

Abstract
Background
Generalized Anxiety Disorder (GAD) is a high prevalence, chronic disorder. Web-based interventions are acceptable, engaging, and can be delivered at scale. Few randomized controlled trials evaluate the effectiveness of prevention programs for anxiety, or the factors that improve effectiveness and engagement.
Objective
The intent of the study was to evaluate the effectiveness of a Web-based program in preventing GAD symptoms in young adults, and to determine the role of telephone and email reminders.
Methods
A 5-arm randomized controlled trial with 558 Internet users in the community, recruited via the Australian Electoral Roll, was conducted with 6- and 12-month follow-up. Five interventions were offered over a 10-week period. Group 1 (Active website) received a combined intervention of psycho-education, Internet-delivered Cognitive Behavioral Therapy (ICBT) for anxiety, physical activity promotion, and relaxation. Group 2 (Active website with telephone) received the identical Web program plus weekly telephone reminder calls. Group 3 (Active website with email) received the identical Web program plus weekly email reminders. Group 4 (Control) received a placebo website. Group 5 (Control with telephone) received the placebo website plus telephone calls. Main outcome measures were severity of anxiety symptoms as measured by the GAD 7-item scale (GAD-7) (at post-test, 6, and 12 months). Secondary measures were GAD caseness, measured by the Mini International Neuropsychiatric Interview (MINI) at 6 months, Centre for Epidemiologic Studies-Depression scale (CES-D), Anxiety Sensitivity Index (ASI), Penn State Worry Questionnaire (PSWQ), and Days out of Role.
Results
GAD-7 symptoms reduced over post-test, 6-month, and 12-month follow-up. There were no significant differences between Group 4 (Control) and Groups 1 (Active website), 2 (Active website with telephone), 3 (Active website with email), or 5 (Control with telephone) at any follow-up. A total of 16 cases of GAD were identified at 6 months, comprising 6.7% (11/165) from the Active groups (1, 2, 3) and 4.5% (5/110) from the Control groups (4, 5), a difference that was not significant. CES-D, ASI, and PSWQ scores were significantly lower for the active website with email reminders at post-test, relative to the control website condition.
Conclusions
Indicated prevention of GAD was not effective in reducing anxiety levels, measured by GAD-7. There were significant secondary effects for anxiety sensitivity, worry, and depression. Challenges for indicated prevention trials are discussed.
Trial Registration
International Standard Randomized Controlled Trial Number (ISRCTN): 76298775; http://www.controlled-trials.com/ISRCTN76298775 (Archived by WebCite at http://www.webcitation.org/6S9aB5MAq).
Keywords: anxiety disorders, prevention, early intervention, Internet, online systems, cognitive behavioral therapy
Introduction
Approximately 5% of the general population experiences General Anxiety Disorder (GAD) at least once in their lifetime [1], with population surveys indicating a lifetime prevalence rate of between 4.3-5.9% and a 12-month prevalence rate of between 1.2-1.9% [2,3]. The cost of GAD to the community is high as a result of its chronic course [4]. GAD frequently presents early in the lifespan and affects the individual throughout adulthood, with an estimated lag time to treatment of between 9 and 23 years [5]. If the prevalence of GAD is to be lowered, prevention, particularly focusing on the early adult and adolescence years when the illness emerges [6], will reduce the prevalence of mental disorder by up to 23% [7-9].
There is some evidence that GAD can be prevented. However, the conduct of research trials has not been optimal either because the researchers have been unable to exclude those with a diagnosis at the onset of the intervention or because the trials are too small or too short to investigate the number of incident cases following the intervention [10]. We reviewed the research literature, but found that only four trials excluded a diagnosis of GAD in adults at baseline. Two of the studies found preventative effects, but both trials had limitations [11,12]. Van’t Veer Tazelaar and colleagues [12] reported that depression and anxiety caseness could be halved in elderly people who were provided with a stepped care intervention of problem solving and cognitive behavioral therapy (CBT) bibliotherapy. However, the investigators did not report data separately for GAD, so the effect of the intervention on GAD compared to depression diagnosis could not be determined. Pitceathly and colleagues [13] reported a protective effect of a brief coping intervention on GAD in cancer patients. The effect was not detectable in the full sample, but was evident for those identified at the start of the trial with high risk of anxiety or depression. No preventative effects were found in the other two studies [14,15]. In the first, a stepped care intervention in elderly people living in residential care did not result in reduced incidence of combined anxiety or depression. In the second, carers of patients with Alzheimer’s disease did not show lower levels of anxiety or depression as a result of an intervention involving a Family Meetings intervention. In effect, no genuine prevention trials have been conducted with younger adults and none with adults without a cancer diagnosis.
A key challenge to delivering prevention interventions is the low level of engagement by those at risk; if symptoms are not disabling, motivation may be low and seeking help from doctors seen as inappropriate. Web-based interventions provide a potentially very useful delivery medium because they are accessible, acceptable, globally disseminable, and have been found to be effective in delivering CBT in clinical settings for both depression and anxiety [16-18]. Engagement may be enhanced by “push” factors (ie, factors that encourage involvement or engagement, such as reminders or coaching) [19]. However, inconsistent findings are reported [20-23]. Because prevention programs are delivered to large numbers at a population level, the costs associated with different push factors are critical to the feasibility of prevention efforts. Hence, there is a need to know the extent to which email reminders and telephone communication with the research team will improve adherence and effectiveness. The present study aimed to evaluate the effectiveness of a Web-based multimedia CBT intervention in individuals aged 18 to 30 years with symptoms of anxiety, who did not meet diagnostic criteria at baseline. The intervention was a website that provided psychoeducation, CBT, physical activity promotion, and relaxation training, with the majority of the sessions focusing on CBT. Each component of the intervention was found to be effective in GAD treatment [24-27]. Our rationale to include all four components was based on the view that combining a range of evidence-based interventions provides potential for maximal impact, as well as the opportunity for participants’ preferences (for example, see [28]). We know very little about engagement in prevention (compared to treatment) programs, and offering a range of interventions, all of which have evidence-based support from treatment settings, would potentially optimize effectiveness and uptake. We focused on young adults, as GAD develops during adolescence and early adulthood and any improvement would be likely to provide benefits over years. The intervention’s “e-couch” website is open following registration and the CBT “worry” program can be experienced.
Five interventions were offered over a 10-week period. Group 1 (Active website) received the combined intervention as described above. Group 2 (Active website with telephone) received the same Web program plus weekly telephone reminder calls. Group 3 (Active website with email) received the Web program plus automated weekly email reminders. Group 4 (Control) received a placebo website, matched in length to the active website. Group 5 (Control with telephone) received the placebo website plus telephone reminder calls. This design allowed us to compare the effectiveness of the active interventions to the control condition (1, 2, 3 vs 4) and also to determine the independent effect of phone contact in the control conditions (5 vs 4). Email reminders are less expensive than person-made telephone reminders, an important consideration for a prevention trial. To our knowledge, no similar prevention trials have been conducted with each of these inclusions: the use of an online intervention for GAD, targeting of young adults in the community, and excluding existing GAD diagnosis.
Methods
Study Design
A randomized controlled trial with 5 arms, called the “iChill” trial, with post-test, 6- and 12-month follow-up, was conducted. The study was approved by the ANU Human Ethics Committee (Protocol 2008/548).
Setting, Participants, and Eligibility Criteria
The study protocol [29] describes trial details. A screening questionnaire was emailed to 120,000 randomly chosen Australians aged 18-30 years registered on the Australian Electoral Roll. Individuals meeting inclusion criteria were invited to a Web portal where they provided consent and undertook screening and baseline surveys. They were then interviewed via telephone to determine current GAD diagnosis using the MINI International Neuropsychiatric Interview (MINI) [30] and randomized to the trial. Inclusion criteria were willingness to consent, an active email and phone number, English language proficiency, Internet access, and a score above 5 on the GAD-7 [31]. In order to specify the target population for whom the intervention might be effective, participants were excluded if they were currently undergoing CBT or seeing a psychologist or a psychiatrist, had a current or previous diagnosis of bipolar disorder, schizophrenia, or psychosis, were at risk of self-harm or suicide based on the MINI depression module, or had a current diagnosis of panic disorder, social phobia, or post-traumatic stress disorder (PTSD) on the MINI. Participants were not excluded if taking antidepressants or benzodiazepines. A total of 40 (7.2%, 40/558) were taking antidepressants and 8 (1.4%, 8/558) were taking benzodiazepines at baseline; 510 were not taking either antidepressants or benzodiazepines.
Randomization
The algorithm for randomization consisted of a stratified block design with eight strata (2 x 2 x 2) corresponding to gender, past GAD diagnosis, and severity of GAD symptoms with a block size of 10. “Past GAD diagnosis” was obtained from the MINI—a proportion of participants (24.2%, 135/558) met lifetime criteria for GAD on the MINI but did not meet MINI criteria for current GAD. To minimize imbalance between such participants, stratification was conducted on the basis of meeting lifetime GAD criteria (along with gender and current GAD symptoms). Allocation was administered via software architecture, and participants were informed of condition allocation after baseline interview.
Interventions
The Active website intervention was a 10-week structured version of the Anxiety and Worry modules of the “e-couch” program (ecouch.anu.edu.au), which consisted of an integrated program of psychoeducation (weeks 1-2), CBT (weeks 3-7), relaxation (weeks 8-9), and physical activity promotion (week 10). The psychoeducation section (Modules 1 and 2) provides information on worry, stress, fear, and anxiety; a description of anxious thinking; differentiation of GAD from other anxiety disorders; risk factors for GAD; comorbidity; and consequences of anxiety and available treatments. This section is based on interventions for mental health literacy that have succeeded in reducing symptoms of depression and anxiety, and improving mental health attitudes [32]. The CBT toolkits (Modules 3-7) addressed typical anxious thoughts and included sections on dealing with the purpose and meaning of worry, the act of worrying, and the content of worry. The information is derived from materials that have been found to reduce anxious cognitions in at-risk people [33,34]. Progressive muscle relaxation (PMR) (Module 8) instructs participants on how to progressively tense and relax different muscle groups to induce relaxation and help to identify tension early. PMR has been trialed in a previous website program for depression in adults [35] and adolescents [36]. The mindfulness meditation module (Module 9) helps participants become aware of their breathing and body, acknowledging thoughts and external distractions but remaining focused on the present. The final module, physical activity (Module 10), tailors advice about physical activity based on the stages of change theory [37]. The control website was an adapted version of the HealthWatch control condition developed for the Australian National University WellBeing study [38]. This website provided information about general health (nutrition, heart health, etc), and invited responses to questions about anxiety. Scripted telephone reminder calls in the Active plus telephone condition were made on a weekly basis to check on participants’ progress and to remind them to complete the module and/ or to keep completing the program. The phone reminders were intended to serve purely as reminders, had no therapeutic input, and were made by casual phone interviewers. Telephone calls were scripted and were based on the email scripts. Any technical issues were referred to the Trial Manager. Phone calls generally lasted between 30 seconds to 2 minutes. Phone calls were made regardless of whether the participant completed the program or not. Participants in the Active plus email and Control plus email conditions were sent a weekly reminder email. These were similar in content to the phone calls. There was no therapeutic input.
Outcome Measures
The primary outcome was the Generalized Anxiety Disorder 7-item scale (GAD-7) [31]. Secondary outcomes were GAD caseness based on MINI; worry, measured by the Penn State Worry Questionnaire (PSWQ) [39]; anxiety sensitivity, as measured by the Anxiety Sensitivity Index (ASI) [40]; depression symptoms, measured by the Centre for Epidemiologic Studies-Depression Scale (CES-D) [41]; and disability measured by Days out of Role from the US National Comorbidity Study [42]. GAD caseness was measured at 6 months. GAD caseness at 36 months will be determined by proxy using GAD-7 cut-off scores. Other measures not analyzed in this paper focused on comorbidities, such as harmful/hazardous alcohol use as measured by the Alcohol Use Disorders Identification Test (AUDIT) [43], or duplicate measures of depression caseness estimated by the Patient Health Questionnaire 9-item (PHQ-9) [44], and other behaviors such as help seeking and perceived need for treatment. Outcomes were assessed at baseline, 6, and 12 months, with the exception of MINI caseness, which was assessed at 6 months.
Sample Size
We aimed, conservatively, to find an effect of 0.3 between each Active website group and the Control, based on effect sizes of 0.6 found for previous treatment and indicated prevention trials (0.6) [33,34]. This assumes a pre-post correlation of .7 between scores. With 600 participants, we would have 80% power to detect effects, allowing for 15% attrition.
Statistical Analysis
Primary analyses were undertaken on an intent-to-treat basis (ITT). Mixed model repeated measures (MMRM) [45] were used to include all available data, including that from participants who subsequently withdrew from the trial. This approaches yields unbiased estimates of intervention effects under the assumption that data are missing at random (MAR). Unlike conventional approaches to analysis, MAR allows observations to be missing conditional on observed variables appearing in the analytic model [46]. Non-linear mixed models were used to analyze caseness.
Results
A total of 558 people were randomized to a trial condition of whom 360 (64.5%) completed post-test, 303 (54.3%) completed 6-month follow-up, and 264 (47.3%) completed the 12-month follow-up. Figure 1 shows the flow of participants. Sample characteristics are presented in Table 1. Although mean GAD-7 scores were above the cut-point of 5 at screening for all participants (mean 8.3, SD 3.3), anxiety symptoms had decreased by the time the baseline was completed (mean 6.7, SD 3.8).
Figure 1.
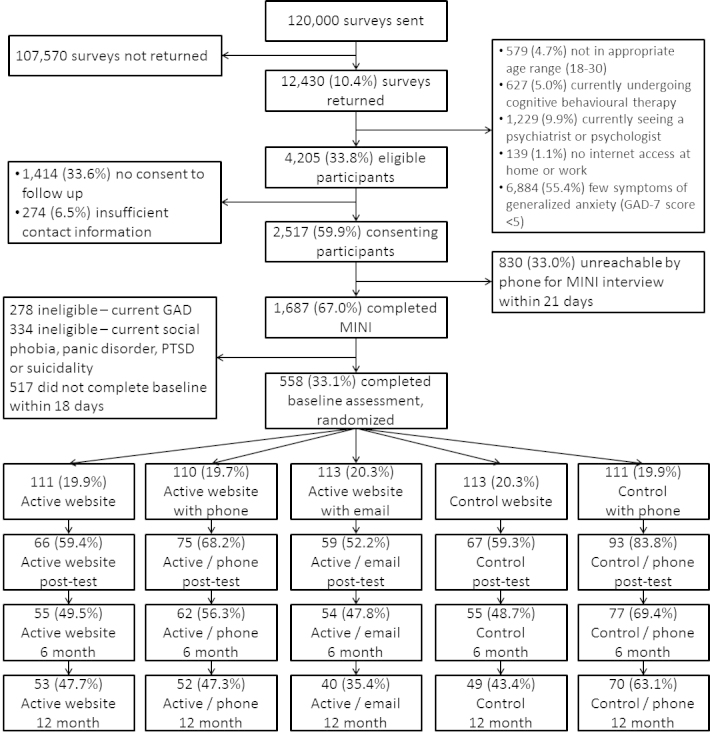
CONSORT diagram showing flow of participants through the study.
Table 1.
Characteristics of the sample at baseline by trial arm.
|
|
Active website (n=111) | Active website with email (n=113) | Active website with phone (n=110) | Control website (n=111) | Control website with phone (n=113) | F a or χ2 | P | |
| mean (SD) or n (%) |
|
|
||||||
| Characteristic | ||||||||
|
|
Age | 25.7 (3.2) | 25.4 (3.3) | 25.5 (3.1) | 26.0 (3.0) | 25.6 (3.5) | 0.623 | .646 |
|
|
GAD-7d score | 6.8 (3.9) | 6.2 (3.9) | 6.8 (3.6) | 6.9 (3.8) | 6.6 (3.7) | 0.604 | .660 |
|
|
CES-De score | 16.7 (10.1) | 17.7 (10.9) | 16.7 (9.8) | 18.8 (10.6) | 17.3 (8.8) | 0.802 | .524 |
|
|
Anxiety sensitivity | 19.3 (11.0) | 19.9 (11.5) | 17.5 (10.6) | 18.7 (9.9) | 18.8 (9.9) | 0.753 | .556 |
|
|
PSWQf | 40.5 (12.2) | 37.9 (12.5) | 39.5 (11.6) | 40.3 (12.0) | 39.2 (10.8) | 0.835 | .503 |
|
|
AUDITg score | 7.2 (5.1) | 7.2 (5.7) | 6.7 (4.8) | 6.9 (4.7) | 7.0 (5.3) | 0.189 | .944 |
|
|
DORh due to anxiety | 0.6 (1.5) | 0.9 (2.3) | 0.6 (1.6) | 0.6 (1.4) | 0.6 (1.2) | 0.859 | .488 |
|
|
Self-rated healthi | 2.4 (0.9) | 2.5 (0.8) | 2.4 (0.8) | 2.5 (0.9) | 2.5 (0.7) | 0.879 | .476 |
|
|
Childhood adversityj | 1.5 (1.4) | 1.9 (1.5) | 1.8 (1.6) | 1.7 (1.5) | 1.7 (1.5) | 0.919 | .452 |
|
|
Traumatic eventsk | 1.4 (1.5) | 1.6 (1.6) | 1.5 (1.5) | 1.4 (1.5) | 1.6 (1.6) | 0.498 | .737 |
|
|
Positive beliefs Internet therapyl | 5.6 (1.2) | 5.4 (1.3) | 5.4 (1.3) | 5.5 (1.3) | 5.8 (1.3) | 2.064 | .084 |
|
|
Female gender | 92 (82.9%) | 90 (79.6%) | 88 (80.0%) | 89 (80.2%) | 91 (80.5%) | 0.474b | .976 |
|
|
Completed university degree | 37 (33.3%) | 32 (28.6%) | 28 (25.9%) | 36 (32.4%) | 30 (26.8%) | 2.352b | .671 |
|
|
Prefer active conditionm | 67 (60.4%) | 51 (45.1%) | 70 (63.6%) | 60 (54.1%) | 70 (61.9%) | 10.501b | .033c |
| Employment status | 16.297b | .038c | ||||||
|
|
Full-time employment | 69 (62.2%) | 68 (61.3%) | 81 (75.7%) | 65 (59.1%) | 58 (51.8%) |
|
|
|
|
Part-time employment | 30 (27.0%) | 27 (24.3%) | 16 (15.0%) | 34 (30.9%) | 36 (32.1%) |
|
|
|
|
Not in labor force | 12 (10.8%) | 16 (14.4%) | 10 (9.3%) | 11 (10.0%) | 18 (16.1%) |
|
|
a F tests are from one-way analysis of variance (ANOVA) for continuous variables
b χ2 tests for categorical variables
c P<.05
dGAD: Generalized Anxiety Disorder
eCES-D: Center for Epidemiologic Studies Depression Scale
fPSWQ: Penn State Worry Questionnaire
gAUDIT: Alcohol Use Disorders Identification Test
hDOR: Days out of Role
iSelf-rated health assessed on a 5-point scale from 1 (excellent) to 5 (poor)
jChildhood adversity based on aggregate of 6 items assessing paternal/maternal mental health problems and substance use problems, high familial conflict, and parental separation/divorce
kTraumatic life events based on count from list of 14 traumatic events
lPositive beliefs in Internet therapy based on 2 items regarding confidence in learning skills about anxiety and better understanding anxiety using the Internet
mPreference for active condition based on a single item asking which intervention would be preferred
There were no differences on any of the baseline measures with the exception of “preference for active condition” and “employment status”. Across all conditions, the most preferred program was the Active website with email reminders (37.8%, 211/558), followed by the Control (31.4%, 175/558), with few participants stating a preference for telephone reminders (5.6%, 31/558 and 11.6%, 65/558, for Active and Control conditions, respectively). Lower preference for the Active website was found among those in the Control and Active with email conditions. Higher rates of full-time work were found among those receiving the Active website with telephone reminders and lower rates among those receiving the Control website with telephone reminders.
Adherence to the intervention differed significantly according to condition. Participants in the reminder conditions completed the majority of the 10 modules (Active/email: 5.5 modules, Active/telephone: 7.3, Control/telephone: 8.3) while those who did not receive reminders completed a little over one-third (3.7 modules for both active and control; F 4, 477.5=38.1, P<.001).
GAD-7 symptoms reduced at post-test and 6-month follow-up, but returned to baseline levels by 12 months. There were no significant differences between Group 4 (Control) and Groups 1 (Active website), 2 (Active website with telephone), 3 (Active website with email), or 5 (Control with telephone) at any follow-up. Outcomes were unchanged after adjusting for employment status and preferences for condition. Likewise, accounting for adherence by adjusting for module completion (ie, testing the efficacy of the intervention) did not change these outcomes. Figure 2 shows estimated marginal means of GAD-7 scores from the mixed model shown in Table 2.
Figure 2.
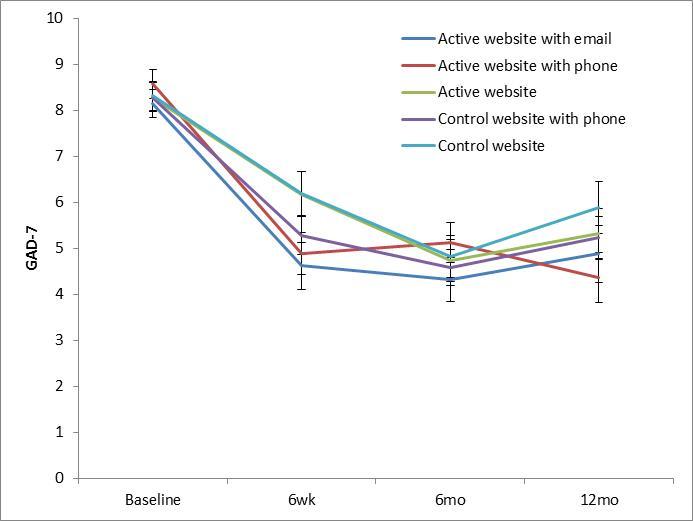
Outcome data on GAD-7 at post-test, 6-month and 12-month follow-ups (error bars represent standard error).
Table 2.
Repeated measures mixed model of GAD-7 scores at post-test, 6, and 12 months.
| Parameter | Estimate | Standard error | df | t / F | P | |
| Intercept |
|
6.946 | 0.359 | 553.0 | 19.3 | <.001 |
| Condition |
|
|
|
|
1.0 | .410 |
|
|
Active website | −0.117 | 0.508 | 553.0 | −0.2 | .818 |
|
|
Active website with email reminders | −0.716 | 0.506 | 553.0 | −1.4 | .158 |
|
|
Active website with phone reminders | −0.173 | 0.510 | 553.0 | −0.3 | .734 |
|
|
Control website with phone reminders | −0.335 | 0.506 | 553.0 | −0.7 | .508 |
|
|
Control website | 0.000 | 0.000 |
|
|
|
| Time | 29.5 | <.001 | ||||
|
|
Baseline | 0.000 | 0.000 |
|
|
|
|
|
Post-test | −1.066 | 0.494 | 389.2 | −2.2 | .032 |
|
|
6-month follow-up | −2.337 | 0.512 | 372.8 | −4.6 | <.001 |
|
|
12-month follow-up | −1.178 | 0.612 | 315.8 | −1.9 | .055 |
| Condition × time interaction | 0.8 | .622 | ||||
|
|
Active vs control at baseline | 0.000 | 0.000 |
|
|
|
|
|
Active vs control at post-test | 0.331 | 0.698 | 390.6 | 0.5 | .636 |
|
|
Active vs control at 6 months | 0.179 | 0.723 | 374.2 | 0.2 | .805 |
|
|
Active vs control at 12 months | −0.274 | 0.853 | 313.9 | −0.3 | .748 |
|
|
Active email vs control at baseline | 0.000 | 0.000 |
|
|
|
|
|
Active email vs control at post-test | −0.517 | 0.718 | 393.9 | −0.7 | .472 |
|
|
Active email vs control at 6 months | 0.370 | 0.730 | 372.3 | 0.5 | .612 |
|
|
Active email vs control at 12 months | −0.157 | 0.896 | 319.4 | −0.2 | .861 |
|
|
Active phone vs control at baseline | 0.000 | 0.000 |
|
|
|
|
|
Active phone vs control at post-test | −0.689 | 0.682 | 384.5 | −1.0 | .314 |
|
|
Active phone vs control at 6 months | 0.736 | 0.709 | 369.4 | 1.0 | .300 |
|
|
Active phone vs control at 12 months | −1.082 | 0.851 | 315.4 | −1.3 | .205 |
|
|
Control phone vs control at baseline | 0.000 | 0.000 |
|
|
|
|
|
Control phone vs control at post-test | −0.137 | 0.655 | 379.2 | −0.2 | .835 |
|
|
Control phone vs control at 6 months | 0.394 | 0.683 | 364.4 | 0.6 | .565 |
|
|
Control phone vs control at 12 months | −0.150 | 0.808 | 310.2 | −0.2 | .853 |
Data on secondary outcomes analyses are displayed for continuous variables in Table 3. Based on the MINI assessment at 6 months, 16 cases of GAD were identified, comprising 6.7% from the Active groups (1, 2, and 3) and 4.5% from the Control groups (4, 5). There was no significant difference in the number of cases across these collapsed groups.
Table 3.
Primary and secondary outcome data.
|
Outcome |
Active | Active / phone | Active / email | Control | Control / phone |
|
|||
| mean (SD)/n | mean (SD)/n | mean (SD)/n | mean (SD)/n | mean (SD)/n | F a | df | P | ||
| Sample size | |||||||||
|
|
Baseline | 111 | 110 | 113 | 111 | 113 |
|
|
|
|
|
Post-test | 66 | 75 | 58 | 66 | 93 |
|
|
|
|
|
6-month | 55 | 62 | 54 | 55 | 77 |
|
|
|
|
|
12-month | 53 | 52 | 40 | 48 | 70 |
|
|
|
| GAD-7 c | 0.8 | 12, 323.4 | .622 | ||||||
|
|
Baseline | 6.8 (3.9) | 6.8 (3.6) | 6.2 (3.9) | 7.0 (3.8) | 6.6 (3.7) |
|
|
|
|
|
Post-test | 6.1 (4.7) | 4.7 (3.6) | 4.6 (2.9) | 6.1 (4.1) | 5.3 (4.2) |
|
|
|
|
|
6-month | 4.3 (3.0) | 5.0 (4.0) | 4.3 (3.7) | 4.6 (3.6) | 4.7 (3.1) |
|
|
|
|
|
12-month | 5.1 (4.6) | 4.0 (3.4) | 5.1 (4.1) | 5.9 (4.5) | 5.1 (3.6) |
|
|
|
| PSWQ d | 1.0 | 12, 345.4 | .419 | ||||||
|
|
Baseline | 40.5 (12.2) | 39.5 (11.6) | 37.9 (12.5) | 40.3 (12.0) | 39.2 (10.8) |
|
|
|
|
|
Post-test | 39.0 (13.2) | 37.4 (10.6) | 33.8 (11.5) | 41.0 (12.3) | 38.4 (12.8) |
|
|
|
|
|
6-month | 33.9 (13.2) | 38.2 (11.3) | 35.9 (11.5) | 38.9 (13.4) | 37.9 (13.5) |
|
|
|
|
|
12-month | 34.1 (14.0) | 33.2 (11.2) | 34.4 (13.1) | 38.3 (13.9) | 37.2 (12.1) |
|
|
|
| ASI e | 1.7 | 12, 345.9 | .057 | ||||||
|
|
Baseline | 19.3 (11.0) | 17.5 (10.6) | 19.9 (11.5) | 18.7 (9.9) | 18.8 (9.9) |
|
|
|
|
|
Post-test | 18.9 (11.8) | 14.6 (10.6) | 17.1 (11.1) | 18.5 (12.2) | 16.7 (11.0) |
|
|
|
|
|
6-month | 16.0 (12.3) | 15.0 (11.5) | 15.4 (9.5) | 17.4 (10.2) | 15.1 (9.8) |
|
|
|
|
|
12-month | 19.5 (12.4) | 14.7 (10.0) | 19.4 (11.6) | 20.3 (11.1) | 21.1 (10.6) |
|
|
|
| CES-D f | 1.9 | 12, 328.4 | .036b | ||||||
|
|
Baseline | 16.7 (10.1) | 16.7 (9.8) | 17.7 (10.9) | 18.8 (10.6) | 17.3 (8.8) |
|
|
|
|
|
Post-test | 14.0 (10.8) | 12.4 (8.6) | 10.9 (8.4) | 17.5 (11.3) | 13.8 (9.6) |
|
|
|
|
|
6-month | 10.7 (7.7) | 12.6 (10.5) | 11.8 (8.9) | 14.4 (11.3) | 13.4 (8.1) |
|
|
|
|
|
12-month | 12.0 (9.2) | 9.7 (5.9) | 12.3 (11.3) | 15.3 (9.3) | 12.6 (8.7) |
|
|
|
| DOR g | 1.1 | 12, 369.9 | .324 | ||||||
|
|
Baseline | 0.6 (1.5) | 0.6 (1.6) | 0.9 (2.3) | 0.6 (1.4) | 0.6 (1.2) |
|
|
|
|
|
Post-test | 0.5 (1.3) | 0.2 (0.5) | 0.4 (0.9) | 0.5 (1.4) | 0.2 (0.8) |
|
|
|
|
|
6-month | 0.3 (1.4) | 0.4 (1.1) | 0.1 (0.6) | 0.5 (1.8) | 0.5 (2.5) |
|
|
|
|
|
12-month | 0.3 (0.8) | 0.2 (0.6) | 0.1 (0.5) | 0.7 (1.8) | 0.4 (1.9) |
|
|
|
astatistics are omnibus F tests from mixed models repeated measures for each outcome, based on time × condition interaction terms
b P<.05
cGAD: Generalized Anxiety Disorder
dPSWQ: Penn State Worry Questionnaire
eASI: Anxiety Sensitivity Index
fCES-D: Center for Epidemiologic Studies Depression scale
gDOR: days out of role due to anxiety
The mixed effect model repeated measure (MMRM) analyses for secondary outcomes were as follows. As for the primary outcome, there were no significant overall interactions between condition and time for CES-D, PSWQ, or Days out of Role. However, there was a significant interaction between condition and time for the ASI. Furthermore, there were significant effects of specific conditions at specific time points. CES-D, ASI, and PSWQ scores were significantly lower for the active website with email reminders at post-test, relative to the control website condition (t 389.2= −2.5, P=.015; t 368.7=−3.4, P<.001; t 371.9=−2.4, P=.017 respectively). The decrease in ASI scores for the active/email condition remained significant at 6 months (t 343.1=−2.3, P=.021). In addition, Days out of Role due to anxiety was significantly decreased at 12 months (but not at post-test or 6 months) for the active/email condition (t 398.3=−2.4, P=.016). There was also reduced worry in the active website with phone reminders at post-test and 6 months, relative to the control condition (t 368.6=−2.0, P=.047; t 340.2= −2.1, P=.035 respectively).
Discussion
Principal Findings
We found no evidence that a range of brief active interventions were associated with improved anxiety outcomes at post-test or at 6 or 12 months as measured by GAD-7 and by caseness at 6 months as measured by the MINI. We found that there were effects on secondary outcomes, most strongly found for anxiety sensitivity, where there was a significant interaction between condition and time for the ASI. In addition, ASI scores were significantly lower for the active website with email reminders at post-test, and at 6 months. There were also small effects at various follow-up intervals for the other measures mostly associated with the active website with email reminders. For instance, CES-D and PSWQ scores were significantly lower for the active website with email reminders at post-test, relative to the control website condition. In addition, Days out of Role due to anxiety was significantly decreased at 12 months for the active/email condition.
At best, these findings suggest that an active website with email may have small effects on a number of secondary outcomes. It is also possible that the GAD-7 may be a poorer measure of anxiety change than the ASI, and that genuine prevention effects operate, but were not discoverable because of our choice of outcome measure. The GAD-7 may be sensitive to a range of anxiety disorders [47] and may not have been the most robust outcome measure.
Limitations
In addition, a number of limitations to the present study need to be considered. There was differential dropout in a number of conditions relative to the control. Nevertheless, the completer analyses (not reported in the paper but undertaken) produced comparable effects to the main ITT analysis. The condition with the strongest secondary outcome effects was also the condition that was associated with the highest preference rating, suggesting that preference for it might have influenced the findings. In addition, the intervention itself may not have been optimal. We argued that combining a range of evidence-based interventions would provide maximal impact as well as provide opportunity for participants to make choices within the program content. It might be suggested that this diluted the effects of the individual components. However, we disagree, given that (1) the combined intervention is highly efficacious (effect sizes greater than 1.0) for patients with a diagnosis of GAD [48], (2) the multimedia intervention in the current paper was associated with effects on a range of secondary measures, and (3) evidence from earlier online trials indicates that much shorter interventions (eg, over 5 sessions rather than 8) are associated with positive outcomes, and that very short interventions can be effective [49]. Consequently, we doubt that the intervention website itself was the reason for the lack of effect on the primary outcome measure. Another criticism is that choosing a multi-modal treatment results in the findings not being clear-cut, as any component might be the effective one. However, we would argue that prevention trials, in direct comparison to treatment trials, are in their infancy. Trials that demonstrate the effectiveness of multi-component interventions represent the first stage of a prevention research program, where, once an effect can be demonstrated, further research would normally then investigate the effect of the subcomponents.
The number of individuals in the current prevention study developing a diagnosis over the 12-month period following the intervention was unexpectedly low. However, elsewhere, comparable rates of 8.6% for the intervention and 4.44% in usual care groups have been reported [14]. These low rates may be due to regression to the mean and to the low threshold of anxiety for recruitment to the trial. The 6-month interval to determine caseness is relatively short with respect to prevention trials in the sense that a longer interval permits more opportunity to develop a disorder and thus to judge the effectiveness of the interventions. The choice of the 6-month interval for the MINI was made in order to maximize follow-up numbers (ie, to determine caseness) as dropouts were expected to increase over the 12-month follow-up period. We reasoned that we could determine proxy measures of caseness at 12 months via the GAD-7. A planned 3-year follow-up using GAD-7 as the primary outcome has commenced and we will report anxiety and depression outcomes at this time. Attrition was higher than expected at about 35% at post-test, although similar rates of dropout have been reported for face-to-face CBT [50].
Consistent with previous eHealth trials, data completion was higher in the control condition and was lowest for the active website condition with automated emails—a finding consistent with earlier trials [35,51]). The lower attrition in the control groups has been attributed to participant burden. Whether online or face-to-face, psychological interventions can be hard work, even threatening, and are often associated with dropout [52]. We also had substantial loss to recruitment between an expression of interest to the trial, and enrollment following invitation to undertake baseline measures. The reasons for failure to take up enrollment are not clear, but the trial was configured to allow enrollment within a week of consent. Delays in telephone and email contact often stretched the recruitment process, although there were strict time limits on each of the processes involved. The multi-modal nature of recruitment made identification of the reasons for non-response very complex, as the screener was conducted by post, the MINI assessment by telephone call, and the baseline invitation by email to an online survey.
A related issue is the role of contact in promoting adherence. In the present trial, adherence to the website was increased by contact via email or telephone. However, increased contact does not always result in improved adherence. A study we undertook with crisis call centers showed that adherence was much lower in participants who were provided with a website and telephone support compared to individuals without such support [53]. More research is required to examine for whom and under what circumstances telephone contact can increase adherence, and the factors that lead to increased dropout. We have reviewed factors that predict adherence for online programs [54]. We also acknowledge that the effects of the intervention in an adolescent rather than a young adult sample might have been more evident, since GAD or worry might emerge in this period. Levels of attrition need to be considered, since these were high. In addition, the sample excluded concurrent other diagnoses such as social phobia and PTSD, reducing generalizability. The trial raises the important question of how best to keep symptomatic people engaged in interventions. One possibility is to change orientation toward healthy living and offer prevention for GAD by stealth. An alternative approach is to constrain participants from dropping out through structure (eg, curriculum activities in schools or induction programs in workforces). These possibilities are currently being pursued in other research projects.
Conclusions
Despite a number of limitations, the present trial represents a methodologically rigorous, well-executed prevention trial, which for the first time examines the effectiveness of the prevention of GAD in symptomatic 18-30 year olds in the community using online technologies. Diagnosis was established using a telephone interview at baseline and 6 months, and GAD diagnosis was an exclusion factor at commencement, ensuring that it was a genuine prevention trial. A post-hoc power analysis found that we had approximately 95% power to find a between-groups effect of d=0.3 between the Active website alone and Control website alone, indicating that the trial was sufficiently powered. Preference for trial condition was measured and assessed for its effect, and the study aimed to determine push and pull factors that might influence uptake and efficaciousness. In this trial, we were not able to demonstrate the preventative effects of the website on anxiety symptoms as measured by the GAD-7. There were indications that prevention was operating in one of the five conditions (email plus active website) on a number of the secondary measures. The 3-year follow-up will provide a stronger test of whether secondary outcomes such as anxiety sensitivity are modifiable in response to a website with email reminders and to determine whether anxiety symptoms and caseness are averted with a longer lapse of time.
Acknowledgments
The trial was funded by NHMRC Project Grant 525419. Helen Christensen is supported by NHMRC Fellowship 1056964. Philip Batterham is supported by NHMRC Fellowship 1035262. Kathleen Griffiths is supported by NHMRC Fellowship 1059620. Both Philip Batterham and Andrew Mackinnon had full access to the data in the study and had input into the final analyses. Philip Batterham takes full responsibility for the integrity of the data and the accuracy of the data analysis.
Abbreviations
- ASI
Anxiety Sensitivity Index
- AUDIT
Alcohol Use Disorders Identification Test
- CBT
Cognitive Behavioral Therapy
- CES-D
Centre for Epidemiologic Studies-Depression
- GAD
generalized anxiety disorder
- ITT
intent-to-treat
- MAR
missing at random
- MINI
Mini International Neuropsychiatric Interview
- PHQ-9
Patient Health Questionnaire 9-item
- PMR
progressive muscle relaxation
- PSWQ
Penn State Worry Questionnaire
Multimedia Appendix 1
CONSORT-EHEALTH checklist V1.6.2 [55].
Footnotes
Conflicts of Interest: Griffiths is the Director of Australian National University e-hub self-help services, which delivers the public access version of e-couch GAD and co-authored the GAD stream of e-couch; Bennett is the development manager of e-hub services. Neither derives a personal financial benefit from e-couch.
References
- 1.Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994 Jan;51(1):8–19. doi: 10.1001/archpsyc.1994.03950010008002. [DOI] [PubMed] [Google Scholar]
- 2.Judd LL, Kessler RC, Paulus MP, Zeller PV, Wittchen HU, Kunovac JL. Comorbidity as a fundamental feature of generalized anxiety disorders: results from the National Comorbidity Study (NCS) Acta Psychiatr Scand Suppl. 1998;393:6–11. doi: 10.1111/j.1600-0447.1998.tb05960.x. [DOI] [PubMed] [Google Scholar]
- 3.Tyrer P, Baldwin D. Generalised anxiety disorder. Lancet. 2006 Dec 16;368(9553):2156–66. doi: 10.1016/S0140-6736(06)69865-6. [DOI] [PubMed] [Google Scholar]
- 4.Greenberg PE, Sisitsky T, Kessler RC, Finkelstein SN, Berndt ER, Davidson JR, Ballenger JC, Fyer AJ. The economic burden of anxiety disorders in the 1990s. J Clin Psychiatry. 1999 Jul;60(7):427–35. doi: 10.4088/jcp.v60n0702. [DOI] [PubMed] [Google Scholar]
- 5.Feldner MT, Zvolensky MJ. Prevention of anxiety psychopathology: a critical review of the empirical literature. Clinical Psychology: Science and Practice. 2004;11(4):405–24. doi: 10.1093/clipsy.bph098. [DOI] [Google Scholar]
- 6.Patel V, Flisher AJ, Hetrick S, McGorry P. Mental health of young people: a global public-health challenge. Lancet. 2007 Apr 14;369(9569):1302–13. doi: 10.1016/S0140-6736(07)60368-7. [DOI] [PubMed] [Google Scholar]
- 7.Henderson M, Glozier N, Holland Elliott K. Long term sickness absence. BMJ. 2005 Apr 9;330(7495):802–3. doi: 10.1136/bmj.330.7495.802. http://europepmc.org/abstract/MED/15817531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kessler RC, Greenberg PE, Mickelson KD, Meneades LM, Wang PS. The effects of chronic medical conditions on work loss and work cutback. J Occup Environ Med. 2001 Mar;43(3):218–25. doi: 10.1097/00043764-200103000-00009. [DOI] [PubMed] [Google Scholar]
- 9.Andrews G, Issakidis C, Sanderson K, Corry J, Lapsley H. Utilising survey data to inform public policy: comparison of the cost-effectiveness of treatment of ten mental disorders. Br J Psychiatry. 2004 Jun;184:526–33. doi: 10.1192/bjp.184.6.526. http://bjp.rcpsych.org/cgi/pmidlookup?view=long&pmid=15172947. [DOI] [PubMed] [Google Scholar]
- 10.Institute of Medicine (US) Committee on Prevention of Mental Disorders . In: Reducing risks for mental disorders: Frontiers for preventive intervention research. Mrazek PJ, Haggerty RJ, editors. Washington, DC: National Academy Press; 1994. [PubMed] [Google Scholar]
- 11.van't Veer-Tazelaar PJ, van Marwijk HW, van Oppen P, van Hout HP, van der Horst HE, Cuijpers P, Smit F, Beekman At. Stepped-care prevention of anxiety and depression in late life: a randomized controlled trial. Arch Gen Psychiatry. 2009 Mar;66(3):297–304. doi: 10.1001/archgenpsychiatry.2008.555. [DOI] [PubMed] [Google Scholar]
- 12.van't Veer-Tazelaar PJ, van Marwijk HW, van Oppen P, van der Horst HE, Smit F, Cuijpers P, Beekman At. Prevention of late-life anxiety and depression has sustained effects over 24 months: a pragmatic randomized trial. Am J Geriatr Psychiatry. 2011 Mar;19(3):230–9. doi: 10.1097/jgp.0b013e3181faee4d. [DOI] [PubMed] [Google Scholar]
- 13.Pitceathly C, Maguire P, Fletcher I, Parle M, Tomenson B, Creed F. Can a brief psychological intervention prevent anxiety or depressive disorders in cancer patients? A randomised controlled trial. Ann Oncol. 2009 May;20(5):928–34. doi: 10.1093/annonc/mdn708. http://annonc.oxfordjournals.org/cgi/pmidlookup?view=long&pmid=19126633. [DOI] [PubMed] [Google Scholar]
- 14.Dozeman E, van Marwijk HW, van Schaik DJ, Smit F, Stek ML, van der Horst HE, Bohlmeijer ET, Beekman AT. Contradictory effects for prevention of depression and anxiety in residents in homes for the elderly: a pragmatic randomized controlled trial. Int Psychogeriatr. 2012 Aug;24(8):1242–51. doi: 10.1017/S1041610212000178. [DOI] [PubMed] [Google Scholar]
- 15.Joling KJ, van Marwijk HW, Smit F, van der Horst HE, Scheltens P, van de Ven PM, Mittelman MS, van Hout HP. Does a family meetings intervention prevent depression and anxiety in family caregivers of dementia patients? A randomized trial. PLoS One. 2012;7(1):e30936. doi: 10.1371/journal.pone.0030936. http://dx.plos.org/10.1371/journal.pone.0030936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Andrews G, Cuijpers P, Craske MG, McEvoy P, Titov N. Computer therapy for the anxiety and depressive disorders is effective, acceptable and practical health care: a meta-analysis. PLoS One. 2010;5(10):e13196. doi: 10.1371/journal.pone.0013196. http://dx.plos.org/10.1371/journal.pone.0013196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Christensen H, Griffiths KM, Farrer L. Adherence in internet interventions for anxiety and depression: systematic review. J Med Internet Res. 2009;11(2):e13. doi: 10.2196/jmir.1194. http://www.jmir.org/2009/2/e13/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Griffiths KM, Farrer L, Christensen H. The efficacy of internet interventions for depression and anxiety disorders: a review of randomised controlled trials. Med J Aust. 2010 Jun 7;192(11 Suppl):S4–11. doi: 10.5694/j.1326-5377.2010.tb03685.x. [DOI] [PubMed] [Google Scholar]
- 19.Chiu TM, Eysenbach G. Stages of use: consideration, initiation, utilization, and outcomes of an internet-mediated intervention. BMC Med Inform Decis Mak. 2010;10:73. doi: 10.1186/1472-6947-10-73. http://www.biomedcentral.com/1472-6947/10/73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Mohr DC, Duffecy J, Ho J, Kwasny M, Cai X, Burns MN, Begale M. A randomized controlled trial evaluating a manualized TeleCoaching protocol for improving adherence to a web-based intervention for the treatment of depression. PLoS One. 2013;8(8):e70086. doi: 10.1371/journal.pone.0070086. http://dx.plos.org/10.1371/journal.pone.0070086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Schneider F, de Vries H, Candel M, van de Kar A, van Osch L. Periodic email prompts to re-use an internet-delivered computer-tailored lifestyle program: influence of prompt content and timing. J Med Internet Res. 2013;15(1):e23. doi: 10.2196/jmir.2151. http://www.jmir.org/2013/1/e23/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Woodall WG, Buller DB, Saba L, Zimmerman D, Waters E, Hines JM, Cutter GR, Starling R. Effect of emailed messages on return use of a nutrition education website and subsequent changes in dietary behavior. J Med Internet Res. 2007;9(3):e27. doi: 10.2196/jmir.9.3.e27. http://www.jmir.org/2007/3/e27/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Farrer L, Christensen H, Griffiths KM, Mackinnon A. Internet-based CBT for depression with and without telephone tracking in a national helpline: randomised controlled trial. PLoS One. 2011;6(11):e28099. doi: 10.1371/journal.pone.0028099. http://dx.plos.org/10.1371/journal.pone.0028099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Linden M, Zubraegel D, Baer T, Franke U, Schlattmann P. Efficacy of cognitive behaviour therapy in generalized anxiety disorders. Results of a controlled clinical trial (Berlin CBT-GAD Study) Psychother Psychosom. 2005;74(1):36–42. doi: 10.1159/000082025. [DOI] [PubMed] [Google Scholar]
- 25.Jayakody K, Gunadasa S, Hosker C. Exercise for anxiety disorders: systematic review. Br J Sports Med. 2014 Feb;48(3):187–96. doi: 10.1136/bjsports-2012-091287. [DOI] [PubMed] [Google Scholar]
- 26.Herring MP, Jacob ML, Suveg C, Dishman RK, O'Connor PJ. Feasibility of exercise training for the short-term treatment of generalized anxiety disorder: a randomized controlled trial. Psychother Psychosom. 2012;81(1):21–8. doi: 10.1159/000327898. [DOI] [PubMed] [Google Scholar]
- 27.Borkovec TD, Costello E. Efficacy of applied relaxation and cognitive-behavioral therapy in the treatment of generalized anxiety disorder. J Consult Clin Psychol. 1993 Aug;61(4):611–9. doi: 10.1037//0022-006x.61.4.611. [DOI] [PubMed] [Google Scholar]
- 28.McHugh RK, Whitton SW, Peckham AD, Welge JA, Otto MW. Patient preference for psychological vs pharmacologic treatment of psychiatric disorders: a meta-analytic review. J Clin Psychiatry. 2013 Jun;74(6):595–602. doi: 10.4088/JCP.12r07757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Christensen H, Griffiths KM, Mackinnon AJ, Kalia K, Batterham PJ, Kenardy J, Eagleson C, Bennett K. Protocol for a randomised controlled trial investigating the effectiveness of an online e health application for the prevention of Generalised Anxiety Disorder. BMC Psychiatry. 2010;10:25. doi: 10.1186/1471-244X-10-25. http://www.biomedcentral.com/1471-244X/10/25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, Hergueta T, Baker R, Dunbar GC. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59 Suppl 20:22–33;quiz 34. [PubMed] [Google Scholar]
- 31.Spitzer RL, Kroenke K, Williams JB, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006 May 22;166(10):1092–7. doi: 10.1001/archinte.166.10.1092. [DOI] [PubMed] [Google Scholar]
- 32.McIntosh A, Cohen A, Turnbull N, Esmonde L, Dennis P, Eatock J. Clinical guidelines and evidence review for panic disorder and generalised anxiety disorder. Sheffield: University of Sheffield/London: National Collaborating Centre for Primary Care; 2004. [PubMed] [Google Scholar]
- 33.Kenardy J, McCafferty K, Rosa V. Internet-delivered indicated prevention for anxiety disorders: a randomized controlled trial. Behav Cognit Psychother. 2003;31(3):279–289. doi: 10.1017/S1352465803003047. [DOI] [Google Scholar]
- 34.Kenardy J, McCafferty K, Rosa V. Internet-delivered indicated prevention for anxiety disorders: six-month follow-up. Clinical Psychologist. 2006;10(1):39–42. doi: 10.1080/13284200500378746. [DOI] [Google Scholar]
- 35.Christensen H, Griffiths KM, Jorm AF. Delivering interventions for depression by using the internet: randomised controlled trial. BMJ. 2004 Jan 31;328(7434):265. doi: 10.1136/bmj.37945.566632.EE. http://europepmc.org/abstract/MED/14742346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Calear AL, Christensen H, Mackinnon A, Griffiths KM, O'Kearney R. The YouthMood Project: a cluster randomized controlled trial of an online cognitive behavioral program with adolescents. J Consult Clin Psychol. 2009 Dec;77(6):1021–32. doi: 10.1037/a0017391. [DOI] [PubMed] [Google Scholar]
- 37.Prochaska JO, DiClemente CC. Stages and processes of self-change of smoking: toward an integrative model of change. J Consult Clin Psychol. 1983 Jun;51(3):390–5. doi: 10.1037//0022-006x.51.3.390. [DOI] [PubMed] [Google Scholar]
- 38.Griffiths KM, Crisp D, Christensen H, Mackinnon AJ, Bennett K. The ANU WellBeing study: a protocol for a quasi-factorial randomised controlled trial of the effectiveness of an Internet support group and an automated Internet intervention for depression. BMC Psychiatry. 2010;10:20. doi: 10.1186/1471-244X-10-20. http://www.biomedcentral.com/1471-244X/10/20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Fresco DM, Mennin DS, Heimberg RG, Turk CL. Using the Penn State Worry Questionnaire to identify individuals with generalized anxiety disorder: a receiver operating characteristic analysis. J Behav Ther Exp Psychiatry. 2003;34(3-4):283–91. doi: 10.1016/j.jbtep.2003.09.001. [DOI] [PubMed] [Google Scholar]
- 40.Peterson R, Reiss R. Anxiety Sensitivity Index Manual (2nd ed.) Worthington, OH: IDS Publishing Corporation; 1992. [Google Scholar]
- 41.Radloff LS. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological Measurement. 1977 Jun 01;1(3):385–401. doi: 10.1177/014662167700100306. [DOI] [Google Scholar]
- 42.Kessler RC, Berglund P, Demler O, Jin R, Koretz D, Merikangas KR, Rush AJ, Walters EE, Wang PS, National Comorbidity Survey Replication The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R) JAMA. 2003 Jun 18;289(23):3095–105. doi: 10.1001/jama.289.23.3095. [DOI] [PubMed] [Google Scholar]
- 43.Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption--II. Addiction. 1993 Jun;88(6):791–804. doi: 10.1111/j.1360-0443.1993.tb02093.x. [DOI] [PubMed] [Google Scholar]
- 44.Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001 Sep;16(9):606–13. doi: 10.1046/j.1525-1497.2001.016009606.x. http://europepmc.org/abstract/MED/11556941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Verbeke G, Molenberghs G. Linear mixed models for longitudinal data. New York: Springer; 2000. [Google Scholar]
- 46.Rubin DB. Multiple imputation for nonresponse in surveys. New York: Wiley; 1987. [Google Scholar]
- 47.Kroenke K, Spitzer RL, Williams JB, Monahan PO, Löwe B. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med. 2007 Mar 6;146(5):317–25. doi: 10.7326/0003-4819-146-5-200703060-00004. [DOI] [PubMed] [Google Scholar]
- 48.Christensen H, Mackinnon A, Batterham P, O'Dea B, Guastella AJ, Griffiths KM, Eagleson C, Kalia Hehir K, Kenardy J, Bennett K, Hickie IB. The effectiveness of an online e-health application compared to attention placebo or sertraline in the treatment of generalised anxiety disorder. J Med Internet Res. 2014:In Press. doi: 10.1186/1745-6215-11-48. (forthcoming) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Christensen H, Griffiths KM, Mackinnon AJ, Brittliffe K. Online randomized controlled trial of brief and full cognitive behaviour therapy for depression. Psychol Med. 2006 Dec;36(12):1737–46. doi: 10.1017/S0033291706008695. [DOI] [PubMed] [Google Scholar]
- 50.Cuijpers P, Donker T, van Straten A, Li J, Andersson G. Is guided self-help as effective as face-to-face psychotherapy for depression and anxiety disorders? A systematic review and meta-analysis of comparative outcome studies. Psychol Med. 2010 Dec;40(12):1943–57. doi: 10.1017/S0033291710000772. [DOI] [PubMed] [Google Scholar]
- 51.Donker T, Bennett K, Bennett A, Mackinnon A, van Straten A, Cuijpers P, Christensen H, Griffiths KM. Internet-delivered interpersonal psychotherapy versus internet-delivered cognitive behavioral therapy for adults with depressive symptoms: randomized controlled noninferiority trial. J Med Internet Res. 2013;15(5):e82. doi: 10.2196/jmir.2307. http://www.jmir.org/2013/5/e82/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Bados A, Balaguer G, Saldaña C. The efficacy of cognitive-behavioral therapy and the problem of drop-out. J Clin Psychol. 2007 Jun;63(6):585–92. doi: 10.1002/jclp.20368. [DOI] [PubMed] [Google Scholar]
- 53.Christensen H, Farrer L, Batterham PJ, Mackinnon A, Griffiths KM, Donker T. The effect of a web-based depression intervention on suicide ideation: secondary outcome from a randomised controlled trial in a helpline. BMJ Open. 2013;3(6):e002886. doi: 10.1136/bmjopen-2013-002886. http://bmjopen.bmj.com/cgi/pmidlookup?view=long&pmid=23811172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Christensen H, Griffiths KM, Farrer L. Adherence in internet interventions for anxiety and depression. J Med Internet Res. 2009;11(2):e13. doi: 10.2196/jmir.1194. http://www.jmir.org/2009/2/e13/ [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Eysenbach G, CONSORT-EHEALTH Group CONSORT-EHEALTH: improving and standardizing evaluation reports of Web-based and mobile health interventions. J Med Internet Res. 2011;13(4):e126. doi: 10.2196/jmir.1923. http://www.jmir.org/2011/4/e126/ [DOI] [PMC free article] [PubMed] [Google Scholar]