

Abstract
Context:
To strengthen the surveillance system in India, Integrated Disease Surveillance Program (IDSP) was launched in 2004. The frequent occurrence of epidemics even after the launching of the IDSP was an indication toward inadequacy of the system. The responsibility for effective implementation of IDSP at the sub-center level lies with the health workers.
Aims:
The aim of the following study was to assess the knowledge and practice of health workers regarding IDSP and to assess the quality of IDSP reports at the sub-center level.
Settings and Design:
It was cross-sectional study carried out in the area under Community Health Center Dighal which is the rural field practice area attached to Post Graduate Institute of Medical Sciences, Rohtak in the State of Haryana, India. Subjects and Methods: All the 24 sub-centers in the area were visited and 46 health workers (22 male; 24 female) who met the inclusion criteria i.e. who had completed 1 year of their service or had been trained for IDSP, were included in the study. Data were collected on a self-designed, semi-structured and pre-tested schedule by interviewing the study subjects and observation of the records/reports.
Statistical Analysis Used:
Percentages and proportions.
Results:
Only 14/46 (~30%) of the workers could expand the abbreviation “IDSP” correctly. Only 4/46 (~9%) workers could narrate any of the trigger events and none could tell all the trigger events. Only at 12 such sub-centers, diagnoses were being written in their out-patient registers according to the defined syndromes. 43/46 (~93%) workers were not aware of the zero reporting.
Conclusions:
The surveillance system is much less alert and intense than the desired level and needs to be strengthened.
Keywords: Disease, gaps, integrated disease surveillance program, surveillance, track
Introduction
To strengthen the surveillance system in India, Integrated Disease Surveillance Program (IDSP) was launched in 2004.[1] IDSP is a decentralized, state based surveillance program which is intended to detect early warning signals of impending outbreaks and help initiate an effective response in a timely manner, thereby preventing plenty of cases. It is also expected to provide essential data to monitor progress of on-going disease control programs and help allocate health resources more efficiently. The frequent occurrence of epidemics even after launching of the IDSP,[1,2,3,4,5] was an indication toward inadequacy of the surveillance system and/or preparedness to identify and control outbreaks in a timely manner. Under the program, sub-centers constitute important component in the network of reporting units from where weekly surveillance data are being collected on “S” (syndromic) surveillance formats using standard case definitions. At the sub-center level, the responsibility for effective implementation of IDSP lies with the health workers.[6] The present study was planned to assess the knowledge and practice of health workers regarding IDSP and to assess the quality of IDSP reports at the sub-center level.
Subjects and Methods
It was cross-sectional study carried out during the period of year from 2010 to 2011 in the area under Community Health Center (CHC) Dighal (District - Jhajjar) which is the rural field practice area attached to Department of Community Medicine, Post Graduate Institute of Medical Sciences, Rohtak in the State of Haryana, India. All the sub-centers in the area were visited and health workers who had completed 1 year of their service or had been trained for IDSP were included in the study. The workers who did not meet any of these criteria i.e. the newly recruited ones whose length of service was <1 year and those who had not received any training regarding IDSP were excluded from the study. A total of 46 such health workers (22 male; 24 female) serving in the area, were selected and were interviewed. Data were collected on a self-designed, semi-structured and pre-tested schedule by interviewing the selected study subjects and observation of the records/reports available at the sub-centers. The data so collected were tabulated, analyzed using percentages and proportions and interpreted accordingly. Prior permission to carry out the study was sought. Participation to the study was voluntary. Informed consent was also obtained from the respondents and they were assured of confidentiality of their responses.
Results and Discussion
Response rate was 100% as all the study workers completed the interviews. Out of 46, 39 (~85%) workers knew about IDSP i.e. they had heard about the term “IDSP,” but only 14/46 (~30%) of the workers could expand the abbreviation correctly. Trigger levels were not known to 42/46 (~91%) of health workers indicating that substantial number workers were not aware of the utility of reports. Only 4/46 (~9%) could narrate any of the trigger events and none could tell all the trigger events [Table 1].
Table 1.
Knowledge of health workers regarding IDSP
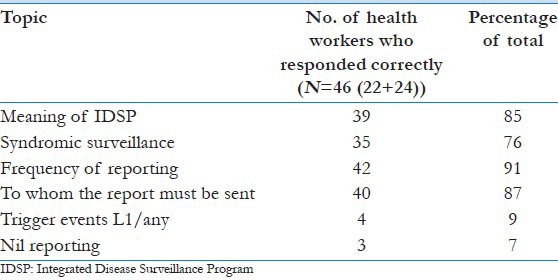
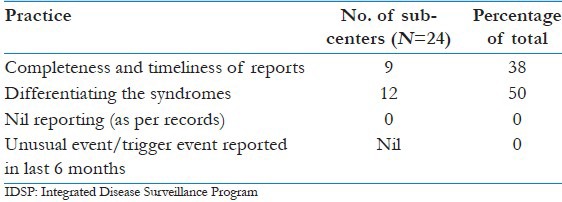
All the sub-centers were sending reports on regular basis but the reports were being sent within the prescribed time limit by only 9/46 (~38%) sub-centers which is a proxy indicator for the status of alertness of the surveillance system and a reflection on the performance of the reporting units. Only 12 such sub-centers were writing in their out-patient registers the diagnoses according to syndromes identifiable as per prescribed case definitions. None of the sub-centers were practicing zero reporting and 43/46 (~93%) workers were not even aware of the zero reporting [Tables 1 and 2]. This reflects that there is a possibility that even the quality supervision might be lacking or the supervisors themselves were not aware about the importance of “nil” reporting.
Table 2.
Practices and quality of IDSP reports among selected sub-centers
So far appraisal of IDSP has probably been a relatively neglected subject in comparison to that of other national health programs. However, findings of the available relevant studies were discussed here. In an evaluation study conducted at Kannur District of Kerala in 2009, it was recommended to organize more number of training programs and retraining after a lapse of 1 year for medical officers (MOs) working in the Primary Health Centers, CHCs, Block Primary Health Centers, etc., However, peripheral workers of the sub-centers were not included in the study.[7] To improve the reporting and the possibility of generation of more timely alerts regarding outbreaks, innovative interventions like introduction of SMS based surveillance were pilot tested by Indian Institute of Public Health, Hyderabad and had been found effective even in resource constraint areas of Andhra Pradesh State of India.[8] An appraisal of national disease surveillance systems in India is being carried out by Research Fellows from Public Health Foundation of India, which could probably document the learning's from the past two decades to help preparation of the next generation of surveillance strategies.[9] In an unpublished study entitled “Evaluation of Integrated Diseases Surveillance Project Bellary Unit, Karnataka State,” absence of clarity in case definitions, lack of a system of quality control for the data collected and inadequate analysis of data for meaningful interpretation were identified as the important gaps in IDSP. In addition, the surveillance unit had to ask repeatedly for sending the weekly reports.[10] Regular analyses of surveillance data as those presented in a study conducted by Gupta et al., would be helpful in timely identification of deviations in the effective control of the diseases.[11]
Limitations
Due to the constraints of limited time and feasibility of the study, the authors could not interview the MOs/multipurpose health supervisors (MPHS) supervisors of the selected health workers to know their perspectives. The issues which need to be further assessed are, for example, whether the MOs and MPHS are supervising the health workers or not, or whether the feedback is being got from and provided to the peripheral staff i.e. the health workers posted at the reporting units or not, etc.
Conclusions and Recommendations
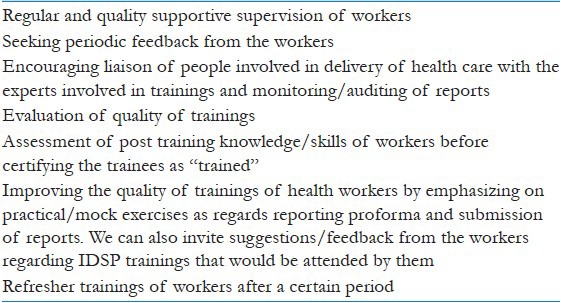
The surveillance system is not as intense as supposed to be and the cases are likely to be detected at a time when the disease would have had already caused sufficient damage to health of people before any control measure could be initiated. Some areas which need to be focused are highlighted below in Table 3.
Table 3.
Target areas which need to be focused/further assessed
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.New Delhi: Government of India; 2004. [Last cited on 2013 Jun 20]. Ministry of Health and Family Welfare. Integrated Disease Surveillance Project. Available from: http://www.idsp.nic.in . [Google Scholar]
- 2.Goel MK, Malik JS, Khanna P, Gaur DR, Behera BK, Yadav RK. Sero-epidemiological investigation of an outbreak of fever in rural area of Rohtak. J Commun Dis. 2009;41:215–7. [PubMed] [Google Scholar]
- 3.Deswal D. Haryana prepares action plan to eradicate Hepatitis C. The Times of India, 2012 Sep 12; [about 3 screens] [Last cited on 2013 Jan 30]. Available from: http://www.articles.timesofindia.indiatimes.com/2012-09-12/india/33788806_1_ ratia-action-plan-viral-load .
- 4.Prinja S, Kumar S, Reddy GM, Ratho RK, Kumar R. Investigation of viral hepatitis E outbreak in a town in Haryana. J Commun Dis. 2008;40:249–54. [PubMed] [Google Scholar]
- 5.Kumar RL, Pallab R, Subhash V, Prinja S, Kumar S, Reddy GM, et al. An outbreak of food borne illness in a medical institution of Chandigarh. J Community Dis. 2009;41:293–5. [Google Scholar]
- 6.New Delhi: Government of India; 2004. [Last cited on 2013 Jun 20]. Ministry of Health and Family Welfare. Health Workers’ Operations Manual. Available from: http://www.nvbdcpchd.gov.in/Health%20Workers%20Manual.pdf . [Google Scholar]
- 7.Borker S, Venugopalan PP. Evaluation of the integrated disease surveillance project training at Kannur district of North Kerala. Indian J Public Health. 2010;54:48. doi: 10.4103/0019-557X.70558. [DOI] [PubMed] [Google Scholar]
- 8.Bhubaneshwar: Public Health Foundation of India; 2009. [Last updated on 2012; Last cited on 2013 Jun 20]. Indian Institute of Public Health. Systemic Evaluation of Integrated Disease Surveillance Program to Assess the Impact of SMS Based Reporting in Andhra Pradesh. Available from: http://www.phfi.org/research/403 . [Google Scholar]
- 9.Public Health Foundation of India. New Delhi: PHFI; 2010. [Last updated on 2013; Last cited on 2013 Jun 15]. An appraisal of national disease surveillance systems in India: from NSPCD to IDSP and beyond. Available from: http://www.phfi.org . [Google Scholar]
- 10.Sathyanarayana An evaluation of integrated diseases surveillance project Bellary Unit Karnataka State, INDIA Docstoc. 2011. [Last cited on 2013 May 24]. Available from: http://www.docstoc.com/docs/43705103/An - Evaluation - of - Integrated - Diseases - Surveillance - Project - Bellary - Unit .
- 11.Gupta SN, Gupta N, Gupta S. Surveillance data analysis of Revised National Tuberculosis Control Program of Kangra, Himachal Pradesh. J Family Med Prim Care. 2013;2:250–5. doi: 10.4103/2249-4863.120730. [DOI] [PMC free article] [PubMed] [Google Scholar]