

Abstract
There are two objectives. One is to show the differences in the mechanical properties of various dental restorative materials compared to those of enamel and dentin. The other is to ascertain which dental restorative materials are more suitable for clinical treatments. Amalgam, dental ceramic, gold alloy, dental resin, zirconia, and titanium alloy were processed as dental restorative material specimens. The specimens (width, height, and length of 1.2, 1.2, and 3.0 mm, respectively) were compressed at a constant loading speed of 0.1 mm/min. The maximum stress (115.0 ± 40.6, 55.0 ± 24.8, 291.2 ± 45.3, 274.6 ± 52.2, 2206.0 ± 522.9, and 953.4 ± 132.1 MPa), maximum strain (7.8% ± 0.5%, 4.0% ± 0.1%, 12.7% ± 0.8%, 32.8% ± 0.5%, 63.5% ± 14.0%, and 45.3% ± 7.4%), and elastic modulus (1437.5 ± 507.2, 1548.4 ± 583.5, 2323.4 ± 322.4, 833.1 ± 92.4, 3895.2 ± 202.9, and 2222.7 ± 277.6 MPa) were evident for amalgam, dental ceramic, gold alloy, dental resin, zirconia, and titanium alloy, respectively. The reference hardness value of amalgam, dental ceramic, gold alloy, dental resin, zirconia, and titanium alloy was 90, 420, 130–135, 86.6–124.2, 1250, and 349, respectively. Since enamel grinds food, its abrasion resistance is important. Therefore, hardness value should be prioritized for enamel. Since dentin absorbs bite forces, mechanical properties should be prioritized for dentin. The results suggest that gold alloy simultaneously has a hardness value lower than enamel (74.8 ± 18.1), which is important in the wear of the opposing natural teeth, and higher maximum stress, maximum strain, and elastic modulus than dentin (193.7 ± 30.6 MPa, 11.9% ± 0.1%, 1653.7 ± 277.9 MPa, respectively), which are important considering the rigidity to absorb bite forces.
Keywords: Enamel, dentin, stress, strain, elastic modulus
Introduction
Dental caries typically damage tooth enamel and dentin. Tooth function and shape are impaired by damage, although they can be recovered and restored by dental treatments. Dental restorative materials are used to clinically treat and reconstruct damaged teeth as well as to recover their functions.1,2
Amalgam and dental resin are commonly used as cavity-filling materials for enamel and dentin that are damaged by dental caries.3 Dental resin, dental ceramic, and zirconia are used for the aesthetic fabrication of denture resin teeth.4–6 In particular, they are used for inlay procedures because they can be made of a color that is very similar to natural teeth.7 Gold alloy, which has the same thermal conductivity as natural teeth, is used in inlay, crown, and bridge procedures.4,7 Titanium alloy dental implants are performed when the entire tooth is lost; titanium alloy is also used to produce implant abutments, denture frameworks, and implant fixtures.8
During mastication, bite forces are applied on the occlusal area of the tooth. These bite forces comprise a vertical compression force and a lingual side compression force. Most previous studies on dental restorative materials investigated the stress–strain curves of materials and hardness values based on indentation tests.9–12 Each of these studies focused only on one dental material; none were comparative studies of the mechanical properties of dental restorative materials and dental hard tissues. Furthermore, no studies have investigated the mechanical properties of dental restorative materials and dental hard tissues with specimens of identical shape and dimension. This is a significant gap in existing research as the mechanical properties of dental restorative materials and dental hard tissues may vary with the shapes and dimensions of test specimens. Furthermore, as dental hard tissue (enamel and dentin) is a nonhomogeneous and anisotropic material, it does not obey Hooke’s Law. Therefore, it is not feasible to compare the mechanical properties based on the elastic modulus alone. It is essential to also consider the stress and strain values.
In this study, the mechanical properties of various dental restorative materials (amalgam, dental ceramic, dental resin, gold alloy, zirconia, and titanium alloy) were determined using test specimens of identical shape and dimensions under the same compressive test conditions. The hardness values of enamel and dentin, obtained from a previous study,13 were compared with those of the dental restorative materials obtained in other previous studies.14–19
The results of this study might help in identifying which dental restorative materials show optimal mechanical properties and hardness values approaching those of enamel and dentin.
Materials and methods
Specimen preparation
Amalgam (Cavex 68; CAVEX, Netherland), dental ceramic (Omega 900; Vident, USA), dental gold alloy (Autofluid® 2PF; Metalor, USA), dental resin (Sinfony; 3M, USA), zirconia (LavaTM Frame Framework Ceramic; 3M), and titanium alloy (Daesung, Korea) were processed as dental restorative material specimens. For each material, 10 specimens with width, height, and length of 1.2, 1.2, and 3.0 mm, respectively, were used (Figure 1). The geometric error was ±0.02 mm from the machine-cut processes below. The materials were machine cut at a feeding speed of 0.2 mm/s and 1000 revolutions per minute (RPM) using a model 140-5L water spray-cooled carborundum wheel (PSI, USA) in a RB216 Culux micro-diamond saw machine (R&B, Korea). Each specimen was prepared for testing after it was wet-sand polished using a METPOL2 device (R&B) using #3000 wet sanding polisher at 45 RPM. After polishing, each specimen was viewed with an IX71 microscope (Olympus, Japan) at 40× magnification to check for the presence of cracks and to identify any potential damage that may have occurred during polishing. No cracks were found in most of the specimens.
Figure 1.
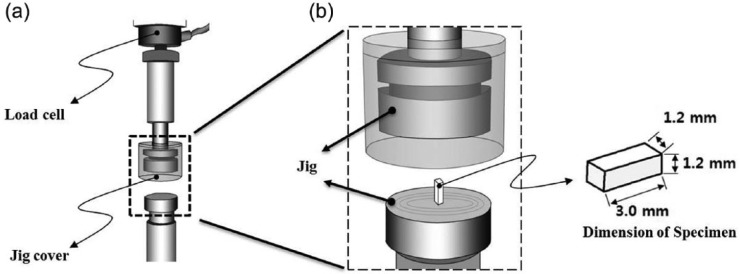
Compression test jig of micro-test machine: (a) Jig—jig cover was installed to prevent the broken pieces from popping when the specimens reached their breaking points and (b) compression test was performed after placing the specimens on the lower jig and lowering the upper jig.
Compression test
A micro-load system (Universal Testing System; R&B) with ±0.5% operating accuracy was used for the compression tests. The volume of the load cell was evaluated from the failure loads of the specimens. The 10 kilogram force (kgf) UM-K10 load cell (Dacell, Korea) was installed in the upper jig of the micro-load system to measure the compressive force of the specimen during the compression tests (Figure 1(a)). The system was used for amalgam, dental ceramic, and dental resin specimens. A SM603 100 kgf load cell (MScell, Korea) was used for gold alloy specimens, and a UM-K500 500 kgf load cell (Dacell) was used for zirconia and titanium alloy specimens. A prepared specimen was placed on the lower jig (Figure 1(b)), and a compression test was performed by lowering the upper jig at a constant loading speed of 0.1 mm/min. The compressive stresses (σ in MPa), strains (ϵ in %), and elastic modulus (E, MPa) of the dental restorative materials were calculated using equations (1) and (2), and the elastic modulus was calculated using equation (3)
| (1) |
where σ is the compressive stress, P is the load or force, and A is the cross-sectional area of specimen
| (2) |
where ϵ (%) is the strain, l is the original length, l′ is the changed length, and
| (3) |
where E is the elastic modulus.
Results
Compression test
Table 1 shows the mean values and standard deviations of the maximum stress (MPa), maximum strain (%), and E (MPa) for dental restorative materials tested, enamels, and dentins. Here, the maximum stress and maximum strain were obtained at the yield point. The mean values and standard deviations of the maximum stress (MPa), maximum strain (%), and E (MPa) of enamel and dentin were obtained from a previous study.13 SPSS statistical software (USA) was used to conduct independent sample t-tests to examine the significance of the maximum stress, maximum strain, and E values.
Table 1.
Mechanical properties from compression tests (n = 10 for each material) and their hardness values of dental hard tissues and dental restorative materials.
| Materials | Maximum stress (MPa) | Maximum strain (%) | Elastic modulus (MPa) | Vickers hardness values (HV) |
|---|---|---|---|---|
| Enamel | 62.2 ± 23.8 | 4.5 ± 0.8# | 1338.2 ± 307.9† | 274.8 ± 18.1 |
| Dentin | 193.7 ± 30.6 | 11.9 ± 0.1 | 1653.7 ± 277.9† | 65.6 ± 3.9 |
| Amalgam | 115.0 ± 40.6 | 7.8 ± 0.5 | 1437.5 ± 507.2† | 90 |
| Dental ceramic | 55.0 ± 24.8 | 4.0 ± 0.1# | 1548.4 ± 583.5† | 420 |
| Gold alloy | 291.2 ± 45.3 | 12.7 ± 0.8 | 2323.4 ± 322.4* | 130–135 |
| Dental resin | 274.6 ± 52.2 | 32.8 ± 0.5 | 833.1 ± 92.4 | 86.3–124.2 |
| Zirconia | 2206.0 ± 522.9 | 63.5 ± 14.0 | 3895.2 ± 202.9 | 1250 |
| Titanium alloy | 953.4 ± 132.1 | 45.3 ± 7.4 | 2222.7 ± 277.6* | 349 |
Significant difference (p > 0.05) based on t-test.
Significant difference (p > 0.05) based on t-test.
Significant difference (p > 0.1) based on t-test.
The maximum stress of amalgam, dental ceramic, gold alloy, dental resin, zirconia, and titanium alloy specimens was 115.0 ± 40.6, 55.0 ± 24.8, 291.2 ± 45.3, 274.6 ± 52.2, 2206.0 ± 522.9, and 953.4 ± 132.1 MPa, respectively. The maximum strain of amalgam, dental ceramic, gold alloy, dental resin, zirconia, and titanium alloy specimens was 7.8% ± 0.5%, 4.0% ± 0.1%, 12.7% ± 0.8%, 32.8% ± 0.5%, 63.5% ± 14.0%, and 45.3% ± 7.4%, respectively. As shown in Table 1, the maximum strain of dental ceramic was not significantly different from that of enamel (p > 0.05). The elastic modulus value of the amalgam, dental ceramic, gold alloy, dental resin, zirconia, and titanium alloy specimens was 1437.5 ± 507.2, 1548.4 ± 583.5, 2323.4 ± 322.4, 833.1 ± 92.4, 3895.2 ± 202.9, and 2222.7 ± 277.6 MPa, respectively. No significant differences were observed among the elastic modulus values of enamel, dentin, amalgam, and dental ceramic (p > 0.1). Furthermore, no significant difference was observed between the elastic modulus values of zirconia and titanium alloy (p > 0.05).
Figure 2 shows the typical stress–strain curve of each dental restorative material. Since the linear regression equation indicated that the R 2 value for amalgam, dental ceramic, gold alloy, dental resin, zirconia, and titanium alloy specimens was 0.9998, 0.9941, 0.9938, 0.9911, 0.9992, and 0.9983, respectively, slips and frictions between the jig (compressor) and specimen were assumed not to be presented during the test. Hereafter, the slope of the typical stress–strain curve of each material is considered to indicate the elastic modulus. Based on the slopes shown in Figure 2 and Table 1, the elastic modulus of zirconia was the largest, making it the stiffest material with a stiffness value of 3895.2 ± 202.9 MPa, and dental resin had the smallest, making it the least stiff material with a stiffness value of 833.1 ± 92.4 MPa.
Figure 2.
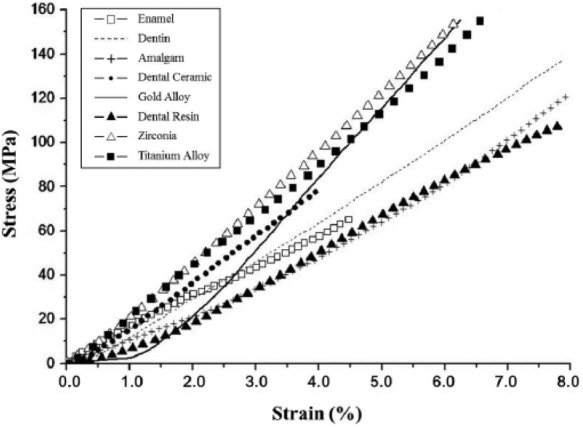
Typical stress–strain curves of dental restorative materials from compression tests.
Vickers hardness values
The Vickers hardness value of enamel (274.8 ± 18.1) was approximately 4.2 times greater than that of dentin (65.6 ± 3.9) (Table 1).13 The reference hardness value of amalgam, dental ceramic, gold alloy, dental resin, zirconia, and titanium alloy was 90, 420, 130–135, 86.3–124.2, 1250, and 349,14–19 respectively. The hardness values of dental hard tissues and dental restorative materials are listed in Table 1.
Discussion and conclusion
The mechanical role played by enamel is to grind (crush) food and protect dentin because of its higher wear resistance, and that played by dentin is to absorb bite forces because of its higher force resistance.13 Therefore, a replacement material for enamel should have a hardness value that is similar to or lower than that of enamel. A replacement material for dentin should have maximum stress, maximum strain, and elastic modulus similar to or higher than those of dentin.
Dental ceramic, zirconia, and titanium alloy showed higher hardness values compared to that of enamel (Table 1).
Amalgam, gold alloy, dental resin, zirconia, and titanium alloy showed higher maximum stress values than enamel. Amalgam, dental ceramic, gold alloy, dental resin, zirconia, and titanium alloy showed higher maximum strain values than enamel. Gold alloy, zirconia, and titanium alloy showed higher elastic modulus values than enamel (Table 1 and Figure 3). Gold alloy, dental resin, zirconia, and titanium alloy showed higher maximum stress values compared to dentin. Gold alloy, dental resin, zirconia, and titanium alloy showed higher maximum strain values compared to dentin. Gold alloy, zirconia, and titanium alloy showed higher elastic modulus values compared to dentin. From these results, gold alloy, zirconia, and titanium alloy were considerably suitable dental restorative materials for replacing dentin, only considering their mechanical properties to absorb bite forces (Table 1 and Figure 3).
Figure 3.
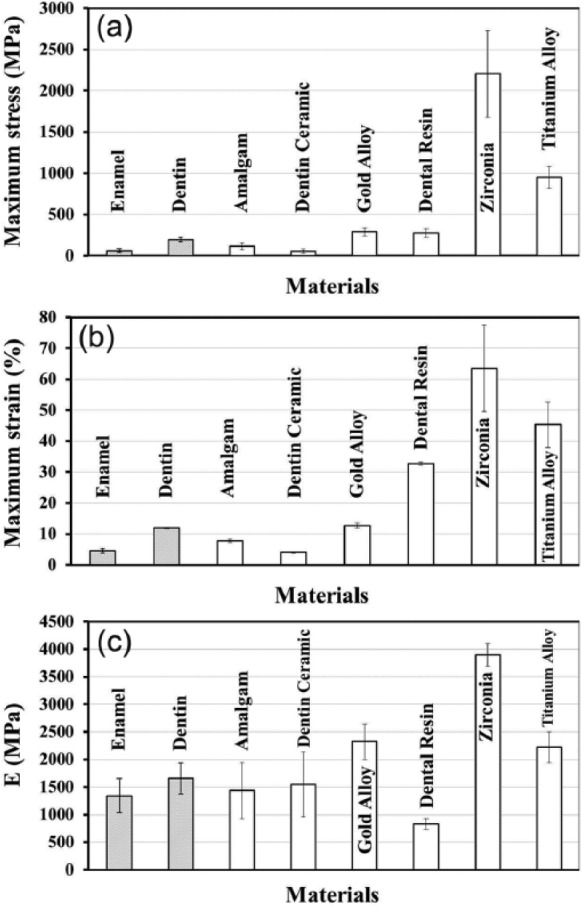
Comparison of (a) maximum stress (MPa), (b) maximum strain (%), and (c) elastic modulus (MPa) of each material from compression tests.
In dental treatments, amalgam, dental resin, and zirconia are the most commonly used dental restorative for cavity filling. Dental ceramic, gold alloy, and dental resin are usually used for inlay and/or onlay. However, maximum stress (2206.0 ± 522.9 MPa), maximum strain (63.5% ± 14.0%), and elastic modulus (3895.2 ± 202.9 MPa) of zirconia were significantly different from the maximum stress (62.2 ± 23.8, 193.7 ± 30.6 MPa), maximum strain (4.5% ± 0.8%, 11.9% ± 0.1%), and elastic modulus (1338.2 ± 307.9, 1653.7 ± 277.9 MPa) of enamel and dentin, respectively.13 The hardness value of zirconia is approximately 4.5 times higher than that (274.8 ± 18.1) of enamel and approximately 20 times higher than that (65.6 ± 3.9) of dentin.13 Thus, zirconia may have poor biocompatibility with natural teeth due to its markedly higher mechanical properties and hardness value.
Titanium alloy is a well-known suitable material for dental implants because of its biocompatibility and osseointegration. However, its maximum stress (953.4 ± 132.1 MPa), maximum strain (45.3% ± 7.4%), and elastic modulus (2222.7 ± 277.6 MPa) values are significantly different from the maximum stress (62.2 ± 23.8, 193.7 ± 30.6 MPa), maximum strain (4.5% ± 0.8%, 11.9% ± 0.1%), and elastic modulus (1338.2 ± 307.9, 1653.7 ± 277.9 MPa) values of enamel and dentin, respectively.13 Owing to the excessive mechanical properties of titanium alloy, the bite force applied by the dental implant, which adheres to the bone, would apply stress to the dental hard tissues and mandibular bones. Therefore, a new dental restorative material for dental implants that has mechanical properties similar to those of dental hard tissues and sufficient osseointegration needs to be developed for functional recovery and dental treatments.
In this study, the mechanical properties of dental hard tissues and various dental restorative materials were compared and studied with respect to the bite force. Furthermore, the hardness values of dental hard tissues and dental restorative materials were determined and analyzed with respect to the wear resistance.
Most dental treatments are aimed at simultaneously restoring the functions of enamel and dentin instead of addressing them separately. Because the mechanical role of enamel is grinding (crushing) food, its abrasion resistance is of vital importance; therefore, the hardness value should be prioritized when identifying replacement materials for enamel. In contrast, dentin absorbs bite forces; therefore, the mechanical properties (maximum stress, maximum strain, and elastic modulus) should be prioritized.
Dental restorative materials including amalgam, gold alloy, and dental resin have lower hardness values than enamel, which is important considering the wear of the opposing natural teeth. Gold alloy and dental resin have higher maximum stresses and maximum strains than dentin, amalgam has similar elastic modulus to dentin, and gold alloy has a higher elastic modulus than dentin, considering the rigidity to absorb the bite forces.
The results of this study suggest that gold alloy simultaneously satisfies the requirements of having a hardness value lower than that of enamel and mechanical properties similar to or higher than those of dentin. These results should help dentists to decide better clinical treatments, and they should contribute to the development of better dental restorative materials possessing suitable mechanical properties to replace dentin, with a hardness values to replace enamel, and having esthetically pleasing colors.
This study has some limitations especially including the aspect ratio of the specimen. Since the aspect ratio may change the stress–strain relationship in enamel, dentin, and dental restorative materials, further studies are needed.
Footnotes
Declaration of conflicting interests: The authors declare that there is no conflict of interest.
Funding: This research was supported by Korea Institute of Industrial Technology (KITECH), Republic of Korea.
References
- 1. Tillberg A, Järvholm B, Berglund A. Risks with dental materials. Dent Mater 2008; 24(7): 940–943 [DOI] [PubMed] [Google Scholar]
- 2. Vaderhobli RM. Advances in dental materials. Dent Clin North Am 2011; 55(3): 619–625 [DOI] [PubMed] [Google Scholar]
- 3. Koplin C, Jaeger R, Hahn P. A material model for internal stress of dental composites caused by the curing process. Dent Mater 2009; 25(3): 331–338 [DOI] [PubMed] [Google Scholar]
- 4. Jager ND, Kler MD, Zel JM. The influence of different core material on the FEA-determined stress distribution in dental crowns. Dent Mater 2006; 22(3): 234–242 [DOI] [PubMed] [Google Scholar]
- 5. Stober T, Lutz T, Gilde H, et al. Wear of resin denture teeth by two-body contact. Dent Mater 2006; 22(3): 243–249 [DOI] [PubMed] [Google Scholar]
- 6. Tara MA, Eschbach S, Wolfart S, et al. Zirconia ceramic inlay-retained fixed dental prostheses—first clinical results with a new design. J Dent 2011; 39(3): 208–211 [DOI] [PubMed] [Google Scholar]
- 7. Knorr SD, Combe EC, Wolff LF, et al. The surface free energy of dental gold-based materials. Dent Mater 2005; 21(3): 272–277 [DOI] [PubMed] [Google Scholar]
- 8. Gil FJ, Planell JA, Padrós A, et al. The effect of shot blasting and heat treatment on the fatigue behavior of titanium for dental implant applications. Dent Mater 2007; 23(4): 486–491 [DOI] [PubMed] [Google Scholar]
- 9. Arcís RW, López-Macipe A, Toledano M, et al. Mechanical properties of visible light-cured resins reinforced with hydroxyapatite for dental restoration. Dent Mater 2002; 18(1): 49–57 [DOI] [PubMed] [Google Scholar]
- 10. Bernstein RL, Preston CB, Lampasso J. Leveling the curve of Spee with a continuous archwire technique: a long term cephalometric study. Am J Orthod Dentofacial Orthop 2007; 131(6): 700–701 [DOI] [PubMed] [Google Scholar]
- 11. Ban S. Reliability and properties of core materials for all-ceramic dental restorations. Jpn Dent Sci Rev 2008; 44(1): 3–21 [Google Scholar]
- 12. Chen Y, Xu L, Liu Z, et al. Microstructures and properties of titanium alloys Ti-Mo for dental use. T Nonferr Metal Soc 2006; 16(2): s824–s828 [Google Scholar]
- 13. Chun KJ, Choi HH, Lee JY. Comparison of mechanical property and role between enamel and dentin in the human teeth. J Dent Biomech 2014; 5. DOI: 10.1177/1758736014520809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Davis JR. Metals handbook: properties and selection: nonferrous alloys and special-purpose materials. 10th ed. Materials Park, OH: ASM International, 1990 [Google Scholar]
- 15. VITA, VITA OMEGA 900 brochures, Vident, USA, http://vident.com [Google Scholar]
- 16. METALOR, Metalor dental(tm) Aurofluid2PF brochures, METALOR, USA, http://www.metalor.com [Google Scholar]
- 17. Posku LT, Placido E, Cardoso PEC. Influence of placement techniques on Vickers and Knoop hardness of class 2 composite resin restorations. Dent Mater 2004; 20(8): 726–732 [DOI] [PubMed] [Google Scholar]
- 18. Lava Technical Product Profile, 3M ESPE, USA, http://solutions.3m.com/wps/portal/3M/en_US/3M-ESPE-NA/dental-professionals/ [Google Scholar]
- 19. Boyer R, Welsch G, Collings EW. Materials properties handbook: titanium alloys. Materials Park, OH: ASM International, 1994 [Google Scholar]