

Abstract
Objective:
Web-based personalized feedback interventions, particularly personalized normative feedback (PNF), are efficacious in improving college drinking outcomes; however, no personalized feedback interventions to date have provided college drinkers with feedback about their own decisional balance. This study tested the relative efficacy of a novel decisional balance feedback (DBF) intervention, PNF, and an assessment-only control condition.
Method:
Participants (N = 724; 56% female) were undergraduate students at a 4-year university in the U.S. Pacific Northwest and were randomized to receive one-time exposure to web-based DBF, PNF, or assessment only. Web-based assessment occurred at baseline and at 1-, 6-, and 12-month follow-ups and included measures of motivation to change, drinking quantity norms, drinking frequency/quantity, and alcohol-related problems.
Results:
At the 1-month follow-up, DBF and PNF participants reported reductions in alcohol-related problems; however, only PNF participants reduced their drinking frequency and quantity. At the 6-month follow-up, only DBF participants showed significant reductions in drinking quantity and alcohol-related problems. Neither group maintained reductions in alcohol use or alcohol-related problems at the 12-month follow-up.
Conclusions:
This study provided preliminary evidence that web-based DBF and PNF are efficacious interventions for college drinkers, with DBF having somewhat longer lasting effects.
According to the 2011 Monitoring the Future National Survey, 36% of college students reported consuming five or more drinks in a row in the past month, and 40% reported having “gotten drunk” (Johnston et al., 2012). In addition, up to 20% of young adults are estimated to have an alcohol use disorder (Blanco et al., 2008). Negative consequences associated with such heavy drinking affect college drinkers themselves (e.g., accidental injury, sexual assault, driving while intoxicated; Hingson et al., 2009) as well as their peers and communities (e.g., sleep disruption; noise complaints; property damage; verbal, physical, or sexual violence; Langley et al., 2003; Wechsler and Nelson, 2008). The continued and pressing severity of college drinking has inspired ongoing efforts to develop and disseminate accessible, time-efficient, and cost-effective interventions tailored to the needs of this population (DeJong et al., 2009; Goldman et al., 2002).
Personalized feedback interventions
Although various interventions have been developed for and tested with college drinkers, the most common interventions incorporate personalized feedback on students’ alcohol use (Carey et al., 2007, 2012; Cronce and Larimer, 2011). Originally, personalized feedback was offered in the context of multicomponent, in-person, brief motivational interventions, which also included alcohol assessment, advice giving, decisional balance exercises, alcohol didactics, and discussion of protective behavioral strategies (e.g., interventions based on the Brief Alcohol Screening and Intervention for College Students [BASICS] model; Dimeff et al., 1999). Personalized feedback, however, is increasingly used as a stand-alone intervention delivered via mail, computer, and Internet (Walters and Neighbors, 2005). Although findings suggest weaker effects for web-based versus in-person personalized feedback interventions (Carey et al., 2012; Wagener et al., 2012), systematic reviews document that web-based personalized feedback is effective in its own right (Carey et al., 2007, 2009, 2012; Cronce and Larimer, 2011; Riper et al., 2009; Walters and Neighbors, 2005). The web-based modality also requires relatively fewer resources than in-person interventions, potentially increasing cost-effectiveness and intervention reach (Carey et al., 2009). Last, ready access to alcohol interventions via the web may help engage more individuals who are concerned about privacy or who are more familiar with web and mobile technologies (Carey et al., 2009).
Personalized feedback interventions can comprise various components, including drinking summaries; didactic information about alcohol use, risk factors, and alcohol expectancies; and protective behavioral strategies (Walters and Neighbors, 2005). Personalized normative feedback (PNF) is, however, the most commonly included component in these interventions. Based on social learning theory (Bandura, 1977), PNF is designed to reduce overestimated descriptive normative perceptions and often includes information on (a) one’s own drinking behavior, (b) one’s perceptions of others’ drinking behavior, and (c) others’ actual drinking behavior. Together, this information highlights discrepancies between one’s own drinking behavior and perceived norms, known as self–other discrepancy (Borsari and Carey, 2003), as well as between normative perceptions and actual norms, and one’s own drinking and actual norms. As a stand-alone intervention, PNF has been associated with decreases in perceived drinking norms, alcohol use, and alcohol-related problems (Cronce and Larimer, 2011).
Decisional balance feedback as a novel web-based intervention
As noted above, decisional balance has been included in multicomponent, in-person, brief motivational interventions (e.g., Carey et al., 2006; Monti et al., 2007). It has also been used as a stand-alone, in-person intervention (Collins and Carey, 2005; LaBrie et al., 2006) and as a measure of motivation to change (Collins et al., 2009; Cunningham et al., 1997; King and DiClemente, 1993; Migneault et al., 1999). Rooted in decision-making theory (Janis and Mann, 1977), decisional balance entails an evaluation of perceived advantages and disadvantages of engaging in a certain behavior and its alternatives, and it has been identified as one aspect of the multidimensional motivation-to-change construct (Miller, 1999). Decisional balance exercises have been designed to reduce decision-making errors by making people more cognizant of the factors contributing to their decisions (Janis and Mann, 1977). Further, this exercise gives people an opportunity to articulate ambivalence about their current behavior and to determine if the weight of evidence is accumulating toward the need for behavior change (Miller, 1999). In this way, the decisional balance may help individuals develop and resolve intrapersonal discrepancy (Miller, 1999), such as actual-ideal discrepancy, the distance between one’s current behavior and one’s perceived ideal behavior/outcome, and actual-ought discrepancy, the distance between current behavior and personally acceptable, morally sanctioned behavior (Higgins, 1987; McNally et al., 2005).
Despite promising findings for other health-related behaviors (e.g., Colten and Janis, 1982; LaBrie et al., 2008), there are few studies that have tested decisional balance as a stand-alone intervention, and evidence for its efficacy in decreasing college drinking is mixed. One study indicated that heavy episodic drinking among college men decreased in the month after they were exposed to a decisional balance exercise regarding their drinking (LaBrie et al., 2006). Another study evaluated the efficacy of both written and in-person decisional balance exercises as stand-alone interventions and did not find an effect for either decisional balance exercise compared with an assessment-only control group (Collins and Carey, 2005). Last, Carey et al. (2006) attempted to enhance the strength and longevity of a brief motivational intervention by adding a decisional balance component. Findings indicated that participants receiving the enhanced intervention decreased their drinking over the 12-month follow-up compared with their assessment-only counterparts; however, the addition of the decisional balance exercise did not significantly augment this effect.
All of these studies have focused on the practice of completing a decisional balance exercise (i.e., generating perceived advantages and disadvantages of drinking vs. changing drinking behavior). No studies to date, however, have provided feedback based on student-generated decisional balance data. Considering the positive findings for web-based personalized feedback interventions in the literature (Carey et al., 2007; Cronce and Larimer, 2011; Riper et al., 2009; Walters and Neighbors, 2005), decisional balance feedback (DBF) may be a novel variant of such interventions by providing students with a summary of their motivation to change (e.g., overall balance toward change, summary of perceived advantages/disadvantages, and the weight of their importance and likelihood).
DBF is well positioned to support drinking reductions among college students. The decisional balance has long been used as a tool in motivational interventions (Miller, 1999; Miller and Rollnick, 2012) and is considered a core process in moving through the stages of change as proposed in the transtheoretical model (DiClemente, 1993; Prochaska, 1994; Prochaska et al., 1994). Further, among individuals with substance use disorders, the development of discrepancy is related to better outcomes, and the decisional balance exercise has been the key therapeutic technique associated with such positive outcomes (Apodaca and Longabaugh, 2009). DBF may thereby complement the existing set of efficacious personalized feedback interventions because, in contrast to the self–other discrepancy developed by PNF (Borsari and Carey, 2003), DBF could facilitate the development and resolution of actual-ideal or actual-ought discrepancy regarding alcohol use consequences (Higgins, 1987; McNally et al., 2005).
Present study
This study’s aims were to develop and test the initial efficacy of a novel personalized feedback intervention, DBF, relative to an assessment-only control condition and PNF, a personalized feedback intervention of known efficacy. We hypothesized that both DBF and PNF interventions would reduce alcohol quantity, frequency, and problems compared with an assessment-only control condition. We focused on these outcomes because both interventions aimed to motivate participants to moderate alcohol use (i.e., quantity and frequency) with an overall goal of reducing alcohol-related problems.
Method
Participants
Participants were 724 (56% female) undergraduate students at a 4-year university in the U.S. Pacific Northwest. Individuals qualified if they were at least 18 years of age and reported at least one heavy drinking episode (i.e., four or more drinks for women and five or more drinks for men; Wechsler et al., 1995) in the past 30 days. See Figure 1 for the participant flowchart. Before recruitment, study procedures were reviewed and approved by the institutional review board at the home institution, and informed consent was obtained.
Figure 1.

Study flowchart. PNF = personalized normative feedback; HDE = heavy drinking episode.
The mean age of the sample was 20.78 (SD = 1.42) years; 7.2% were freshmen, 14.2% were sophomores, 23.7% were juniors, 51.7% were seniors, and 3.2% described their class standing as other. In this sample, 67.1% self-identified as White/European American, 17.8% as Asian, 9.6% as multiracial, 1% as Black/African American, 0.7% as Native Hawaiian/Pacific Islander, and 0.6% as American Indian/Alaska Native; 3.3% endorsed the “other” racial group. Further, 6.5% indicated Hispanic/Latino ethnicity. Of the overall sample, 26.9% reported being members of the fraternity/sorority system.
Measures
Single items assessing age, gender, class standing, race, ethnicity, and membership in an on-campus fraternity/sorority organization were used to describe the sample and compare groups at baseline.
Measures used to generate drinking outcome variables.
The Frequency–Quantity (F-Q) questionnaire (adapted from Borsari and Carey, 2000; Collins et al., 2002; Dimeff et al., 1999) comprises single items assessing drinking consumption patterns (e.g., “Think of the occasion you drank the most in the last month. How much alcohol did you drink?” “How many days in the last month did you consume alcohol?”). This measure was used to assess whether participants experienced at least one heavy drinking episode in the past 30 days, which served as the primary inclusion criterion, as well as drinking frequency, which served as an outcome variable. Typical and peak drinking quantity and hours items were used to create estimated blood alcohol levels for the PNF intervention (see the Web-based personalized feedback interventions section below).
The Timeline Followback (TLFB; Sobell and Sobell, 1992) consists of monthly calendars that allow for retrospective evaluation of drinking behavior for each day of the previous month(s). Concordance tests have indicated that the TLFB and prospective daily self-monitoring correlate up to r = .89 for 30-day drinking (Carney et al., 1998). The TLFB was used to aggregate the 30-day drinking quantity outcome variable.
The Rutgers Alcohol Problem Index (White and Labouvie, 1989) consists of 23 items assessing alcohol-related consequences. Sample items include, “Not able to do your homework or study for a test” and “Wanted to stop drinking but couldn’t.” Respondents indicate on a Likert-type scale how many times in the past 30 days they experienced each problem listed (i.e., 0 = 0 times, 1 = 1–2 times, 2 = 3–5 times, 3 = 6–10 times, 4 = more than 10 times). Internal consistency for this measure was adequate (α = .88). The summary score was used to represent the alcohol-related problems outcome variable.
Measures used to generate personalized feedback intervention content.
The Modified Daily Drinking Questionnaire (modified for this study from BASICS; Collins et al., 2002; Dimeff et al., 1999) includes a grid assessing alcohol consumption on each day of a typical drinking week during the past 30 days. Adequate 1-week test–retest correlations have been calculated for estimates of a typical drinking week (r = .93; Miller et al., 2002). Weekly drinking quantity scores were created by summing the number of standard drinks (one standard drink is equal to 12 oz. beer, 5 oz. wine, or 1.5 oz. distilled spirits) reported over a typical week. These scores were used in the PNF intervention as a comparison with perceived and actual norms.
The Drinking Norms Rating Form (adapted from Baer et al., 1991) asks participants to report perceived daily alcohol use of average U.S. and local college students of like gender over the course of a typical week. It has shown adequate concurrent validity and test–retest reliability in prior studies (Marlatt et al., 1998; Neighbors et al., 2006). In this study, internal consistency was adequate (α = .76 and .74, respectively). The perceived norm for weekly drinking quantity was the sum of the number of standard drinks participants believed same-gender students at their university had consumed. This measure was used in the construction of the PNF to highlight discrepancies between participants’ perceptions of drinking norms and actual drinking norms.
Using an open-ended decisional balance worksheet (Collins et al., 2009), participants were asked to think about their current pattern of drinking and record the advantages and disadvantages of “continuing to drink as you are now” and “reducing your drinking in some way you feel comfortable with.” Responses were capped at 16 for each of the four categories. That said, no participants approached 16 responses, which allays concerns about potential data truncation. Next, participants were asked to report on the likelihood and importance of each of the named advantages and disadvantages on a 7-point, Likert-type scale.
The counts of the pros and cons listed in the four fields of this open-ended questionnaire formed the decisional balance proportion, which may be written as the following:
 |
where subscripts red = reducing drinking and cur = current drinking. Decisional balance proportion scores at 0.5 represent an even balance between pros and cons of reducing drinking and current drinking. Scores between 0.5 and 1.0 indicate a balance tipped toward reducing drinking, and scores between 0.0 and 0.5 indicate a balance tipped toward maintaining current drinking.
A prior study indicated the adequate convergent and discriminant validity for the decisional balance proportion (Collins et al., 2009). The following pieces of data from the decisional balance worksheet were used in the DBF intervention (for further information about the DBF intervention used in this study, please contact the corresponding author): (a) the decisional balance proportion, (b) perceived advantages and disadvantages regarding current drinking/reducing drinking (see qualitative analysis of decisional balance content in Collins et al., in press), and (c) participants’ ratings of the likelihood and importance of each named advantage and disadvantage.
Participant satisfaction.
The Post-Intervention Measure included 13 participant satisfaction items (e.g., “I thought this exercise was interesting”) rated on a 7-point Likert-type scale (1 = strongly disagree and 7 = strongly agree). This measure was administered immediately following delivery of the PNF and DBF interventions.
Web-based personalized feedback interventions
Decisional balance feedback.
Participants received personalized feedback on their perceived advantages and disadvantages of their current drinking based on their self-report responses to the baseline decisional balance worksheet. This feedback included (a) a graphic representation of the decisional balance proportion, (b) graphic and textual representations of the quantitative total, (c) qualitative content of advantages and disadvantages of current drinking and reducing drinking, and (d) likelihood and importance of each advantage and disadvantage. For more information about the DBF intervention used in this study, please contact the corresponding author.
Personalized normative feedback.
The PNF was based on the normative feedback component of the BASICS intervention (Dimeff et al., 1999) and was adapted from Collins et al. (2002) for online use. The PNF presented participants with personalized information designed to reduce overestimated normative perceptions about drinking in one’s peer group. The PNF consisted of four main feedback elements: (a) typical weekly quantity compared with perceived and actual same-gender peer norms, (b) typical and peak estimated BAL compared with same-gender peer norms, (c) calories consumed from alcohol in a typical week compared with same-gender peer norms, and (d) money spent on alcohol during a typical week compared with same-gender peer norms. For more information about the PNF intervention used in this study, please contact the corresponding author.
Procedure
A random sample (N = 2,425) of undergraduate students from the university registrar’s list was invited to participate. On a rolling basis from April 2011 through February 2012, potential participants for the current study were emailed study invitations, which included the study URL and a randomly generated identification number needed to log into the secure study website. Interested individuals logged into the study website, read information about the study procedures and their rights as participants, and provided electronic informed consent. Next, participants completed the baseline questionnaires, which took approximately 30 minutes.
Individuals who qualified for study participation (i.e., were at least 18 years of age and reported at least one heavy drinking episode in the past 30 days) were immediately and automatically randomized using blocked randomization to one of the three study conditions. Control participants were shown a screen that thanked them for their time and reminded them that they would be contacted for the 1-month follow-up. Participants randomized to the DBF and PNF conditions were seamlessly linked to their corresponding intervention content and, afterward, the Post-Intervention Measure to provide satisfaction feedback. They were then thanked for their participation and reminded that they would be contacted for the 1-month follow-up. After their submission of the survey, all participants were mailed a thank you letter containing a $20 check for completing the questionnaires and a reminder about their next assessment.
One, 6, and 12 months after the baseline questionnaires were completed, participants were contacted via email and prompted to revisit the website to complete the same questionnaires they completed at baseline. As necessary, participants were reminded via email, telephone, and postal mail to revisit the study website. Following completion of each online questionnaire session, participants were mailed $20 checks. Over the course of the study, participants could be compensated up to a total of $80 in participant payments. Participants who provided complete data for all assessments were entered into a drawing to receive one of four $250 cash prizes. Follow-ups were completed on a rolling basis throughout the study and were concluded in March 2013.
Data analysis plan
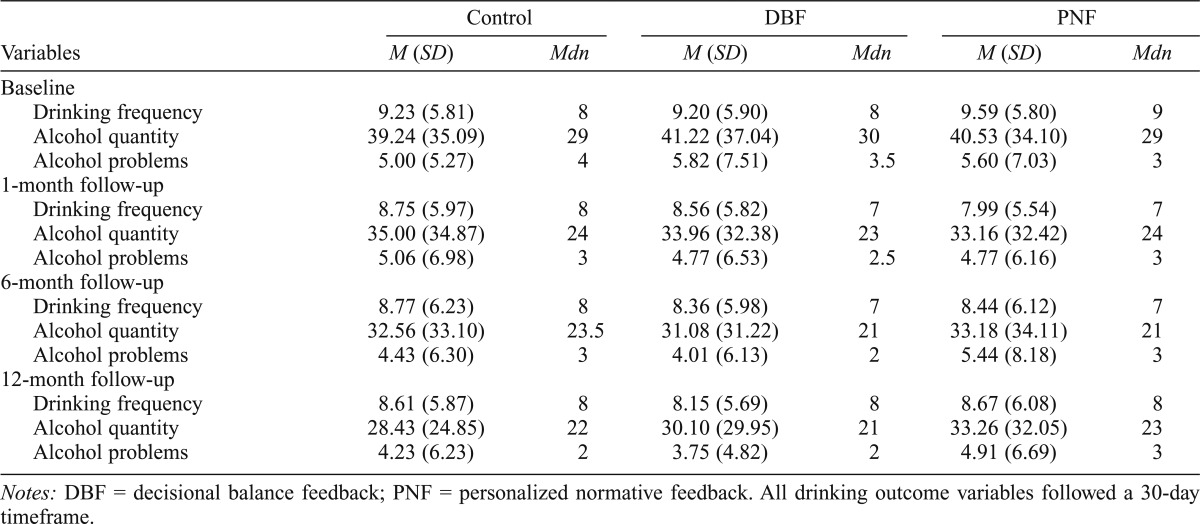
Descriptive analyses were conducted using SPSS Version 19 (IBM Corp., Armonk, NY) to describe the sample as well as to determine the distribution shapes of the outcome variables and the presence of outliers. Because primary alcohol outcomes were determined to be positively skewed, overdispersed counts (see Table 1 for descriptive statistics), we used nonparametric tests as well as negative binomial or zero-inflated negative binomial (ZINB) regressions for preliminary and primary analyses involving alcohol outcomes (Neal and Simons, 2007). Specifically, nonparametric tests (i.e., Kruskal–Wallis) and Pearson chi-square tests were used to examine baseline ineligible/included and intervention group differences as well as associations between data “missingness” (Allison, 2001, p. 3) and predictors of the primary models (i.e., tests of the intervention on drinking variables). In primary analyses, negative binomial or ZINB models were used to test the effects of the interventions on drinking outcomes (Cameron and Trivedi, 1998).
Table 1.
Descriptive statistics for drinking variables by intervention group and timepoint
| Variables | Control |
DBF |
PNF |
|||
| M (SD) | Mdn | M (SD) | Mdn | M (SD) | Mdn | |
| Baseline | ||||||
| Drinking frequency | 9.23 (5.81) | 8 | 9.20 (5.90) | 8 | 9.59 (5.80) | 9 |
| Alcohol quantity | 39.24 (35.09) | 29 | 41.22 (37.04) | 30 | 40.53 (34.10) | 29 |
| Alcohol problems | 5.00 (5.27) | 4 | 5.82 (7.51) | 3.5 | 5.60 (7.03) | 3 |
| 1-month follow-up | ||||||
| Drinking frequency | 8.75 (5.97) | 8 | 8.56 (5.82) | 7 | 7.99 (5.54) | 7 |
| Alcohol quantity | 35.00 (34.87) | 24 | 33.96 (32.38) | 23 | 33.16 (32.42) | 24 |
| Alcohol problems | 5.06 (6.98) | 3 | 4.77 (6.53) | 2.5 | 4.77 (6.16) | 3 |
| 6-month follow-up | ||||||
| Drinking frequency | 8.77 (6.23) | 8 | 8.36 (5.98) | 7 | 8.44 (6.12) | 7 |
| Alcohol quantity | 32.56 (33.10) | 23.5 | 31.08 (31.22) | 21 | 33.18 (34.11) | 21 |
| Alcohol problems | 4.43 (6.30) | 3 | 4.01 (6.13) | 2 | 5.44 (8.18) | 3 |
| 12-month follow-up | ||||||
| Drinking frequency | 8.61 (5.87) | 8 | 8.15 (5.69) | 8 | 8.67 (6.08) | 8 |
| Alcohol quantity | 28.43 (24.85) | 22 | 30.10 (29.95) | 21 | 33.26 (32.05) | 23 |
| Alcohol problems | 4.23 (6.23) | 2 | 3.75 (4.82) | 2 | 4.91 (6.69) | 3 |
Notes: DBF = decisional balance feedback; PNF = personalized normative feedback. All drinking outcome variables followed a 30-day timeframe.
ZINB represents a subset of generalized linear models for count outcomes that are positively skewed and have more zero responses than would be expected, given the negative binomial distribution. ZINB regressions model two processes: (a) a Bernoulli trial, which determines the probability that an observation is a “certain” or consistent zero that does not belong to the negative binomial distribution, and (b) a negative binomial regression, if the observation is a feasible count response predicted by the negative binomial distribution (Hardin and Hilbe, 2007). For the purpose of these analyses, we reported the statistics for both processes but focused on the interpretation of the negative binomial portion of the ZINB models. The resulting effect sizes are reported as incident rate ratios (IRRs), where IRRs < 1 indicate an inverse association, IRRs = 1 indicate no association, and IRRs > 1 indicate a positive association.
Results
Preliminary analyses
Ineligible students (Mage = 20.40 years, SD = 1.72) were significantly younger than included students (Mage = 20.78 years, SD = 1.42), z = -4.87, p < .001. Relatedly, greater proportions of upperclassmen were included (35% of freshmen, 55% of sophomores, 54% of juniors, 63% of seniors, and 64% of other class standing) versus not included, χ2(4, n = 1,285) = 40.69, p < .001. Inclusion status covaried with race, with 35% of Black/African American, 37% of Asian, 40% of American Indian/Alaska Native, 50% of Native Hawaiian/Pacific Islander, 57% of other, 65% of multiracial, and 65% of White/European American students included, χ2(6, n = 1,277) = 82.88, p < .001. Inclusion status also covaried with fraternity/sorority status, with 85% of fraternity/sorority versus 50% of non–fraternity/sorority students included, χ2(1, n = 1,285) = 92.12, p < .001. Gender and ethnicity were not associated with inclusion (ps > .34).
Kruskal–Wallis and Pearson chi-square tests determined if random group assignment was successful. The three groups did not differ significantly on baseline demographic (i.e., age, gender, class standing, race, ethnicity, and membership in an on-campus fraternity/sorority organization) or drinking outcome variables (ps > .16; see Table 1 for descriptive statistics).
Website tracking confirmed that 88% of participants assigned to the PNF and DBF groups were exposed to the intervention (Figure 1). A Pearson chi-square test indicated that intervention exposure did not differ significantly by group (p = .48).
Overall, participant retention rates were 91%, 84%, and 74% at the 1-, 6-, and 12-month follow-ups, respectively (see Figure 1 for retention by group). Missingness on the drinking outcome variables was not associated with group or baseline drinking outcomes (ps > .09). Although missingness occurring completely at random cannot be directly tested because the probability of missingness on the outcome variable is assessed as a function of the values of both predictors and outcome variables, analyses suggested that the missingness mechanism may be considered “ignorable” for the primary analyses (Allison, 2001).
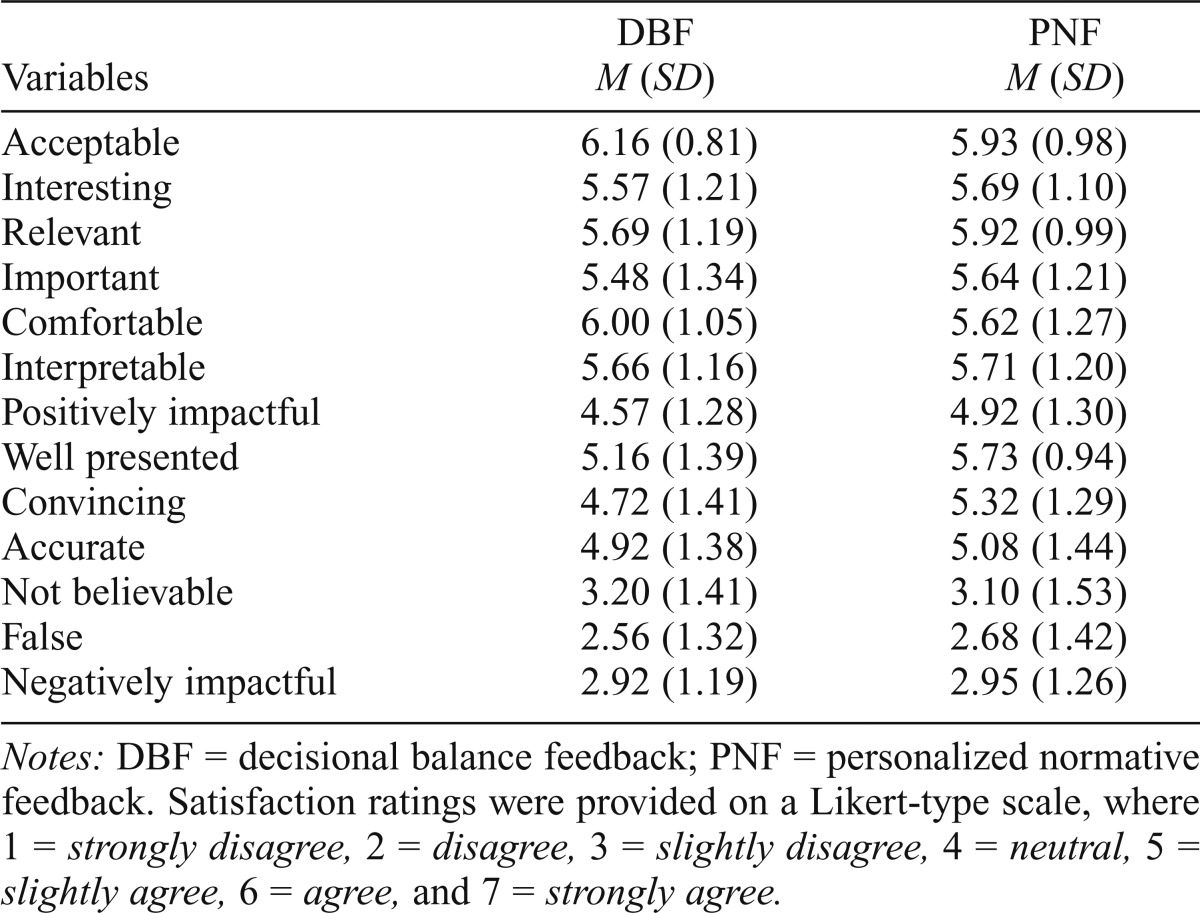
Participant satisfaction with personalized feedback interventions
Aside from neutral scores on items assessing how positively impactful, accurate, and convincing the interventions were, participants in the DBF and PNF groups “slightly agreed” or “agreed” with items indicating satisfaction with personalized feedback interventions and “slightly disagreed” or “disagreed” with items indicating dissatisfaction (see Table 2 for descriptive statistics). Mann–Whitney U tests indicated that DBF participants rated their feedback as significantly more acceptable, z = -2.72, p = .006, and comfortable, z = -3.44, p < .001, than PNF participants. Conversely, PNF participants rated their intervention as more convincing, z = -4.47, p < .001, well presented, z = -4.18, p < .001, and positively impactful, z = -2.91, p = .004, than DBF participants (Table 2). There were no further significant differences between the groups on other satisfaction items (ps > .07).
Table 2.
Participant satisfaction by intervention group
| Variables | DBF M (SD) | PNF M (SD) |
| Acceptable | 6.16 (0.81) | 5.93 (0.98) |
| Interesting | 5.57 (1.21) | 5.69 (1.10) |
| Relevant | 5.69 (1.19) | 5.92 (0.99) |
| Important | 5.48 (1.34) | 5.64 (1.21) |
| Comfortable | 6.00 (1.05) | 5.62 (1.27) |
| Interpretable | 5.66 (1.16) | 5.71 (1.20) |
| Positively impactful | 4.57 (1.28) | 4.92 (1.30) |
| Well presented | 5.16 (1.39) | 5.73 (0.94) |
| Convincing | 4.72 (1.41) | 5.32 (1.29) |
| Accurate | 4.92 (1.38) | 5.08 (1.44) |
| Not believable | 3.20 (1.41) | 3.10 (1.53) |
| False | 2.56 (1.32) | 2.68 (1.42) |
| Negatively impactful | 2.92 (1.19) | 2.95 (1.26) |
Notes: DBF = decisional balance feedback; PNF = personalized normative feedback. Satisfaction ratings were provided on a Likert-type scale, where 1 = strongly disagree, 2 = disagree, 3 = slightly disagree, 4 = neutral, 5 = slightly agree, 6 = agree, and 7 = strongly agree.
Intervention effects on drinking variables
Drinking frequency in the past 30 days.
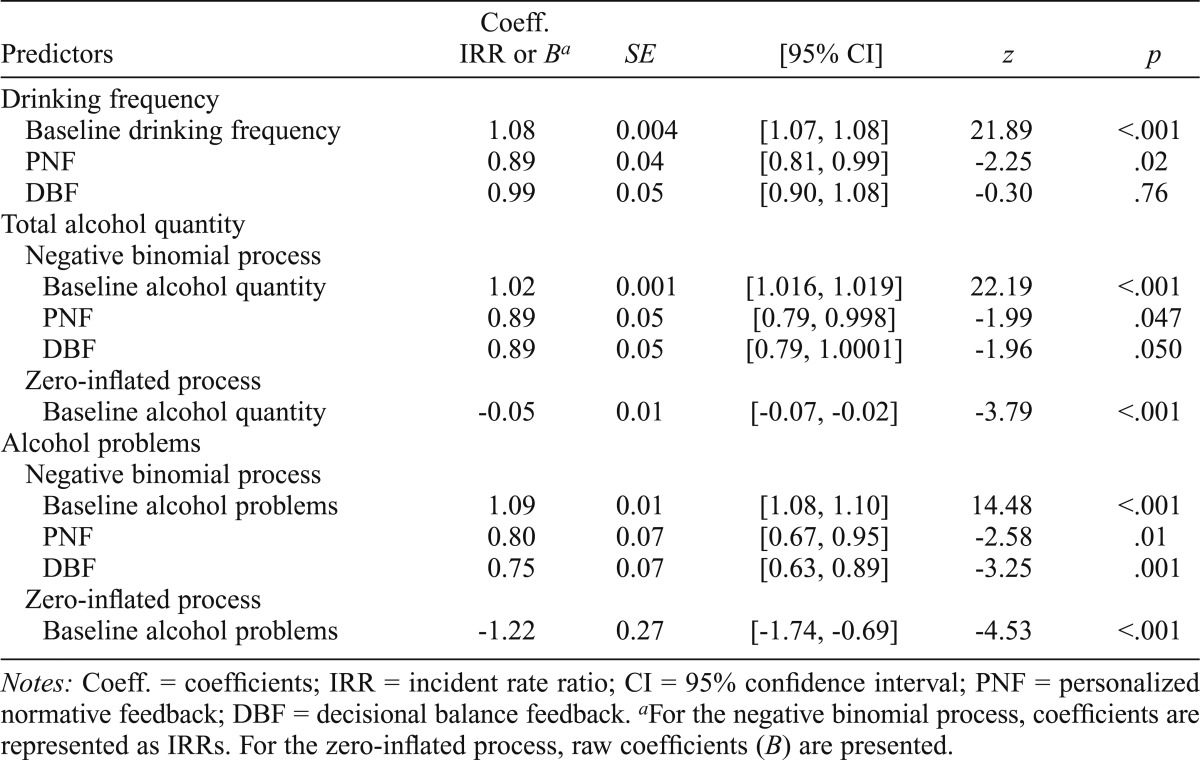
The negative binomial model testing treatment effects on drinking frequency at the 1-month follow-up was significant, χ2(3, n = 668) = 383.20, p < .001, Nagelkerke pseudo-R2 = .44. After we controlled for baseline, PNF participants’ drinking frequency was 11% lower at the 1-month follow-up than that of control participants (see Table 3 for parameter statistics). On the other hand, DBF participants’ drinking frequency was not significantly lower than that of control participants. Comparing DBF and PNF, DBF participants drank significantly more frequently than PNF participants at the 1-month follow-up (IRR = 1.10, p =.046).
Table 3.
Model parameters for short-term drinking outcomes (1-month follow-up)
| Predictors | Coeff. IRR or Ba | SE | [95% CI] | z | p |
| Drinking frequency | |||||
| Baseline drinking frequency | 1.08 | 0.004 | [1.07, 1.08] | 21.89 | <.001 |
| PNF | 0.89 | 0.04 | [0.81, 0.99] | -2.25 | .02 |
| DBF | 0.99 | 0.05 | [0.90, 1.08] | -0.30 | .76 |
| Total alcohol quantity | |||||
| Negative binomial process | |||||
| Baseline alcohol quantity | 1.02 | 0.001 | [1.016, 1.019] | 22.19 | <.001 |
| PNF | 0.89 | 0.05 | [0.79, 0.998] | -1.99 | .047 |
| DBF | 0.89 | 0.05 | [0.79, 1.0001] | -1.96 | .050 |
| Zero-inflated process | |||||
| Baseline alcohol quantity | -0.05 | 0.01 | [-0.07, -0.02] | -3.79 | <.001 |
| Alcohol problems | |||||
| Negative binomial process | |||||
| Baseline alcohol problems | 1.09 | 0.01 | [1.08, 1.10] | 14.48 | <.001 |
| PNF | 0.80 | 0.07 | [0.67, 0.95] | -2.58 | .01 |
| DBF | 0.75 | 0.07 | [0.63, 0.89] | -3.25 | .001 |
| Zero-inflated process | |||||
| Baseline alcohol problems | -1.22 | 0.27 | [-1.74,-0.69] | -4.53 | <.001 |
Notes: Coeff. = coefficients; IRR = incident rate ratio; CI = 95% confidence interval; PNF = personalized normative feedback; DBF = decisional balance feedback.
For the negative binomial process, coefficients are represented as IRRs. For the zero-inflated process, raw coefficients (B) are presented.
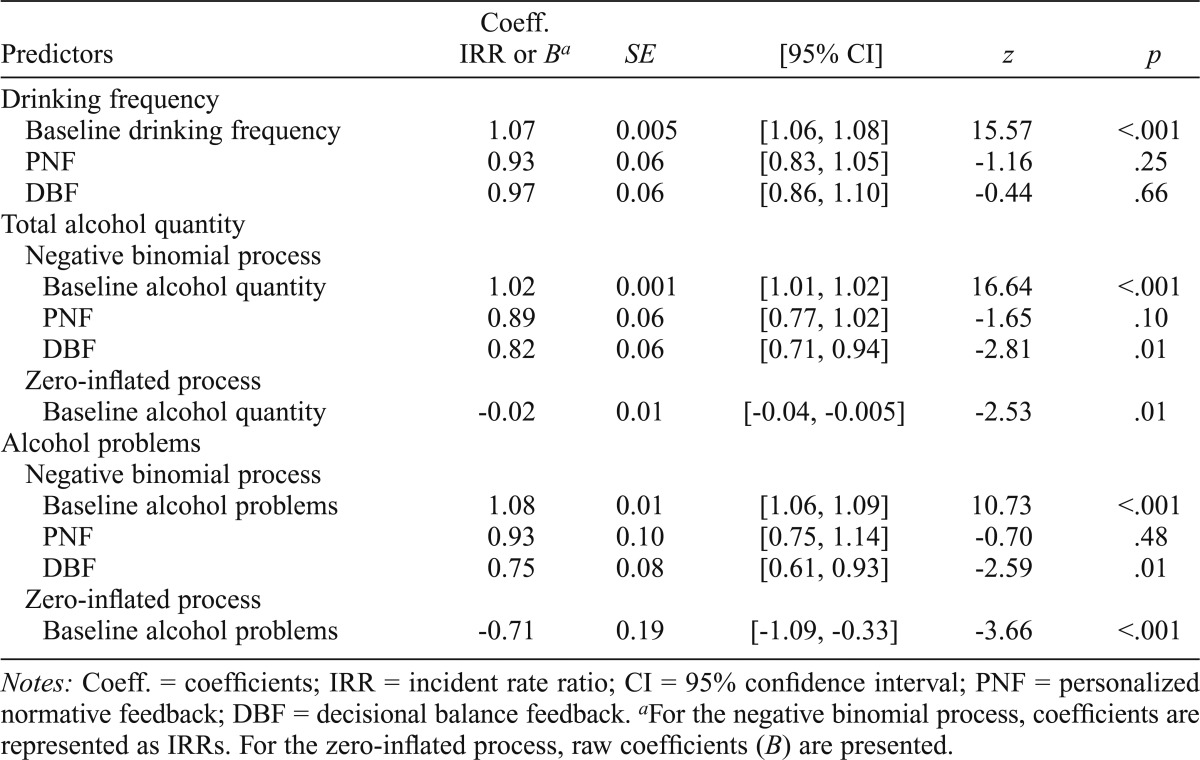
At the 6-month follow-up, the omnibus model was significant, χ2(3, n = 606) = 216.18, p < .001, Nagelkerke pseudo-R2 = .30. However, the only significant predictor was baseline drinking frequency (Table 4).
Table 4.
Model parameters for mid-term drinking outcomes (6-month follow-up)
| Predictors | Coeff. IRR or Ba | SE | [95% CI] | z | p |
| Drinking frequency | |||||
| Baseline drinking frequency | 1.07 | 0.005 | [1.06, 1.08] | 15.57 | <.001 |
| PNF | 0.93 | 0.06 | [0.83, 1.05] | -1.16 | .25 |
| DBF | 0.97 | 0.06 | [0.86, 1.10] | -0.44 | .66 |
| Total alcohol quantity | |||||
| Negative binomial process | |||||
| Baseline alcohol quantity | 1.02 | 0.001 | [1.01, 1.02] | 16.64 | <.001 |
| PNF | 0.89 | 0.06 | [0.77, 1.02] | -1.65 | .10 |
| DBF | 0.82 | 0.06 | [0.71, 0.94] | -2.81 | .01 |
| Zero-inflated process | |||||
| Baseline alcohol quantity | -0.02 | 0.01 | [-0.04, -0.005] | -2.53 | .01 |
| Alcohol problems | |||||
| Negative binomial process | |||||
| Baseline alcohol problems | 1.08 | 0.01 | [1.06, 1.09] | 10.73 | <.001 |
| PNF | 0.93 | 0.10 | [0.75, 1.14] | -0.70 | .48 |
| DBF | 0.75 | 0.08 | [0.61, 0.93] | -2.59 | .01 |
| Zero-inflated process | |||||
| Baseline alcohol problems | -0.71 | 0.19 | [-1.09,-0.33] | -3.66 | <.001 |
Notes: Coeff. = coefficients; IRR = incident rate ratio; CI = 95% confidence interval; PNF = personalized normative feedback; DBF = decisional balance feedback.
For the negative binomial process, coefficients are represented as IRRs. For the zero-inflated process, raw coefficients (B) are presented.
Similarly, the omnibus model at the 12-month follow-up was significant, χ2(3, n = 537) = 129.86, p < .001, Nagelkerke pseudo-R2 = .22, and baseline drinking frequency was the only significant predictor (IRR = 1.06, p < .001).
Drinking quantity in the past 30 days.
The ZINB model testing intervention effects on drinking quantity at the 1-month follow-up was significant, χ2(3, n = 669) = 456.95, p < .001, Nagelkerke pseudo-R2 = .52. After we controlled for baseline, both PNF and DBF participants’ drinking quantity was 11% lower than control participants’ (Table 3); however, the effect of DBF did not quite reach significance (p = .05). PNF and DBF participants did not significantly differ from one another on drinking quantity (p = .95).
At the 6-month follow-up, the omnibus model was significant, χ2(3, n = 606) = 278.25, p < .001, Nagelkerke pseudo-R2 = .39. After we controlled for baseline, DBF participants evinced 18% lower drinking quantity compared with control participants, whereas PNF participants did not maintain a significant difference (Table 4). DBF and PNF participants did not significantly differ from one another at the 6-month follow-up (p = .10).
At the 12-month follow-up, the omnibus model was significant, χ2(3, n = 537) = 202.76, p < .001, Nagelkerke pseudo-R2 = .32. The only significant predictor, however, was baseline drinking quantity (IRR = 1.01, p < .001).
Alcohol-related problems in the past 30 days.
The ZINB model testing intervention effects on alcohol-related problems at the 1-month follow-up was significant, χ2(3, n = 660) = 266.30, p < .001, Nagelkerke pseudo-R2 = .43. Compared with controls, PNF and DBF participants had 20% and 25% lower alcohol-related problem scores, respectively (Table 3). PNF and DBF participants did not significantly differ from one another on alcohol-related problems (p = .50).
At the 6-month follow-up, the omnibus model was significant, χ(3, n = 600) = 156.75, p < .001, Nagelkerke pseudo-R2 = .32. After we controlled for baseline problem scores, DBF participants maintained their 25% reduction in alcohol-related problems compared with control participants, whereas PNF participants did not (Table 4). In fact, DBF participants reported significantly fewer alcohol-related problems than did PNF participants (IRR = 0.81, p = .049).
At the 12-month follow-up, the omnibus model was significant, χ2(3, n = 530) = 110.72, p < .001, Nagelkerke pseudo-R2 = .29. However, the only significant predictor was baseline problem score (IRR = 1.07, p < .001).
Discussion
This study’s aim was to test the efficacy of DBF, a new personalized feedback intervention, compared with assessment-only control and PNF, an established and efficacious personalized feedback intervention, in reducing college drinking and alcohol-related problems. Analyses at the 1-month follow-up indicated that participants receiving DBF and PNF reduced their alcohol-related problems. However, PNF but not DBF participants significantly reduced their drinking frequency and quantity at the 1-month follow-up.
Because both interventions specifically targeted alcohol use and problems, observed short-term improvements in alcohol outcomes were expected. For example, PNF provided participants with feedback regarding their alcohol frequency and quantity in the context of other students of their same gender, and it targeted problems by providing feedback on consequences related to blood alcohol levels, expense, and calories consumed compared with other students. Qualitative research has indicated that students perceive these particular problems as salient and important negative consequences of drinking (Colby et al., 2009; Collins et al., in press).
Conversely, DBF provided feedback on participants’ motivation to change as measured by their own decisional balance of advantages and disadvantages of current drinking and reducing drinking. Specifically, participants received feedback on their decisional balance proportion (i.e., how balanced they were toward reducing alcohol use vs. maintaining current drinking), as well as the number, qualitative content, and weightings of importance and likelihood of their perceived advantages and disadvantages of current drinking and self-defined drinking reduction. Because DBF highlighted perceived disadvantages of current drinking, it is understandable that this intervention precipitated a decrease in alcohol-related problems at follow-up. Consistent with decision-making theory (Janis and Mann, 1977), motivational theory (Miller, 1999), and the transtheoretical model (Prochaska, 1994; Prochaska et al., 1994), DBF likely helped individuals develop and resolve actual-ought or actual-ideal discrepancies in behavior related to their experience of alcohol-related problems.
The interventions differed in terms of longevity of effects. Specifically, DBF participants showed reductions in drinking quantity and alcohol-related problems at the 6-month follow-up, whereas PNF effects were only evident at the 1-month follow-up. DBF may confer longer lasting effects because it aims to create intrapersonal or intrinsic discrepancies around people’s goals and desired behavior (Miller, 1999), which may increase the salience and importance of comparing present behavior with future goals or desired behavior. PNF, on the other hand, relies on developing discrete interpersonal discrepancies, which are primarily focused in the present and may be less salient if individuals do not identify with the applied normative group (e.g., Lewis and Neighbors, 2007).
The specific PNF content may also help explain this finding. Some prior studies have involved PNF focused on alcohol consumption only (i.e., drinking frequency and quantity), whereas the PNF in this study additionally provided information on calories consumed and money spent. Feedback on calories consumed and money spent has been included in prior studies of PNF with college students (Walters and Neighbors, 2005). It is, however, possible that this additional PNF content diluted the message or interfered with the consistency of the feedback (e.g., PNF may have indicated that students consumed more than their peers yet did not spend a lot of money on alcohol), which may have decreased the longevity of its effects. Indeed, prior research has shown that longer interventions or the addition of information or components does not necessarily augment intervention effects (Kulesza et al., 2010).
Neither group maintained alcohol use or problem reductions at the 12-month follow-up. On the one hand, this finding is consistent with existing literature, which has shown that computer-delivered interventions—sometimes only consisting of PNF—have short-lived effects (Carey et al., 2012). On the other hand, it stands in contrast with newer research studies, in which web-based PNF has been associated with drinking reductions through the 6- (Lewis et al., 2013) and 12-month follow-ups (LaBrie et al., 2013).
Limitations
Limitations of this study deserve mention. Given the overrepresentation of seniors, a disproportionate number of participants had reached the legal drinking age and may not have had the same factors influencing their drinking as a younger sample (e.g., only being able to drink at larger parties where alcohol is provided; fear of legal repercussions). This older sample may also be more experienced with drinking than other college samples, which could limit generalizability to the college drinking population as a whole. Last, given the skewness toward older students, the PNF may not have been deemed as relevant as if it had been focused on age-matched peers.
Second, drinking outcomes were based on self-report, which is subject to inaccuracies resulting from memory biases, social desirability, and item wording (Belli, 1998; Bickart et al., 2006; Davis et al., 2010; Garry et al., 2002). Self-report can, however, be reliable when timeframes are manageable, behaviors are not stigmatized, and there are no negative consequences tied to disclosure (Babor et al., 1987; Carey, 2002; Maisto et al., 1982).
Conclusions and future directions
The present findings provided preliminary evidence that web-based DBF is an efficacious intervention for college drinking. Although neither DBF nor PNF interventions showed effects past the 6-month follow-up, the DBF effects were longer lasting than those of the PNF. Despite some limitations around generalizability of the current sample, these study findings indicate that DBF is a promising web-based intervention for at-risk college drinkers.
It has been previously posited that the decisional balance may help individuals develop and resolve intrapersonal discrepancy (Miller, 1999), such as actual-ideal and actual-ought discrepancy (Higgins, 1987; McNally et al., 2005). Findings suggest that DBF’s focus on intrapersonal discrepancy may be as effective in precipitating decreases in alcohol use and problems as PNF’s focus on interpersonal discrepancy. Future studies are necessary to replicate these promising findings, explore potential underlying mechanisms, and understand whether combining the two types of interventions can boost their overall effectiveness.
Acknowledgments
The authors thank Samantha Chalker, Laura Haelsig, Jennifer Hicks, Gail Hoffman, Jessica Holttum, Ami Kanagawa, Mayanka Nehru, Anthony Olds, Morgan Quick, Emily Taylor, and Katy Thysell for their assistance with participant and data management; Eric Ping for his expert computer programming; and Drs. Mary E. Larimer and Clayton Neighbors for their consultation on this project.
Footnotes
This research was supported by National Institute on Alcohol Abuse and Alcoholism Career Transition Award K22AA018384 (to Susan E. Collins). Megan Kirouac is now at the University of New Mexico.
References
- Allison PD. Missing data. Thousand Oaks, CA: Sage; 2001. [Google Scholar]
- Apodaca TR, Longabaugh R. Mechanisms of change in motivational interviewing: A review and preliminary evaluation of the evidence. Addiction. 2009;104:705–715. doi: 10.1111/j.1360-0443.2009.02527.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Babor TF, Stephens RS, Marlatt GA. Verbal report methods in clinical research on alcoholism: Response bias and its minimization. Journal of Studies on Alcohol. 1987;48:410–423. doi: 10.15288/jsa.1987.48.410. [DOI] [PubMed] [Google Scholar]
- Baer JS, Stacy A, Larimer M. Biases in the perception of drinking norms among college students. Journal of Studies on Alcohol. 1991;52:580–586. doi: 10.15288/jsa.1991.52.580. [DOI] [PubMed] [Google Scholar]
- Bandura A. Social learning theory. New York, NY: General Learning Press; 1977. [Google Scholar]
- Belli RF. The structure of autobiographical memory and the event history calendar: Potential improvements in the quality of retrospective reports in surveys. Memory. 1998;6:383–406. doi: 10.1080/741942610. [DOI] [PubMed] [Google Scholar]
- Bickart BA, Phillips JM, Blair J. The effects of discussion and question wording on self and proxy reports of behavioral frequencies. Marketing Letters. 2006;17:167–180. [Google Scholar]
- Blanco C, Okuda M, Wright C, Hasin DS, Grant BF, Liu SM, Olfson M. Mental health of college students and their non-college-attending peers: Results from the National Epidemiologic Study on Alcohol and Related Conditions. Archives of General Psychiatry. 2008;65:1429–1437. doi: 10.1001/archpsyc.65.12.1429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borsari B, Carey KB. Effects of a brief motivational intervention with college student drinkers. Journal of Consulting and Clinical Psychology. 2000;68:728–733. [PubMed] [Google Scholar]
- Borsari B, Carey KB. Descriptive and injunctive norms in college drinking: A meta-analytic integration. Journal of Studies on Alcohol. 2003;64:331–341. doi: 10.15288/jsa.2003.64.331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cameron AC, Trivedi PK. Regression analysis of count data. Cambridge, England: Cambridge University Press; 1998. [Google Scholar]
- Carey KB. Clinically useful assessments: Substance use and comorbid psychiatric disorders. Behaviour Research and Therapy. 2002;40:1345–1361. doi: 10.1016/s0005-7967(02)00039-6. [DOI] [PubMed] [Google Scholar]
- Carey KB, Carey MP, Maisto SA, Henson JM. Brief motivational interventions for heavy college drinkers: A randomized controlled trial. Journal of Consulting and Clinical Psychology. 2006;74:943–954. doi: 10.1037/0022-006X.74.5.943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey KB, Scott-Sheldon LA, Elliott JC, Garey L, Carey MP. Face-to-face versus computer-delivered alcohol interventions for college drinkers: A meta-analytic review, 1998 to 2010. Clinical Psychology Review. 2012;32:690–703. doi: 10.1016/j.cpr.2012.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey KB, Scott-Sheldon LAJ, Carey MP, DeMartini KS. Individual-level interventions to reduce college student drinking: A meta-analytic review. Addictive Behaviors. 2007;32:2469–2494. doi: 10.1016/j.addbeh.2007.05.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carey KB, Scott-Sheldon LAJ, Elliott JC, Bolles JR, Carey MP. Computer-delivered interventions to reduce college student drinking: A meta-analysis. Addiction. 2009;104:1807–1819. doi: 10.1111/j.1360-0443.2009.02691.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carney MA, Tennen H, Affleck G, Del Boca FK, Kranzler HR. Levels and patterns of alcohol consumption using timeline follow-back, daily diaries and real-time “electronic interviews.”. Journal of Studies on Alcohol. 1998;59:447–454. doi: 10.15288/jsa.1998.59.447. [DOI] [PubMed] [Google Scholar]
- Colby SM, Colby JJ, Raymond GA. College versus the real world: Student perceptions and implications for understanding heavy drinking among college students. Addictive Behaviors. 2009;34:17–27. doi: 10.1016/j.addbeh.2008.07.023. [DOI] [PubMed] [Google Scholar]
- Collins SE, Carey KB. Lack of effect for decisional balance as a brief motivational intervention for at-risk college drinkers. Addictive Behaviors. 2005;30:1425–1430. doi: 10.1016/j.addbeh.2005.01.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins SE, Carey KB, Otto JM. A new decisional balance measure of motivation to change among at-risk college drinkers. Psychology of Addictive Behaviors. 2009;23:464–471. doi: 10.1037/a0015841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins SE, Carey KB, Sliwinski MJ. Mailed personalized normative feedback as a brief intervention for at-risk college drinkers. Journal of Studies on Alcohol. 2002;63:559–567. doi: 10.15288/jsa.2002.63.559. [DOI] [PubMed] [Google Scholar]
- Collins SE, Kirouac M, Taylor E, Spelman P, Grazioli V, Hoffman G, et al. Advantages and disadvantages of college drinking in students’ own words: Content analysis of the decisional balance worksheet. Psychology of Addictive Behaviors. in press. [DOI] [PubMed]
- Colten ME, Janis IL. Effects of moderate self-disclosure and the balance-sheet procedure. In: Janis IL, editor. Counseling on personal decisions: Theory and research on helping in short-term relationships. New Haven, CT: Yale University Press; 1982. pp. 159–171. [Google Scholar]
- Cronce JM, Larimer ME. Individual-focused approaches to the prevention of college student drinking. Alcohol Research & Health. 2011;34:210–221. [PMC free article] [PubMed] [Google Scholar]
- Cunningham JA, Sobell LC, Gavin DR, Sobell MB, Breslin FC. Assessing motivation for change: Preliminary development and evaluation of a scale measuring the costs and benefits of changing alcohol or drug use. Psychology of Addictive Behaviors. 1997;11:107–114. [Google Scholar]
- Davis CG, Thake J, Vilhena N. Social desirability biases in self-reported alcohol consumption and harms. Addictive Behaviors. 2010;35:302–311. doi: 10.1016/j.addbeh.2009.11.001. [DOI] [PubMed] [Google Scholar]
- DeJong W, Larimer ME, Wood MD, Hartman R. NIAAA’s rapid response to college drinking problems initiative: Reinforcing the use of evidence-based approaches in college alcohol prevention. Journal of Studies on Alcohol and Drugs, Supplement. 2009;16:5–11. doi: 10.15288/jsads.2009.s16.5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DiClemente CC. Changing addictive behaviors: A process perspective. Current Directions in Psychological Science. 1993;2:101–106. [Google Scholar]
- Dimeff LA, Baer JS, Kivlahan DR, Marlatt GA. Brief alcohol screening and intervention for college students (BASICS): A harm reduction approach. New York, NY: Guilford Press; 1999. [Google Scholar]
- Garry M, Sharman SJ, Feldman J, Marlatt GA, Loftus EF. Examining memory for heterosexual college students’ sexual experiences using an electronic mail diary. Health Psychology. 2002;21:629–634. doi: 10.1037//0278-6133.21.6.629. [DOI] [PubMed] [Google Scholar]
- Goldman MS, Boyd GM, Faden V. College drinking, what it is, and what to do about it: A review of the state of the science (pp. 5–240. Journal of Studies on Alcohol, Supplement 14. 2002 [Google Scholar]
- Hardin JW, Hilbe JM. Generalized linear models and extensions. 2nd ed. College Station, TX: Stata Press; 2007. [Google Scholar]
- Higgins ET. Self-discrepancy: A theory relating self and affect. Psychological Review. 1987;94:319–340. [PubMed] [Google Scholar]
- Hingson RW, Zha W, Weitzman ER. Magnitude of and trends in alcohol-related mortality and morbidity among U.S. college students ages 18-24, 1998-2005. Journal of Studies on Alcohol and Drugs, Supplement. 2009;16:12–20. doi: 10.15288/jsads.2009.s16.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Janis IL, Mann L. Decision-making: A psychological analysis of conflict, choice, and commitment. New York, NY: The Free Press; 1977. [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national survey results on drug use, 1975-2011: Volume II, College students and adults ages 19-50. Ann Arbor, MI: Institute for Social Research, The University of Michigan; 2012. [Google Scholar]
- King TK, DiClemente CC. A decisional balance measure for assessing and predicting drinking behavior. Atlanta, GA: Paper presented at the Annual Conference of the Association for the Advancement of Behavior Therapy; 1993. [Google Scholar]
- Kulesza M, Apperson M, Larimer ME, Copeland AL. Brief alcohol intervention for college drinkers: How brief is? Addictive Behaviors. 2010;35:730–733. doi: 10.1016/j.addbeh.2010.03.011. [DOI] [PubMed] [Google Scholar]
- LaBrie JW, Lewis MA, Atkins DC, Neighbors C, Zheng C, Kenny SR, Larimer ME. RCT of web-based personalized normative feedback for college drinking prevention: Are typical student norms good enough? Manuscript submitted for publication; 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LaBrie JW, Pedersen ER, Earleywine M, Olsen H. Reducing heavy drinking in college males with the decisional balance: Analyzing an element of motivational interviewing. Addictive Behaviors. 2006;31:254–263. doi: 10.1016/j.addbeh.2005.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- LaBrie JW, Pedersen ER, Thompson AD, Earleywine M. A brief decisional balance intervention increases motivation and behavior regarding condom use in high-risk heterosexual college men. Archives of Sexual Behavior. 2008;37:330–339. doi: 10.1007/s10508-007-9195-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Langley JD, Kypri K, Stephenson SCR. Secondhand effects of alcohol use among university students: Computerised survey. BMJ. 2003;327:1023–1024. doi: 10.1136/bmj.327.7422.1023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis MA, Neighbors C. Optimizing personalized normative feedback: The use of gender-specific referents. Journal of Studies on Alcohol and Drugs. 2007;68:228–237. doi: 10.15288/jsad.2007.68.228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis MA, Patrick ME, Litt DM, Blayney JA, Atkins DC, Kim T, Larimer ME. Randomized controlled trial of a web-delivered personalized normative feedback intervention to reduce alcohol-related risky sexual behavior. Manuscript submitted for publication; 2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maisto SA, Sobell MB, Sobell LC. Reliability of self-reports of low ethanol consumption by problem drinkers over 18 months of follow-up. Drug and Alcohol Dependence. 1982;9:273–278. doi: 10.1016/0376-8716(82)90066-7. [DOI] [PubMed] [Google Scholar]
- Marlatt GA, Baer JS, Kivlahan DR, Dimeff LA, Larimer ME, Quigley LA, Williams E. Screening and brief intervention for high-risk college student drinkers: results from a 2-year follow-up assessment. Journal of Consulting and Clinical Psychology. 1998;66:604–615. doi: 10.1037//0022-006x.66.4.604. [DOI] [PubMed] [Google Scholar]
- McNally AM, Palfai TP, Kahler CW. Motivational interventions for heavy drinking college students: Examining the role of discrepancy-related psychological processes. Psychology of Addictive Behaviors. 2005;19:79–87. doi: 10.1037/0893-164X.19.1.79. [DOI] [PubMed] [Google Scholar]
- Migneault JP, Velicer WF, Prochaska JO, Stevenson JF. Decisional balance for immoderate drinking in college students. Substance Use & Misuse. 1999;34:1325–1346. doi: 10.3109/10826089909029387. [DOI] [PubMed] [Google Scholar]
- Miller ET, Neal DJ, Roberts LJ, Baer JS, Cressler SO, Metrik J, Marlatt GA. Test-retest reliability of alcohol measures: Is there a difference between internet-based assessment and traditional methods? Psychology of Addictive Behaviors. 2002;16:56–63. [PubMed] [Google Scholar]
- Miller WR. Enhancing motivation for change in substance abuse treatment (Vol. 35) Rockville, MD: U.S. Department of Health and Human Services; 1999. [PubMed] [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Helping people change. 3rd ed. New York, NY: Guilford Press; 2012. [Google Scholar]
- Monti PM, Barnett NP, Colby SM, Gwaltney CJ, Spirito A, Rohsenow DJ, Woolard R. Motivational interviewing versus feedback only in emergency care for young adult problem drinking. Addiction. 2007;102:1234–1243. doi: 10.1111/j.1360-0443.2007.01878.x. [DOI] [PubMed] [Google Scholar]
- Neal DJ, Simons JS. Inference in regression models of heavily skewed alcohol use data: A comparison of ordinary least squares, generalized linear models, and bootstrap resampling. Psychology of Addictive Behaviors. 2007;21:441–452. doi: 10.1037/0893-164X.21.4.441. [DOI] [PubMed] [Google Scholar]
- Neighbors C, Lewis MA, Bergstrom RL, Larimer ME. Being controlled by normative influences: Self-determination as a moderator of a normative feedback alcohol intervention. Health Psychology. 2006;25:571–579. doi: 10.1037/0278-6133.25.5.571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prochaska JO. Strong and weak principles for progressing from precontemplation to action on the basis of twelve problem behaviors. Health Psychology. 1994;13:47–51. doi: 10.1037//0278-6133.13.1.47. [DOI] [PubMed] [Google Scholar]
- Prochaska JO, Velicer WF, Rossi JS, Goldstein MG, Marcus BH, Rakowski W, Rossi SR. Stages of change and decisional balance for 12 problem behaviors. Health Psychology. 1994;13:39–46. doi: 10.1037//0278-6133.13.1.39. [DOI] [PubMed] [Google Scholar]
- Riper H, van Straten A, Keuken M, Smit F, Schippers G, Cuijpers P. Curbing problem drinking with personalized-feedback interventions: A meta-analysis. American Journal of Preventive Medicine. 2009;36:247–255. doi: 10.1016/j.amepre.2008.10.016. [DOI] [PubMed] [Google Scholar]
- Sobell LC, Sobell MB. Timeline followback: A technique for assessing self-reported ethanol consumption. In: Allen J, Litten RZ, editors. Measuring alcohol consumption: Psychosocial and biological methods. Totowa, NJ: Humana Press; 1992. pp. 41–72. [Google Scholar]
- Wagener TL, Leffingwell TR, Mignogna J, Mignogna MR, Weaver CC, Cooney NJ, Claborn KR. Randomized trial comparing computer-delivered and face-to-face personalized feedback interventions for high-risk drinking among college students. Journal of Substance Abuse Treatment. 2012;43:260–267. doi: 10.1016/j.jsat.2011.11.001. [DOI] [PubMed] [Google Scholar]
- Walters ST, Neighbors C. Feedback interventions for college alcohol misuse: What, why and for whom? Addictive Behaviors. 2005;30:1168–1182. doi: 10.1016/j.addbeh.2004.12.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wechsler H, Dowdall GW, Davenport A, Rimm EB. A gender-specific measure of binge drinking among college students. American Journal of Public Health. 1995;85:982–985. doi: 10.2105/ajph.85.7.982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wechsler H, Nelson TF. What we have learned from the Harvard School of Public Health College Alcohol Study: Focusing attention on college student alcohol consumption and the environmental conditions that promote it. Journal of Studies on Alcohol and Drugs. 2008;69:481–490. doi: 10.15288/jsad.2008.69.481. [DOI] [PubMed] [Google Scholar]
- White HR, Labouvie EW. Towards the assessment of adolescent problem drinking. Journal of Studies on Alcohol. 1989;50:30–37. doi: 10.15288/jsa.1989.50.30. [DOI] [PubMed] [Google Scholar]