

Abstract
Background:
Vitamin D deficiency is common in older adults in Western countries with seasonal winters, when the amount of sunlight is much reduced. There is a paucity of data on the prevalence of vitamin D deficiency in patients with hip fracture in countries such as Singapore where the climate is predominantly tropical.
Objectives:
In this study, our aims were to ascertain the prevalence of vitamin D deficiency and risk factors associated with vitamin D deficiency in hospitalized elderly patients with hip fracture in Singapore.
Methods:
We prospectively studied 485 patients with hip fracture admitted to the orthopedic department over a 1-year period. Nonfragility fractures and younger patients (patients <60 years and those with high-impact injuries) were excluded. Data on patient demographics, comorbidities, functional status, and serum 25-hydroxyvitamin D3 levels were collected. Vitamin D deficiency was defined using Holick classification.
Results:
Vitamin D levels were available for 412 patients. Vitamin D deficiency was present in 57.5% (n = 237). Prevalence of vitamin D insufficiency was 34.5%, with only 8% of patients having normal vitamin D levels. Univariate analyses showed Malay race and functional factors (being housebound, requiring bathing and dressing assistance) to be associated with vitamin D deficiency. However, only ethnicity and housebound patients were significant in the multivariate model.
Conclusions:
Vitamin D deficiency and insufficiency are common in patients with hip fracture in Singapore. Vitamin D deficiency was associated with being housebound and those of Malay ethnicity. Clothing habits resulting in reduced sunlight exposure may increase the risk of vitamin D deficiency.
Keywords: vitamin D, hip fracture, elderly, sunlight
Introduction
Vitamin D deficiency is associated with increased muscle weakness and pain leading to reduced strength, balance, and function1; increased bone turnover2,3; and increased risk of falls and hip fractures4 in older adults. Elderly people are at greater risk of vitamin D deficiency because of risk factors such as (1) suboptimal sunlight exposure and lower cutaneous synthesis of vitamin D, (2) reduced dietary intake of D2 (ergocalciferol) and D3 (cholecalciferol), (3) impaired intestinal absorption, and (4) impaired hydroxylation in the liver and kidneys1
Vitamin D deficiency is common in elderly patients in Western countries, especially in the early spring due to reduced cutaneous synthesis during winter months,5,6 in housebound individuals,7 and in medical inpatients.8 The prevalence of vitamin D deficiency is even higher in elderly patients with fragility fractures (varying from 55% to 91.6%6,9–12).
Singapore is a multicultural country consisting predominantly of 74.1% Chinese, 13.4% Malays, and 9.2% Indians13 situated 1° north of the equator. It has a tropical rainforest climate with uniform temperature and periods of sunshine throughout the year. We postulated that vitamin D deficiency in Singapore should be lower than in the countries with seasonal winters (ie, with winters in which there is reduced sunlight). There is a paucity of data on prevalence of vitamin D deficiency among patients with hip fracture in tropical countries such as Singapore. There are a few studies in India that revealed high rates (76.7%-96.7%) of vitamin deficiency among patients with hip fracture.14,15
The aims of this study were to ascertain the prevalence of hypovitaminosis D and the risk factors associated with vitamin D deficiency among hospitalized elderly patients with hip fractures in Singapore.
Methods
We did a prospective cohort study from September 01, 2009 to August 31, 2010. These patients were part of the orthogeriatric hip fracture service where patients with hip fracture were comanaged by orthopedic surgeons and geriatricians. A total of 485 consecutive older patients with fragility hip fracture admitted to the orthopedic department were studied. We excluded patients younger than 60 years old and those with high-impact injuries.
Data on patient demographics (age, gender, race, and living arrangements), falls history, premorbid mobility, premorbid functional status, inpatient mortality, and serum 25-hydroxyvitamin D3 levels were collected by a research assistant employed by the Department of Orthopaedic Surgery.
We defined vitamin D deficiency using Holick classification1 where vitamin D deficiency is considered when there is a vitamin D level <20 ng/mL, vitamin D insufficiency is defined as vitamin D level 21 to 29 ng/mL, and normal vitamin D levels are defined as ≥30 ng/mL. The 25-hydroxyvitamin D3 was measured using Roche Cobas e601 immunoassay analyzer (Roche) using the Roche Elecsys vitamin-D3 assay (Roche Mannheim, Germany) in the hospital’s accredited laboratory.
Statistical Analysis
We analyzed the data using Stata version 10.1 (Statacorp, College Station, Texas) statistical software. We present continuous variables as mean and standard deviation, while categorical data are presented as frequency and percentages. We used univariate logistic regression analysis to ascertain the risk factors associated with vitamin D deficiency. The significant risk factors from univariate logistic regression were then entered into a multivariate logistic regression analysis to assess the independent risk factors associated with vitamin D deficiency. We considered a P value of <.05 to be statistically significant. We obtained ethics committee approval for this study from National Healthcare Group Domain Specific Review Board.
Results
A total of 485 patients with hip fracture were admitted during the 1-year period of whom 412 had vitamin D levels measured during their admission. The patients had a mean age of 79.8 years. They were predominantly female (71.4%) and of Chinese ethnicity (88.4%). Most patients were admitted from home (94.9%); only 4.4% were admitted from nursing homes. The majority were community ambulant (64.6%) before the hip fracture. Nearly half of them needed assistance with mobility (46.1%) although most were independent in their basic activities of daily living (see Table 1). Nearly a third (28.2%) were recurrent fallers (defined as ≥2 falls in the last 12 months). Inpatient mortality was low at 1.94%.
Table 1.
Demographics of Patients With Hip Fracture.
| Age, years, mean ± SD (Range) | 79.8 ± 9.1 |
| Gender | |
| Female | 294 (71.4%) |
| Male | 118 (28.6%) |
| Race | |
| Chinese | 364 (88.4%) |
| Malay | 21 (5.1%) |
| Indian | 18 (4.4%) |
| Others | 9 (2.2%) |
| Living arrangement | |
| Home | 391 (94.9%) |
| Nursing home | 18 (4.4%) |
| Sheltered home/others | 3 (0.7%) |
| Falls history | |
| Recurrent fallers | 137 (28.2%) |
| Mobility prior to hip fracture | |
| Community ambulant | 266 (64.6%) |
| Housebound | 146 (35.4%) |
| Assistance required with mobility before hip fracture | |
| Independent without aid | 222 (53.9%) |
| Ambulant with assistance/wheelchair bound | 190 (46.1%) |
| Premorbid bathing | |
| Independent | 323 (78.4%) |
| Bathing with assistance | 89 (21.6%) |
| Premorbid dressing | |
| Independent | 333 (80.8%) |
| Dressing with assistance | 79 (19.2%) |
| Premorbid toileting | |
| Independent | 346 (84.0%) |
| Toileting with assistance | 66 (16.0%) |
| Premorbid transfers | |
| Independent | 357 (86.7%) |
| Transfer with assistance | 55 (13.3%) |
| Premorbid feeding | |
| Independent | 388 (94.2%) |
| Feeding with assistance | 24 (5.8%) |
| Premorbid continence | |
| Continent | 365 (88.6%) |
| Incontinent | 47 (11.4%) |
| More than 3 ADLs assisted | |
| Yes | 67 (16.3%) |
| No | 345 (83.7%) |
| Inpatient mortality | 8 (1.94%) |
Abbreviations: ADLs, activities of daily living; SD, standard deviation.
The mean vitamin D level was 19.1 ng/mL. The prevalence of vitamin D deficiency among hospitalized elderly patients with hip fracture was 57.5% and vitamin D insufficiency was present in 34.5% of patients, with only 8% having normal vitamin D levels (see Figure1). Most Malay patients with hip fracture were vitamin D deficient (90.5%, n = 19).
Figure 1.
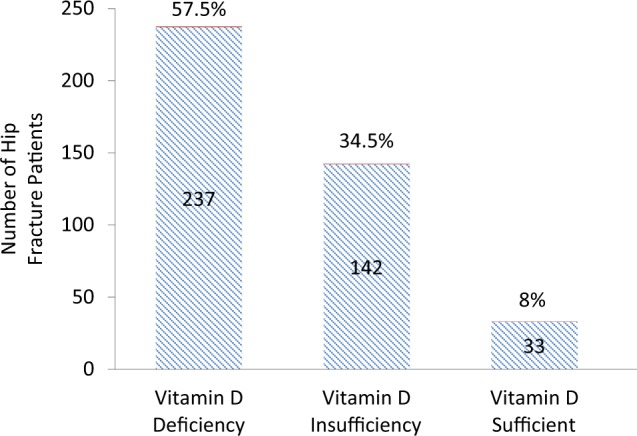
Prevalence of vitamin D deficiency in patients with hip fracture in Singapore.
Upon univariate analysis, Malay patients with hip fracture, (odds ratio [OR] = 7.7, P = .007), housebound patients with hip fracture (OR = 2.05, P = .001), those requiring assistance in bathing (OR = 2.22, P = .002), and dressing (OR= 2.37, P= .002) before the hip fracture were found to be more likely to have vitamin D deficiency (see Table 2). Patients with hip fracture who required assistance in mobility before the hip fracture had a tendency to vitamin D deficiency (OR = 1.47, P = .5) although this did not reach statistical significance. There was no significant association between age, previous number of falls, and living arrangement with vitamin D deficiency. Multivariate analysis showed only Malay race (OR = 6.94, P = .01) and housebound status (OR = 1.97, P = .002) to be associated with vitamin D deficiency (Table 2).
Table 2.
Univariate and Multivariate Analysis of Factors Associated With Vitamin D Deficiency.
| Factors | Odds ratio (95% Confidence Intervals) | P value |
|---|---|---|
| Age | 1.02 (0.99-1.04) | .06 |
| Gender (female) | 1.26 (0.78-1.85) | .39 |
| Race (Malays vs Chinese) | 7.70 (1.77-33.56) | .007 |
| Race (Indians vs Chinese) | 1.27 (0.48-3.36) | .62 |
| Falls history | 0.97 (0.86-1.12) | .75 |
| Charlson comorbidity index score | 1.05 (0.95-1.15) | .31 |
| Nursing home versus home | 1.52 (0.56-4.14) | .41 |
| Housebound versus community ambulant | 2.04 (1.34-3.12) | .001 |
| Mobility with assistance versus independent | 1.47 (1.00-2.19) | .05 |
| Bathing with assistance versus independent | 2.22 (1.33-3.70) | .002 |
| Multivariate analysis | ||
| Race | 6.94 (1.58-30.43) | .01 |
| Housebound versus community ambulant | 1.97 (1.28-3.03) | .002 |
Discussion
This study shows that hypovitaminosis D is common in older patients presenting with hip fractures—even in sunny Singapore. Of the elderly patients with hip fracture, 57.5% had vitamin D deficiency and 34.5% vitamin D insufficiency, with only 8% of patients with hip fracture having sufficient vitamin D levels. This is comparable to deficiency and insufficiency levels found in Western patients with hip fracture.9,10,16 The predominance of female patients with hip fracture also mirrors that seen in Western countries.17 The low inpatient mortality of 1.94% is also not dissimilar to other Comanaged Geriatric Fracture Centres.18
The finding that the housebound state carried a significantly greater risk of vitamin D deficiency compared to previously community-ambulant elderly patients with hip fracture has also been previously reported.17 This group of frailer housebound patients are more likely to have less sun exposure as they are not only confined indoors due to reduced physical activity but are also likely to have other risk factors, such as reduced dietary source of vitamin D as well as coexisting illnesses (such as liver and renal impairment) that could contribute to vitamin D deficiency.
Interestingly, patients with hip fracture previously residing in nursing homes before admission were not significantly associated with vitamin D deficiency. We postulate that this unexpected finding could be explained by the small sample size. A Turkish study had shown that patients living in old age homes had higher risk of vitamin D deficiency than those living in their own homes. In the same study, they also found that clothing habits and exposure to sunlight were also associated with higher risk of vitamin D deficiency.19
We were interested to find the levels of vitamin D deficiency to be 90.5% in Malay patients with hip fracture compared to 55% of Chinese and 61.1% Indian patients with hip facture. Darker skin pigmentation is associated with low vitamin D levels and the presence of genetic factors may have resulted in increased 24-hydroxylase activity in Indians. However, in our study, we did not find any significant differences in Indian patients but only in those of Malay ethnicity. We postulate that this could be related to religious cultural practice of dressing style (long sleeves, head dress for Muslim-Malay females) and this avoidance of sunlight by the Malays could account for the lower vitamin D levels. Similar findings of Malays being at greater risk of vitamin D deficiency than the Chinese were also shown in a recent study in Singapore by Hawkins20 although this was in a younger population. Studies have shown a high prevalence of vitamin D deficiency (49.4%-100%) in healthy young women in the Middle East despite abundant sunlight, and conservative clothing style has been identified as a risk factor.21,22 This is an interesting finding which merits further study for vitamin D genetic polymorphisms, environmental factors, and clothing habits which might account for the ethnic differences observed.
One limitation of this study was that 25-hydroxyvitamin D3 levels were measured rather than total 25-hydroxyvitamin D as that was the only vitamin D assay available at our hospital. More than 95% of 25-hydroxyvitamin D measurable in the serum is 25-hydroxyvitamin D3. 25-Hydroxyvitamin D2 reaches measurable concentration only in patients taking D2 supplements.23 Thankfully, most vitamin D supplements are in the form of 25-hydroxyvitamin D3. Hence 25-hydroxyvitamin D3 correlates very closely to total 25-hydroxyvitamin D. Another limitation was that we did not capture data on whether the patients were taking vitamin D supplementation on admission to hospital. It would have been useful to find out whether those taking supplementation were still at risk of vitamin D deficiency.
Also, the actual definition of vitamin D deficiency is also not universally agreed and cutoffs have been known to vary from 12 to 30 µg/L. The Institute of Medicine has defined serum vitamin D levels of 20 µg/L as adequate and less than 12 µg/L as deficient.24 Holick and the Endocrine Society Clinical Practice Guideline has defined vitamin D deficiency as <20 µg/L and insufficiency as 21 to 29 µg/L.1,25 In this study, we took <20 µg/L to be vitamin D deficient based on Holick classification.1
Furthermore, we do not have the data on which patients had received vitamin D supplementation before admission. The authors of a systematic review and meta-analysis of hip fracture risk in relation to vitamin D supplementation and serum 25-hyroxyvitamin D levels argue that neither higher nor lower dose vitamin D supplementation prevented hip fracture. However, the review consisted mainly of uncontrolled observational studies.26
Conclusion
In summary, this study confirms that vitamin D deficiency is common in elderly patients with hip fracture in Singapore and is associated with being housebound and ethnicity (Malay race). This initial work warrants further larger scale studies of ethnic vitamin D variations and potential causal interrelationship between function (housebound state), cognition, comorbidities, and vitamin D deficiency state on fragility fractures as well as the possible effect of styles of clothing on vitamin D levels.
Acknowledgments
We wish to thank Professor Graham Mulley for his invaluable contributions and advice in improving the manuscript.
Footnotes
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Horlick MF. Vitamin D deficiency. N Engl J Med. 2007;357(3):266–281 [DOI] [PubMed] [Google Scholar]
- 2. Mezuita-Raya P, Muñoz-Torres M, Luna JD, et al. Relation between vitamin D insufficiency, bone density, and bone metabolism in healthy postmenopausal women. J Bone Miner Res. 2001;16(8):1408–1415 [DOI] [PubMed] [Google Scholar]
- 3. Ooms ME, Roos JC, Bezemer PD, van der Vigh WJ, Bouter LM, Lips P. Prevention of bone loss by vitamin D supplementation in elderly women: a randomized double-blind trial. J Clin Endocrinol Metab. 1995;80(4):1052–1058 [DOI] [PubMed] [Google Scholar]
- 4. Cauley JA, LaCroix AZ, Wu L. Serum 25-Hydroxyvitamin D Concentrations and Risk for Hip Fractures. Ann Intern Med. 2008;149(4):242–250 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Looker AC, Dawson-Hughes B, Calvo MS. Serum 25-hydroxyvitamin D status of adolescents and adults in two seasonal subpopulations from NHANES III. Bone. 2002;30(5):771–777 [DOI] [PubMed] [Google Scholar]
- 6. Nurmi I, Kaukonen JP, Lüthje P, et al. Half of the patients with acute hip fracture suffer from hypovitaminosis D: a prospective study in south-eastern Finland. Osteoporos Int. 2005;16(12):2018–2024 [DOI] [PubMed] [Google Scholar]
- 7. Lips P. Vitamin D deficiency and secondary hyperparathyroidism in the elderly: consequences for bone loss and fractures and therapeutic implications. Endocr Rev. 2001;22(4):477–501 [DOI] [PubMed] [Google Scholar]
- 8. Thomas MK, Lloyd-Jones DM, Thadhani RI, et al. Hypovitaminosis D in medical inpatients. N Engl J Med. 1998;338(12):777–783 [DOI] [PubMed] [Google Scholar]
- 9. Gallacher SJ, McQuillian C, Harkness M, Finlay F, Gallagher AP, Dixon T. Prevalence of vitamin D inadequacy in Scottish adults with vertebral fragility fractures. Curr Med Res Opin. 2005;21(9):1355–1361 [DOI] [PubMed] [Google Scholar]
- 10. Moniz C, Dew T, Dixon T. Prevalence of vitamin D inadequacy in osteoporotic hip fracture patients in London. Curr Med Res Opin. 2005;21(12):1891–1894 [DOI] [PubMed] [Google Scholar]
- 11. Beringer T, Heyburn G, Finch M, et al. Prevalence of vitamin D inadequacy in Belfast following fragility fracture. Curr Med Res Opin. 2006;22(1):101–105 [DOI] [PubMed] [Google Scholar]
- 12. LeBoff MS, Kohlmeier L, Hurwitz S, Franklin J, Wright J, Glowacki J. Occult vitamin D deficiency in postmenopausal US women with acute hip fractures. JAMA. 1999;281(16):1505–1511 [DOI] [PubMed] [Google Scholar]
- 13. Singapore Department of Statistics. Census of Population: 2010. http://www.singstat.gov.sg/publications/publications_and_papers/cop2010/census_2010_release1/cop2010sr1.pdf Accessed 21st Jan 2014
- 14. Dhanwal DK, Sahoo S, Gautam VK, Saha R. Hip fracture patients in India have vitamin D deficiency and secondary hyperparathyroidism. Osteoporos Int. 2013;24(2):553–557 [DOI] [PubMed] [Google Scholar]
- 15. Khadgawat R, Brar KS, Gahlo M, et al. High prevalence of vitamin D deficiency in Asian-Indian patients with fragility hip fracture: a pilot study. J Assoc Physicians India. 2010;58:538–542 [PubMed] [Google Scholar]
- 16. Bischoff-Ferrari HA, Can U, Staehelin HB, et al. Severe vitamin D deficiency in Swiss hip fracture patients. Bone. 2008;42(3):597–602 [DOI] [PubMed] [Google Scholar]
- 17. Gloth FM III, Gundberg CM, Hollis BW, Haddard JG, Jr, Tobin JD. Vitamin D deficiency in homebound elderly persons. JAMA. 1995;274(21):1683–1686 [DOI] [PubMed] [Google Scholar]
- 18. Friedman SM, Mendelson DA, Bingham KW, Kates SL. Impact of comanaged Geriatric Fracture Center on short-term hip fracture outcomes. Arch Intern Med. 2009;169(18):1712–1717 [DOI] [PubMed] [Google Scholar]
- 19. Atli T, Gullu S, Uvsal AR, Erdogan G. The prevalence of Vitamin D deficiency and effects of ultraviolet light on vitamin D levels in elderly Turkish population. Arch Gerontol Geriatr. 2005;40(1):53–60 [DOI] [PubMed] [Google Scholar]
- 20. Hawkins RC. 25-OH VitaminD3 Concentrations in Chinese, Malays, and Indians. Clin Chem. 2009;55(9):1749–1751 [DOI] [PubMed] [Google Scholar]
- 21. Al-Mogbel ES. Vitamin D status among adult Saudi Females visiting primary health care clinics. Int J Health Sci (Qassim). 2012;6(2):116–126 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Golgahar J, Al-Saffar N, Altayab Diab D, Al-Othman S, Darwish A, Al-Kafaji G. Predictors of vitamin D deficiency and insufficiency in adult Bahrainis: a cross-sectional study. Public Health Nutr. 2014;17(4):732–738 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Leino A, Turpeinen U, Koskinen P. Automated measurement of 25-OH vitamin D3 on the Roche Modular E170 analyzer. Clin Chem. 2008;54(12):2059–2062 [DOI] [PubMed] [Google Scholar]
- 24. Institute of Medicine (IOM). Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academies Press; 2011 [PubMed] [Google Scholar]
- 25. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96(7):1911–1930 [DOI] [PubMed] [Google Scholar]
- 26. Lai JKC, Lucas RM, Clements MS, Roddam AW, Banks E. Hip fracture risk in relation to vitamin D supplementation and serum 25-hydroxyvitamin D levels: a systematic review and meta-analysis of randomised controlled trials and observational studies. BMC Public Health. 2010;10:331. [DOI] [PMC free article] [PubMed] [Google Scholar]