Peters TJ, et al. An alarming lack of public awareness towards oral cancer. Br Dent J. 1999;187:319–22. doi: 10.1038/sj.bdj.4800269. [DOI] [PubMed] [Google Scholar]
- 12.Kikwilu EN, Masalu JR, Kahabuka FK, Senkoro AR. Prevalence of oral pain and barriers to use of emergency oral care facilities among adult Tanzanians. BMC Oral Health. 2008;8:28. doi: 10.1186/1472-6831-8-28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Gómez I, Warnakulasuriya S, Varela-Centelles PI, López-Jornet P, Suárez-Cunqueiro M, Diz-Dios P, et al. Is early diagnosis of oral cancer a feasible objective? Who is to blame for diagnostic delay? Oral Dis. 2010;16:333–42. doi: 10.1111/j.1601-0825.2009.01642.x. [DOI] [PubMed] [Google Scholar]
- 14.Masalu J, Mtaya M, Astrøm AN. Risk awareness, exposure to oral health information, oral health related beliefs and behaviours among students attending higher learning institutions in Dar es Salaam, Tanzania. East Afr Med J. 2002;79:328–33. doi: 10.4314/eamj.v79i6.8854. [DOI] [PubMed] [Google Scholar]
- 15.Astrøm AN, Jackson W, Mwangosi IE. Knowledge, beliefs and behavior related to oral health among Tanzanian and Ugandan teacher trainees. Acta Odontol Scand. 2000;58:11–8. doi: 10.1080/000163500429370. [DOI] [PubMed] [Google Scholar]
- 16.Yazdani R, Vehkalahti MM, Nouri M, Murtomaa H. Smoking, tooth brushing and oral cleanliness among 15- year-olds in Tehran, Iran. Oral Health Prev Dent. 2008;6:45–51. [PubMed] [Google Scholar]
- 17.Petersen PE, Hoerup N, Poomviset N, Prommajan J, Watanapa A. Oral health status and oral health behavior of urban and rural schoolchildren in Southern Thailand. Int Dent J. 2001;51:95–102. doi: 10.1002/j.1875-595x.2001.tb00829.x. [DOI] [PubMed] [Google Scholar]
- 18.Nyandindi U, Palin-Palokas T, Milén A, Robison V, Kombe N. Oral health knowledge, attitudes, behaviour and skills of children entering school in urban and rural areas in Tanzania. Pub Health. 1994;108:35–41. doi: 10.1016/s0033-3506(05)80033-2. [DOI] [PubMed] [Google Scholar]
- 19.Tubaishat RS, Darby ML, Bauman DB, Box CE. Use of miswak versus toothbrushes: Oral health beliefs and behaviours among a sample of Jordanian adults. Int J Dent Hyg. 2005;3:126–36. doi: 10.1111/j.1601-5037.2005.00136.x. [DOI] [PubMed] [Google Scholar]
- 20.Ahmed S, Solaiman F, Islam MR, Akhter SM, Nizami MZ, Khatun MA. Attitude on Oral Hygiene among the school going children in selected schools at Dhaka city. City Dent Col J. 2013;10:41–6. [Google Scholar]