

Abstract
Objectives
The last prevalence survey encompassing urban populations was part of the nationwide Health and Nutrition examination survey (NHANES I) in the 1970's. We carried out a prevalence survey for hip osteoarthritis (OA) in the Framingham Study Community cohort.
Methods
Persons age 50 and older living in Framingham in 2002 – 2005 were recruited by random digit dialing without respect to joint pain or arthritis. Anteroposterior standing long-limb radiographs of the lower extremities including the pelvis were obtained and read for radiographic hip OA (ROA) by two trained physicians with all possible cases of ROA confirmed by an experienced musculoskeletal radiologist. ROA was defined as Kellgren-Lawrence score ≥ 2. Using a homunculus in which the hip joint was depicted, participants were asked whether they had hip pain on most days. Those who said ‘yes’ were defined as having hip pain. Symptomatic hip OA (SxOA) was defined as radiographic OA with ipsilateral hip pain. We defined a person as having hip OA if at least one of their hip joints was affected.
Results
Of 978 subjects studied (mean age 63.5 years; 56% women), age-standardized prevalence of ROA was 19.6% (95% CI 16.7%-23.0%) and SxOA was 4.2% (95% CI 2.9%-6.1%%). Overall, we found that men had higher prevalence of ROA (p<0.0001) compared to women, but men did not have a higher prevalence of SxOA compared to women (5.2% vs 3%, p=0.08).
Conclusion
In conclusion, hip osteoarthritis is a common condition in middle aged and older persons in urban and suburban U.S.
Background
Osteoarthritis is the leading cause of disability in middle aged and elderly persons, and hip osteoarthritis accounts for much of this burden. It causes pain, gait abnormalities, and functional impairments. According to the American Academy of Orthopaedic Surgeons, more than 231,000 total hip replacements are performed each year in the United States (US), most of them for treatment of hip osteoarthritis.
Despite this, little is known of the prevalence of symptomatic hip OA in the US, especially in urban populations. There has been only one prevalence study of hip OA in the urban US to our knowledge (1). The nationwide Health and Nutrition examination survey (NHANES I) carried out a hip OA prevalence survey in the early 1970's. Its estimates of prevalence for disease (prevalence of symptomatic hip OA < 1% in persons age 55-79) are far lower than those of other studies (1,2). Under-reading of the NHANES x-rays has been documented making the estimates from this study suspect (2,3). While there have been estimates of disease prevalence in the U.S. from a rural population, rural environments and farming are known risk factors for hip OA, leaving uncertain the burden of disease in most of the US whose population is predominantly urban and suburban (4–9). European studies have shown a higher prevalence of hip OA compared to NHANES I (7,8,10,11). We carried out a prevalence survey for hip OA in the Framingham Study Community cohort, one of the subgroups of the Framingham Osteoarthritis Study and one whose recruitment was community based.
Methods
We performed a community-based study of osteoarthritis in the city of Framingham in 2002 – 2005. We recruited participants aged 50 years and older using random digit dialing from the year 2000 census data from the town of Framingham, Massachusetts. Subjects were not selected for the study based on having joint problems. At least 15 attempts were made to contact potential subjects by telephone over a 4-week period before a telephone number was retired from the list of randomly selected numbers. Repeated attempts were made at least once each during daytime hours on a weekday, evening hours on a weekday, and weekend hours, although most were called several times during each of these periods. To enhance recruitment efforts, flyers were posted in public areas, and community leaders and Framingham senior centers were informed of the study. Our study, including our call strategy, was approved by the institutional review board of Boston University Medical Center.
Inclusion criteria required subjects to be ambulatory (use of assistive devices such as canes and walkers was allowed) with no plans to move away from the area for at least 5 years. Subjects were excluded if they had a history of bilateral total knee replacement, rheumatoid arthritis, dementia, terminal cancer or contraindications to MRI. Those with hip replacement were not excluded. Of the 2582 eligible subjects contacted, 1830 subjects expressed initial interest in participating. Of those, 791 of 1830 that did not eventually take part in the study, 39 were lost to contact, 194 were ineligible for study (most not in the appropriate age range), and the rest (558) subsequently declined to participate even though initially expressing interest. A flowsheet of participation has been published elsewhere (12). Ultimately we studied 1039 subjects who were examined during the period from October 2002 to June 2005.
For symptom assessment, subjects filled out questionnaires, answering questions regarding the presence and frequency of joint symptoms. Subjects indicated on a homunculus whether they had hip joint pain or discomfort on most days of the previous month.
As part of this examination, anteroposterior standing long-limb radiographs of the lower extremities including the pelvis were obtained using a near horizontal beam. While these were originally obtained primarily to assess mechanical alignment of the limb, they included images of both hip joints, and these images were used to assess hip osteoarthritis prevalence in this study. To determine whether long limb films adequately captured hip OA, we compared long-limb films with pelvis films from Osteoarthritis Initiative (OAI) subjects who had both sets of films (although not at the same examination) (see figure 1 for example of long limb film and pelvis film of a typical OAI participant). One hundred OAI subjects with both sets of films were evaluated, and their pelvis films were read independently from their long-limb films. For the presence of radiographic OA, the agreement for OA between pelvis and long limb films using one reader (CK) was kappa = 0.72 (p<.001).
Figure 1. Example of AP Pelvis and Standing Long Limb Films (from same person).

Films where both hips were unreadable were excluded. Films were assessed for Kellgren-Lawrence grade: radiographic OA (ROA) was defined as K/L ≥ 2 (at least probable joint space narrowing in either superolateral or superomedial hip joint plus an osteophyte). The joint space narrowing and osteophyte size were assessed in accordance with the OARSI atlas (13). Two readers (KL and CK) who received training from an experienced musculoskeletal radiologist (AG) read all films. KL served as 1st screener for disease. All films showing KL read as showing possible osteoarthritis of either hip were verified by AG, but he did not read films KL screened as negative. To ensure we did not miss any films showing hip OA, all films not screened by AG were read by CK. All films read that CK read as showing possible osteoarthritis of either hip were verified by AG. To further ensure we did not miss hip OA, we asked AG to read 66 hips scored as not having OA by CK mixed with positive films, and AG read only 1 of these 66 hips (1.5%) as showing OA. Assuming AG was the gold standard, our approach to reading had a sensitivity of 98.5%. Specificity was presumed high given the serial approach to diagnosis (x-rays had to be read as positive by both readers, an approach that minimizes false positives). The interobserver agreement for OA between CK and AG was kappa = 0.71 (p<.001). Symptomatic hip OA (SxOA) was defined as radiographic OA with ipsilateral hip pain (done similarly in the other US prevalence study) (14). We defined a person as having hip OA if at least one of their hip joints was affected. Persons with a hip replacement were defined as having both radiographic and symptomatic hip OA in that joint (n=22 subjects).
SAS was used to analyze the dataset. Another statistical program R was used to obtain age-standardized rate using the CDC year 2000 population data (15). Proportions were compared using chi square or Fisher's exact test as appropriate.
Results
One thousand thirty-nine participants underwent radiography. Of those, 60 subjects were excluded as their films were unreadable, and 1 subject had missing questionnaires. Of the remaining 978 subjects (table 1) evaluated, mean age was 63.5 years (SD 9.0 years; range 51-92). Women accounted for 56% of the sample, and mean BMI was 27.9 (SD 4.8; range 16.6-51.0). Caucasians accounted for 93% of subjects. Hip pain was present in 24.7% (CI 95% 21.2%, 28.6%) of women and 14.7% (CI95% 11.4, 18.0) of men. Among x-rays read, 18.5% of people had radiographic hip OA in at least one hip (13.7% unilateral) and 4.0% had symptomatic hip OA (3.6% unilateral). The age standardized estimate of radiographic hip OA was 19.6% and of symptomatic hip OA, it was 4.2%. There was an increase in prevalence of radiographic OA with age (p<0.0001), and a trend toward an increase in prevalence of SxOA with age (p=0.08) (see table 1). Subjects with hip pain had a higher prevalence of ROA than those without hip pain (21.5% ROA with hip pain vs 15.1% ROA without hip pain, p=0.03).
Table 1. Prevalence of Radiographic and Symptomatic Hip Osteoarthritis by Sex, Age.
| Radiographic Hip OA (95% Cl) | Symptomatic Hip OA (95% Cl) | |
|---|---|---|
| Men (n=434) | 24.7% (20.6%-28.7%) | 5.2% (3.3%-7.8%) |
| Women (n=544) | 13.6% (10.7%-16.5%) | 3.0% (1.7%-4.8%) |
| Age 50-59 (n=390) | 14.6% (11.1%-18.1%) | 3.4% (1.8%-5.8%) |
| Age 60-69 (n=337) | 16.6% (12.6%-20.6%) | 2.7% (1.3%-5.1%) |
| Age 70-79 (n=197) | 25.9% (19.8%-32.0%) | 6.3% (3.3%-10.7%) |
| Age ≥ 80 (n=54) | 31.5% (19.1%-43.9%) | 7.4% (0.2%-17.9%) |
| Crude Prevalence | 18.5% (16.1%-20.9%) | 4.0% (2.8%-5.4%) |
| Age-standardized Prevalence | 19.6% (16.7%-23.0%) | 4.2% (2.9%-6.1%) |
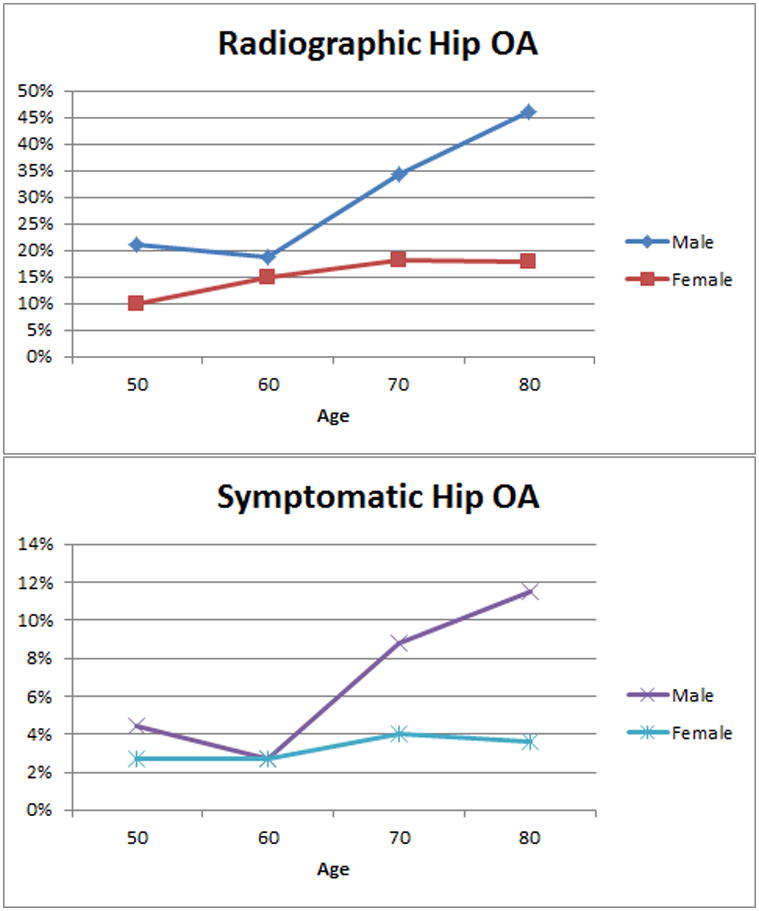
We found men had a higher prevalence of radiographic hip OA (24.7% men ROA vs. 13.6% women ROA, p<0.0001), but men did not have a higher prevalence of SxOA compared to women (5.2% men SxOA vs 3.0% women SxOA, p=0.08) (see figure 2).
Figure 2. Prevalence of Hip OA Per Age Stratified By Sex.
Discussion
In one of the first prevalence studies of hip osteoarthritis from an urban population in the US and the first in many years, we found that 19.6% of subjects, and 50 years old and over had radiographic hip OA in at least one hip. We found that 4.2% of subjects had symptomatic hip OA.
Long-limb x-rays are not usually used for hip osteoarthritis assessment, but they produce readable images of hip structure. We confirmed the suitability of our long limbs readings for the assessment of OA by examining selected pairs of intra-person films from the OAI cohort in which both long limbs and pelvis films were obtained in subjects (although these were not acquired at exactly the same examination).
In the NHANES I study, in those aged 55-74 the prevalence of radiographic hip OA was 3.1%, and that of symptomatic hip OA was 0.7%. However, the prevalences found in NHANES I study are thought to be underestimates as they are systematically and markedly lower than other prevalence studies both in the US and in Europe (2). In NHANES I, non-weight bearing radiographs were used and scores from both hips were averaged so that one hip with disease (grade 2) and one normal hip (grade 0) might be summarized as questionable OA in the person (grade 1), a score interpreted as non-OA.
The Johnston County prevalence study, a prevalence survey of a rural community in the U.S., found a much higher prevalence of osteoarthritis than reported here: 27.6% with radiographic hip OA and 9.7% with symptomatic hip OA (14). However, Johnston County has a higher percentage of African Americans compared to Framingham (∼ 93% Framingham subjects were Caucasians) and African Americans may have higher rates of hip OA. In Johnston County Caucasians, the prevalence of radiograph hip OA was 26.6% and 9.2% had symptomatic hip OA. More importantly, both rural community backgrounds and farming have long been documented to be risk factors for hip OA. Older studies in England and Sweden showed a higher risk of hip OA among farmers, and more recently, rural male farmers in India were shown to be more at risk for hip OA compared to rural male non-farmers (5,7,8). Farming was also shown to be an occupational risk for hip OA in the Netherlands (9).
For symptomatic hip OA, our findings are similar to recent prevalence studies in France (age 50-74, men 1.58-3.9%, women 2.17-5.13%) and slightly lower than Spain (overall 7.4%, men 6.7%, women 8%) (10,11).
In contrast to OA in joints outside the hips, other studies have reported that radiographic hip OA may be equally prevalent in men and women. In NHANES I, radiographic disease was slightly more prevalent in men than women (men 3.5% vs women 2.8%). On the other hand, in Johnston County, it was more prevalent in women (men 24.3% vs women 30.1%). In other prevalence studies, the association of radiographic hip OA with sex has been inconsistent (16).
Unlike radiographic OA, symptomatic OA in the hip tends to be more prevalent in women. In a prevalence study of symptomatic hip OA (defined as having symptoms with corresponding radiographic OA in the same hip) from France, authors found a slightly higher prevalence in women (age 40-75: men 1.9% vs women 2.5%) (10). However, they excluded subjects over age 75, so this may account for finding a lower prevalence compared to ours. In Spain, the prevalence of symptomatic hip OA was 7.4% (men 6.7% and women 8%) (11). In general, hip pain has been reported higher in women (17). Our finding of a modest (and non-significant) male predominance for symptomatic hip OA is unusual in this regard, but is based on small numbers, and the gender difference we found was not statistically significant.
Our study has significant strengths. It was community based and subjects were recruited without reference to joint complaints. The validity of our findings is suggested by the strong association of hip OA prevalence with age and its relation with self reported hip pain. We found that women had a higher prevalence of hip pain than men, and this is consistent with other studies.
Among limitations to this study are that the Framingham community cohort is mostly (although not entirely) Caucasian. There were too few members of other race and ethnic groups to allow for comparisons. The NHANES I study did not find a racial difference of radiographic hip OA between Caucasians and African Americans, whereas the Johnston County study reported a slightly higher prevalence of both symptomatic and radiographic hip OA in African Americans (1,14). Other limitations include the use of long limb films which could have led to a slight underestimation of radiographic hip OA prevalence. We also cannot rule out selection bias with our method of random digit dialing recruitment.
In conclusion, we provide the first prevalence estimate of hip OA prevalence in a community based urban population in the US in many years. Based on these data, we suggest that of those age 50 and over in urban/suburban US, 19.6% of persons have radiographic hip OA and 4.2% have symptomatic disease.
Acknowledgments
Supported by NIH AR47785 and by NIH AG18393
Bibliography
- 1.Tepper S, Hochberg MC. Factors associated with hip osteoarthritis: data from the First National Health and Nutrition Examination Survey (NHANES-I) Am J Epidemiol. 1993;137:1081–1088. doi: 10.1093/oxfordjournals.aje.a116611. [DOI] [PubMed] [Google Scholar]
- 2.Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H, Deyo RA, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part II. Arthritis Rheum. 2008;58:26–35. doi: 10.1002/art.23176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Helmick CG, Felson DT, Lawrence RC, Gabriel S, Hirsch R, Kwoh CK, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part I. Arthritis Rheum. 2008;58:15–25. doi: 10.1002/art.23177. [DOI] [PubMed] [Google Scholar]
- 4.Jordan JM, Linder GF, Renner JB, Fryer JG. The impact of arthritis in rural populations. Arthritis Care Res Off J Arthritis Health Prof Assoc. 1995;8:242–250. doi: 10.1002/art.1790080407. [DOI] [PubMed] [Google Scholar]
- 5.Thelin A, Holmberg S. Hip osteoarthritis in a rural male population: A prospective population-based register study. Am J Ind Med. 2007;50:604–607. doi: 10.1002/ajim.20484. [DOI] [PubMed] [Google Scholar]
- 6.Grubber JM, Callahan LF, Helmick CG, Zack MM, Pollard RA. Prevalence of radiographic hip and knee osteoarthritis by place of residence. J Rheumatol. 1998;25:959–963. [PubMed] [Google Scholar]
- 7.Croft P, Coggon D, Cruddas M, Cooper C. Osteoarthritis of the hip: an occupational disease in farmers. BMJ. 1992;304:1269–1272. doi: 10.1136/bmj.304.6837.1269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Vingård E, Alfredsson L, Goldie I, Hogstedt C. Occupation and osteoarthrosis of the hip and knee: a register-based cohort study. Int J Epidemiol. 1991;20:1025–1031. doi: 10.1093/ije/20.4.1025. [DOI] [PubMed] [Google Scholar]
- 9.Andersen S, Thygesen LC, Davidsen M, Helweg-Larsen K. Cumulative years in occupation and the risk of hip or knee osteoarthritis in men and women: a register-based follow-up study. Occup Environ Med. 2012;69:325–330. doi: 10.1136/oemed-2011-100033. [DOI] [PubMed] [Google Scholar]
- 10.Guillemin F, Rat AC, Mazieres B, Pouchot J, Fautrel B, Euller-Ziegler L, et al. Prevalence of symptomatic hip and knee osteoarthritis: a two-phase population-based survey. Osteoarthr Cartil OARS Osteoarthr Res Soc. 2011;19:1314–1322. doi: 10.1016/j.joca.2011.08.004. [DOI] [PubMed] [Google Scholar]
- 11.Quintana JM, Arostegui I, Escobar A, Azkarate J, Goenaga JI, Lafuente I. Prevalence of knee and hip osteoarthritis and the appropriateness of joint replacement in an older population. Arch Intern Med. 2008;168:1576–1584. doi: 10.1001/archinte.168.14.1576. [DOI] [PubMed] [Google Scholar]
- 12.Englund M, Guermazi A, Gale D, Hunter DJ, Aliabadi P, Clancy M, et al. Incidental meniscal findings on knee MRI in middle-aged and elderly persons. N Engl J Med. 2008;359:1108–1115. doi: 10.1056/NEJMoa0800777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Altman RD, Gold GE. Atlas of individual radiographic features in osteoarthritis, revised. Osteoarthr Cartil OARS Osteoarthr Res Soc. 2007;15(Suppl A):A1–56. doi: 10.1016/j.joca.2006.11.009. [DOI] [PubMed] [Google Scholar]
- 14.Jordan JM, Helmick CG, Renner JB, Luta G, Dragomir AD, Woodard J, et al. Prevalence of hip symptoms and radiographic and symptomatic hip osteoarthritis in African Americans and Caucasians: the Johnston County Osteoarthritis Project. J Rheumatol. 2009;36:809–815. doi: 10.3899/jrheum.080677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Klein RJ, Schoenborn CA. Age adjustment using the 2000 projected U.S. population. Healthy People 2010 Stat Notes Cent Dis Control Prev Cent Health Stat. 2001:1–10. [PubMed] [Google Scholar]
- 16.Felson DT. Epidemiology of hip and knee osteoarthritis. Epidemiol Rev. 1988;10:1–28. doi: 10.1093/oxfordjournals.epirev.a036019. [DOI] [PubMed] [Google Scholar]
- 17.Keenan AM, Tennant A, Fear J, Emery P, Conaghan PG. Impact of multiple joint problems on daily living tasks in people in the community over age fifty-five. Arthritis Rheum. 2006;55:757–764. doi: 10.1002/art.22239. [DOI] [PubMed] [Google Scholar]