

Abstract
Objective:
This investigation examined the concurrent validity of a new video simulation assessing adolescent alcohol and marijuana decision making in peer contexts (A-SIDE).
Method:
One hundred eleven youth (60% female; age 14–19 years; 80% White, 12.6% Latino; 24% recruited from treatment centers) completed the A-SIDE simulation, self-report measures of alcohol and marijuana use and disorder symptoms, and measures of alcohol (i.e., drinking motives and expectancies) and marijuana (i.e., expectancies) cognitions in the laboratory.
Results:
Study findings support concurrent associations between behavioral willingness to use alcohol and marijuana on the simulation and current use variables as well as on drinking motives and marijuana expectancies. Relations with use variables were found even when sample characteristics were controlled. Interestingly, willingness to accept nonalcoholic beverages (e.g., soda) and food offers in the simulation were inversely related to recent alcohol and marijuana use behavior.
Conclusions:
These findings are consistent with prior work using laboratory simulations with college students and provide preliminary validity evidence for this procedure. Future work is needed to examine the predictive utility of the A-SIDE with larger and more diverse samples of youth.
Given normative developmental shifts from familial to peer influences across adolescence, peer contexts have often been the focus of alcohol and other drug (AOD) decision-making research. The mechanisms by which peers influence their friends’ decisions to use substances remain poorly understood and require assessment techniques sensitive to social contexts in decision-making processes. Traditional approaches have focused on retrospective self-reports of situational features associated with use, such as group size, constellation, and location (Anderson and Parent, 2007). Although methods are available for use with emerging adults and adults to examine situational and contextual influences on drinking, both in situ (Clapp et al., 2007) and in the laboratory (e.g., Larsen et al., 2012), researchers studying younger adolescents are limited by unique ethical and legal issues surrounding observation of youth engaging in substance use.
Laboratory-based procedures have been developed to examine how context can influence youth decision making about alcohol without direct exposure to this agent. Teunissen and colleagues (2012) experimentally manipulated peer feedback in a simulated chat room to examine the effects of peer status on boys’ (ages 14–15 years) behavioral willingness (BW) to drink alcohol in a response to a series of written vignettes. Youth BW ratings were influenced by both peer pro- and anti-alcohol norms, particularly those of high-status peers. Cameron et al. (2011) developed innovative drinking game procedures, using water, to examine social/contextual influences on alcohol consumption including the gender composition of groups and type of drinking game in college. Willingness to drink alcohol by incoming college students, assessed via audio simulation of social drinking contexts (C-SIDE), was concurrently associated with alcohol expectancies and drinking motives and predicted average alcohol consumption and hazardous drinking at the end of students’ first year of college (Anderson et al., 2013). These contextually specific simulation paradigms allow examination of social contextual influences on alcohol use in the laboratory with a greater level of ecological validity than previously available.
In this article, we describe the validation of a video simulation of peer AOD contexts focusing on alcohol and marijuana for use with a broad range of adolescents within the community (A-SIDE). We examined whether decision making on the simulation varied as a function of demographic characteristics and alcohol-related cognitions (i.e., expectancies and motives). We anticipated that adolescent BW on the A-SIDE would be related to current AOD use patterns, such that alcohol or marijuana BW during the simulation would be related to greater self-reported quantity and/or frequency of use. We expected alcohol BW to relate to greater positive and fewer negative alcohol expectancies as well as higher levels of enhancement and social motives. For marijuana, we focused on positive and negative marijuana expectations and anticipated a similar pattern of results as those stated above for alcohol.
Method
Participants
Youth ages 14–19 years who reported more than 10 use episodes within their lifetime (inclusive of alcohol or marijuana) and did not meet criteria for current psychosis, social anxiety disorder, or eating disorders by the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-Kid; Sheehan et al., 2010) were invited to participate. Data presented here are from 111 teens (60% female; 80% White, 12.6% Latino; 24% recruited from treatment centers; 99.1% lifetime alcohol use; 89.0% lifetime marijuana use). Eighty-five youth completed study measures in two assessment sessions spaced approximately 3 weeks apart, whereas 26 completed assessments in a single-session investigation on cue reactivity (Quackenbush and Anderson, 2011). These samples differed such that youth in the single administration, compared with those whose sessions were spaced 3 weeks apart, were somewhat older (Mage = 16.8 vs. 16.3 years), t(109) = 2.23, p = .03; used marijuana more frequently (lifetime users: M = 13.71, SD = 12.92 vs. M = 6.25, SD = 11.03), t(90) = 2.72, p = .008; reported more marijuana use disorder symptoms (lifetime users: M = 2.75, SD = 1.92, vs. M = 0.45, SD = 0.75), t(25.33 [unequal variances; Satterthwaite’s df]) = 5.73, p < .0001; and greater BW for marijuana on the A-SIDE (M = 1.77, SD = 1.28, vs. M = 0.64, SD = 1.00), t(109) = 4.74, p < .0001. Institutional review boards at each recruitment site approved study procedures.
Measures
The MINI-Kid is designed to screen youth for diagnoses from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV; American Psychiatric Association, 1994). Single-item questions on demographics, lifetime and recent alcohol and marijuana use, and treatment exposure were also administered at screening.
The Structured Clinical Interview (Brown et al., 1994) queried experiences with substance use, mental health services, and related variables. The Customary Drinking and Drug Use Record, Lifetime Version (Brown et al., 1998) structured interview provided information about AOD use including the average (M = 4.93, SD = 5.66) and maximum quantity (M = 7.97, SD = 8.43) of alcoholic drinks consumed per episode for an average month over the past 3 months; days using per month over past 3 months (alcohol: M = 4.09, SD = 5.74; marijuana: M = 7.46, SD = 11.67), and the number of AOD-related problems experienced by youth (alcohol use disorder symptoms; M = 1.24, SD = 1.71; drug use disorder symptoms: M = 0.91, SD = 1.45) and has been validated for use with adolescents (Brown et al., 1994). Given their distribution, AOD problems were dichotomized for analysis (0 = none, 1 = 1 or more).
The 28-item Modified Drinking Motives Questionnaire (Grant et al., 2007) indexes reasons to drink alcohol due to social (α = .69), enhancement (α = .92), coping-anxiety (α = .58), coping-depression (α = .81), and conformity considerations (α = .85) on a 1 (almost never) to 4 (almost always) scale and was successfully used in an undergraduate sample (Mage = 19.7, SD = 3.3; Grant et al., 2007). Because of systematic errors in administration, 16 youth did not receive this questionnaire; available data were used in the analyses.
The 100-item Alcohol Expectancy Questionnaire for Adolescents (AEQ-A; Brown et al., 1987) was completed by youth in the multisession sample, and they were asked about perceived outcomes of alcohol use including global positive changes (α = .84), improved cognitive-behavioral performance (α = .77), sexual enhancement (α = .77), cognitive-behavioral impairment (α = .87), increased arousal (α = .77), and relaxation and tension-reduction expectancies (α = .85; all alphas in this sample), rated from 1 (disagree strongly) to 5 (agree strongly).
The Marijuana Effect Expectancy Questionnaire (Aarons et al., 2001), completed by all participants, assessed outcome expectations for using marijuana, including cognitive-behavioral impairment (α = .87), relaxation–tension reduction (α = .87), sexual facilitation (α = .72), perceptual-cognitive enhancement (α = .71), global negative expectancies (α = .73), and craving/physical effects (α = .76). Items were rated on a 1 (disagree strongly) to 5 (agree strongly) scale.
Procedures
Recruitment.
Participants were recruited from public schools, youth groups, and substance use treatment centers in the Pacific Northwest. Phone screenings were conducted after obtaining parental consent and youth assent, with written consent and assent obtained before laboratory procedures. Gift cards were provided for participation.
A-SIDE procedure.
Interviewers taught participants the procedure using training vignettes and then presented them with the following social context:
You arrive at a friend’s house in late afternoon/early evening. There are a few other people there hanging out. Imagine that these people are your friends, you are in the room, the camera view is your eyes. Your friends are going to ask you to join in with what they are doing. Role-play what you would think, say, or do in this situation. Remember, there are no right or wrong answers.
Twelve social scenes were presented in random order via laptop, featuring four adolescent characters (two male, two female), three types of social grouping (alone, mixed-gender, and same-gender dyads), and two types of offers (alcohol or marijuana, soda or food). AOD (alcohol or marijuana) and control (soda or food) offer scenes were paired such that each youth experienced a balance of offers in the same location in the home with the same actors. Each scene was approximately 20 seconds in length. After each presentation, youth completed an open-ended elicitation of thoughts and feelings within each scene. After the youth viewed and responded to all of the scenes, a gender-matched interviewer briefly presented a reminder image of each offer and guided the participant through a structured interview assessing social information processing and decision making within the scene (Dodge and Price, 1994). Youth self-reported willingness to accept (scored 0/1) each offer of alcohol, marijuana, nonalcoholic beverage, or food (Would you accept the offer of … ?). Ratings were summed within offer type (i.e., alcohol, marijuana, nonalcoholic beverages, food), resulting in four scores ranging from 0 to 3. See Anderson and Parent (2007) for details on the production of the A-SIDE.
Results
Overall, youth were more likely to accept offers of nonalcoholic (M = 2.14, SD = 1.14) than alcoholic beverages (M = 1.22, SD = 0.11), t(110) = -6.47, p < .0001. Food offers (M = 2.10, SD = 0.09) were accepted more often than marijuana (M = 0.90, SD = 0.11), t(110) = -7.43, p < .0001. Demographic characteristics (age, sex, race, Latino status) and treatment history were unrelated to A-SIDE BW ratings. Alcohol and marijuana BW were positively correlated (r = .31, p = .0008), as were food and nonalcoholic beverage BW (r = .52, p < .0001).
At the bivariate level, alcohol BW was positively related to enhancement (r = .26, p = .01) and coping-anxiety motives (r = .35, p = .0005), with a trend for social drinking motives (r = .20, p = .06). BW was not associated with alcohol expectancies. Marijuana BW was positively associated with relaxation (r = .26, p = .007) and sexual facilitation expectancies for marijuana use (r = .23, p = .02), and inversely related to expectations that marijuana use leads to cognitive-behavioral impairments (r = -.40, p < .0001) and global negative outcomes (r = -.38, p < .0001).
Regression analyses (Stata Version 13.0; StataCorp LP, College Station, TX) examined the relationships between A-SIDE BW ratings and current AOD patterns including relevant covariates (i.e., sex, administration type, treatment history). As alcohol BW was not related to frequency of alcohol consumed (r = .03, n.s.) or alcohol use disorder symptoms (r = .09, n.s.) at the bivariate level, regressions were not conducted for those outcomes. Using negative binomial regression, greater alcohol BW was associated with greater average alcohol consumption (B = 0.28, SE = 0.07, p < .0001), when accounting for sex (B = 0.48, SE = 0.19, p = .01), and treatment history (B = 0.70, SE = 0.21, p = .001), χ2(4) = 29.14, p = .0002. BW for nonalcoholic beverages was not statistically significant in this model (B = -0.13, SE = 0.08, n.s.).
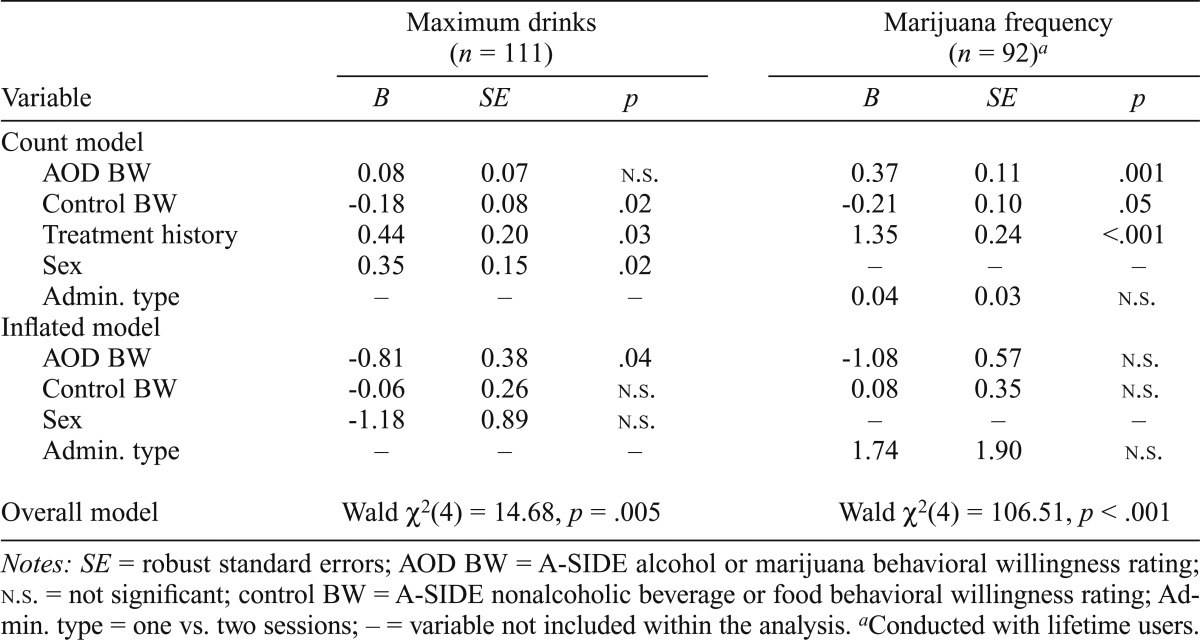
Table 1 presents the results of the zero-inflated models for maximum drink per occasion (negative binomial regression) and days using marijuana per month (Poisson regression). In the count portion of the models (i.e., prediction of the intensity of consumption), accepting more marijuana use offers was related to increased frequency of recent marijuana consumption, but accepting more alcohol offers did not reach significance for maximum drinks per episode. Interestingly, accepting nonalcoholic beverage and food offers were associated with lower maximum consumption per drinking episode and lower frequency of marijuana use, respectively. The zero-inflated nature of the distributions (i.e., likelihood of being a nonuser) was associated with fewer acceptances of alcohol on the A-SIDE and evidenced a nonsignificant trend (p = .06) for fewer marijuana use offers.
Table 1.
Prediction of 30-day drinking patterns (past 3 months)
| Maximum drinks (n = 111) |
Marijuana frequency (n = 92)a |
|||||
| Variable | B | SE | p | B | SE | p |
| Count model | ||||||
| AOD BW | 0.08 | 0.07 | n.s. | 0.37 | 0.11 | .001 |
| Control BW | -0.18 | 0.08 | .02 | -0.21 | 0.10 | .05 |
| Treatment history | 0.44 | 0.20 | .03 | 1.35 | 0.24 | <.001 |
| Sex | 0.35 | 0.15 | .02 | – | – | – |
| Admin. type | – | – | – | 0.04 | 0.03 | n.s. |
| Inflated model | ||||||
| AOD BW | -0.81 | 0.38 | .04 | -1.08 | 0.57 | n.s. |
| Control BW | -0.06 | 0.26 | n.s. | 0.08 | 0.35 | n.s. |
| Sex | -1.18 | 0.89 | n.s. | – | – | – |
| Admin. type | – | – | – | 1.74 | 1.90 | n.s. |
| Overall model | Wald χ2(4) = 14.68, p = .005 | Wald χ2(4) = 106.51, p < .001 | ||||
Notes: SE = robust standard errors; AOD BW = A-SIDE alcohol or marijuana behavioral willingness rating; n.s. = not significant; control BW = A-SIDE nonalcoholic beverage or food behavioral willingness rating; Admin, type = one vs. two sessions; – = variable not included within the analysis.
Conducted with lifetime users.
Although the overall model was significant, reporting drug use disorder symptoms was not related to BW for marijuana offers when accounting for sampling characteristics, χ2(4) = 22.47, p = .0002, with the overall effect being driven by treatment history (B = 1.92, SE = 0.21, p = .001) and administration type (B = -1.39, SE = 0.59, p = .02).
Discussion
This investigation provided preliminary support for the use of the A-SIDE as a laboratory-based measure of teens’ AOD decision making. BW to drink alcohol in the simulations was associated with the quantity of alcohol consumed, whereas marijuana BW was associated with frequency of consumption. Accepting AOD offers on the A-SIDE was associated with common cognitive predictors of alcohol and marijuana use, drinking motives, and marijuana expectancies. The associations found for drinking motives complement work conducted with college students using the C-SIDE audio simulation. The lack of association between alcohol expectancies and BW on the A-SIDE is inconsistent with our previous work with college students (Anderson et al., 2013). It is unclear why simulation performance for alcohol differed for the A-SIDE and C-SIDE; however, these investigations used different alcohol expectancy measures (AEQ-A vs. AEMax; Goldman and Darkes, 2004). As we did not include measures of marijuana motives in this investigation, the relative impact of motives and expectancies for each substance offer type is unknown. Future research should include balanced measurement of these cognitions for both alcohol and marijuana to better elucidate these relations.
A number of findings with this adolescent sample were consistent with work using the C-SIDE audio simulation with entering college students (Anderson et al., 2013). First, we replicated the preference for nonalcoholic beverages and food offers over AOD offers within the scenes. These findings suggest that although some youth will opt for AOD use at times, social contexts seemingly facilitate acceptances of food and nonalcoholic beverages. Cultural patterns around accepting consumables from hosts may facilitate these behaviors in social contexts. Although nonalcoholic beverage and food offers were originally designed to function as a control for undifferentiated positive or negative responding in the simulations, we found that nonalcoholic beverage acceptances were associated with a lower quantity of drinking, as was found with the C-SIDE. For marijuana, increased willingness to accept food offers was related to less frequent marijuana use. Because these offers are not mutually exclusive during the simulation, it is unclear whether accepting nonalcoholic beverages or food represents behavioral substitution, as accepting these offers is correlated on the simulation. For alcohol, we hypothesized that consuming nonalcoholic beverages and food on the C-SIDE might represent using the prevention strategy of stomach loading or already having a beverage in hand to diffuse later offers of alcohol (Anderson et al., 2013). How this mechanism might work for marijuana use frequency, when marijuana use is associated with increased food consumption (Foltin et al., 1998), is unclear.
This investigation suggests that simulation procedures may have merit as laboratory-based measures of AOD decision making. Similar to other researchers within the area (e.g., Teunissen et al., 2012), we relied on BW ratings to serve as a proxy for AOD use and were able to conduct concurrent validation of BW with the A-SIDE. Prospective work with the C-SIDE suggests that this type of simulation may be able to uniquely predict AOD use and problems later on (Anderson et al., 2013); however, similar longitudinal tests are necessary here. Our use of two different administration strategies is a limitation of this work. Further, some of our measures evidenced low reliability (i.e., coping-anxiety and social drinking motives). Future work must examine the validity of the A-SIDE to predict use outcomes across time in larger, more diverse samples of youth.
Acknowledgments
We thank the participating schools and treatment centers as well as Sara Parent, Carly Kennedy, Cody Packard, Jennifer Go, John Frederick, and Joanna Robinson for their work on this project. We also thank Stephanie Wormington and Katia Duncan for their comments on early drafts of this manuscript.
Footnotes
This research was funded by National Institute on Drug Abuse Grant R21 019960 (to Kristen G. Anderson) and a Reed College Summer Research Award (to Mathias Quackenbush).
References
- Aarons GA, Brown SA, Stice E, Coe MT. Psychometric evaluation of the marijuana and stimulant effect expectancy questionnaires for adolescents. Addictive Behaviors. 2001;26:219–236. doi: 10.1016/s0306-4603(00)00103-9. [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: Author; 1994. [Google Scholar]
- Anderson KG, Duncan K, Buras M, Packard CD, Kennedy C. C-SIDE: Drinking simulation for college students. Journal of Studies on Alcohol and Drugs. 2013;74:94–103. doi: 10.15288/jsad.2013.74.94. [DOI] [PubMed] [Google Scholar]
- Anderson KG, Parent SJ. Adolescent decision-making about substance use: A video-based assessment. In: Galwye VN, editor. Progress in Educational Psychology Research. New York, NY: Nova Science Publishers; 2007. pp. 3–21. Reprinted in (2008) Psychology of Decision-Making (P. M. Garrison, Ed.). New York: Nova Publishers. [Google Scholar]
- Brown SA, Christiansen BA, Goldman MS. The Alcohol Expectancy Questionnaire: An instrument for the assessment of adolescent and adult alcohol expectancies. Journal of Studies on Alcohol. 1987;48:483–491. doi: 10.15288/jsa.1987.48.483. [DOI] [PubMed] [Google Scholar]
- Brown SA, Myers MG, Lippke L, Tapert SF, Stewart DG, Vik PW. Psychometric evaluation of the Customary Drinking and Drug Use Record (CDDR): A measure of adolescent alcohol and drug involvement. Journal of Studies on Alcohol. 1998;59:427–438. doi: 10.15288/jsa.1998.59.427. [DOI] [PubMed] [Google Scholar]
- Brown SA, Myers MG, Mott MA, Vik PW. Correlates of success following treatment for adolescent substance abuse. Applied & Preventive Psychology. 1994;3:61–73. [Google Scholar]
- Cameron JM, Leon MR, Correia CJ. Extension of the simulated drinking game procedure to multiple drinking games. Experimental and Clinical Psychopharmacology. 2011;19:295–302. doi: 10.1037/a0024312. [DOI] [PubMed] [Google Scholar]
- Clapp JD, Holmes MR, Reed MB, Shillington AM, Freisthler B, Lange JE. Measuring college students’ alcohol consumption in natural drinking environments: Field methodologies for bars and parties. Evaluation Review. 2007;31:469–489. doi: 10.1177/0193841X07303582. [DOI] [PubMed] [Google Scholar]
- Dodge KA, Price JM. On the relation between social information processing and socially competent behavior in early school-aged children. Child Development. 1994;65:1385–1397. doi: 10.1111/j.1467-8624.1994.tb00823.x. [DOI] [PubMed] [Google Scholar]
- Foltin RW, Fischman MW, Byrne MF. Effects of smoked marijuana on food intake and body weight of humans living in a residential laboratory. Appetite. 1988;11:1–14. doi: 10.1016/s0195-6663(88)80017-5. [DOI] [PubMed] [Google Scholar]
- Goldman MS, Darkes J. Alcohol expectancy multiaxial assessment: A memory network-based approach. Psychological Assessment. 2004;16:4–15. doi: 10.1037/1040-3590.16.1.4. [DOI] [PubMed] [Google Scholar]
- Grant VV, Stewart SH, O’Connor RM, Blackwell E, Conrod PJ. Psychometric evaluation of the five-factor Modified Drinking Motives Questionnaire–Revised in undergraduates. Addictive Behaviors. 2007;32:2611–2632. doi: 10.1016/j.addbeh.2007.07.004. [DOI] [PubMed] [Google Scholar]
- Larsen H, Engels RC, Wiers RW, Granic I, Spijkerman R. Implicit and explicit alcohol cognitions and observed alcohol consumption: Three studies in (semi)naturalistic drinking settings. Addiction. 2012;107:1420–1428. doi: 10.1111/j.1360-0443.2012.03805.x. [DOI] [PubMed] [Google Scholar]
- Quackenbush M, Anderson KG. Attentional bias to alcohol and marijuana cues: Eye tracking and adolescent decision making [Abstract 0860] Alcoholism: Clinical and Experimental Research. 2011;35(Supplement s1):225A. [Google Scholar]
- Sheehan DV, Sheehan KH, Shytle RD, Janavs J, Bannon Y, Rogers JE, Wilkinson B. Reliability and validity of the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI-KID) Journal of Clinical Psychiatry. 2010;71:313–326. doi: 10.4088/JCP.09m05305whi. [DOI] [PubMed] [Google Scholar]
- Teunissen HA, Spijkerman R, Prinstein MJ, Cohen GL, Engels RC, Scholte RH. Adolescents’ conformity to their peers’ pro-alcohol and anti-alcohol norms: The power of popularity. Alcoholism: Clinical and Experimental Research. 2012;36:1257–1267. doi: 10.1111/j.1530-0277.2011.01728.x. [DOI] [PMC free article] [PubMed] [Google Scholar]