

Abstract
Infectious causes of peripheral nervous system (PNS) disease are underrecognized but potentially treatable. Heightened awareness educed by advanced understanding of the presentations and management of these infections can aid diagnosis and facilitate treatment. In this review, we discuss the clinical manifestations, diagnosis, and treatment of common bacterial, viral, and parasitic infections that affect the PNS. We additionally detail PNS side effects of some frequently used antimicrobial agents.
Keywords: peripheral nervous system, neuropathy, radiculopathy, infectious disease, antibiotics, antivirals
Introduction
Although relatively rare compared to vascular and primary inflammatory or autoimmune causes, infection can be an unrecognized cause for peripheral nervous system (PNS) disease. However, PNS disease related to infection can cause severe neurological injury, either due to direct effects of the microbe or due to secondary immune overactivation (Table 1). Distinguishing infectious neurologic etiologies from noninfectious ones and understanding the differences between various pathogens can help guide treatment and in some cases cure or at least prevent ongoing injury to the patient. Herein, we approach major infectious causes of radiculopathies, peripheral neuropathies, and neuromuscular junction disorders by causative organism in an attempt to aid in clinical decision making in PNS disease.
Table 1.
Summary of the Most Common Peripheral Nervous System Presentations for Selected Organisms.
| Organism | Clinical Presentation |
|---|---|
| Viruses | |
| HIV | |
| Early disease |
|
| Advanced disease |
|
| Human T-cell lymphotropic virus |
|
| Herpes simplex virus | Sacral radiculitis |
| Varicella-zoster virus |
|
| Cytomegalovirus |
|
| Epstein-Barr virus |
|
| West Nile Virus |
|
| Hepatitis C virus | Axonal sensory polyneuropathy |
| Rabies virus | Acute flaccid paralysis of affected limb |
| Bacteria and mycobacteria | |
| Borrelia burgdorferi |
|
| Corynebacterium diphtheriae |
|
| Campylobacter jejuni | Acute inflammatory demyelinating polyneuropathy |
| Mycobacterium tuberculosis |
|
| Mycobacterium leprae |
|
| Brucella spp. |
|
| Clostridium botulinum | Symmetric descending paralysis |
Abbreviation: HIV, human immunodeficiency virus.
Viruses With Clinical Implications in the PNS
Retroviruses
Human immunodeficiency virus
Any discussion of the PNS complications of infectious disease would be incomplete without comment about human immunodeficiency virus (HIV), arguably the most well-described viral etiology of PNS dysfunction. Human immunodeficiency virus is a retrovirus that is transmitted primarily by sexual contact and contaminated blood. In the most recent reports by the World Health Organization (WHO), an estimated 34 million people were living with HIV in 2011, with significant geographic variability in the prevalence of the disease. Human immunodeficiency virus commonly affects both the central nervous system (CNS) and the PNS (Table 1). Distal symmetric polyneuropathy (DSP) associated with HIV is the most common PNS complaint, affecting up to 30% to 50% of patients with advanced infection.1,2 Typical symptoms of the DSP include paresthesias or numbness in a stocking-glove distribution, though up to 71% of patients may be asymptomatic.1 Diagnosis is clinical, as electromyography (EMG) is frequently unremarkable or too difficult for the patient even to tolerate. Although the prevalence of this syndrome is still high despite combination antiretroviral therapy (cART), the mainstay of treatment is control of underlying HIV infection. However, several antiretroviral medications are also implicated in the development of similar conditions and should be avoided. Commonly implicated antiretrovirals include didanosine, zalcitabine, and stavudine (also known as “d drugs” for their 3-letter acronyms: ddI, ddC, and d4T), but others have been associated, as well. Treatment is otherwise largely identical to that of other neuropathic pain syndromes, although in severe cases, medications commonly used for neuropathic pain may not offer sufficient pain relief, requiring a multidisciplinary approach.
Inflammatory demyelinating polyneuropathy, mononeuropathy multiplex, and polyradiculopathies have also been described in patients with HIV having varying degrees of immune suppression but more commonly early in infection.1 Diagnosis is typically made clinically in patients with known HIV and appropriate symptoms not attributable to other causes of peripheral neuropathy, although EMG can provide supportive data by demonstrating distal axonal type degeneration.
Aside from distal peripheral neuropathies, HIV has also been associated with cranial neuropathies, particularly facial palsies, including facial diplegia. Although bilateral facial weakness is rare, its presence should raise suspicion for possible presenting HIV infection.3
Although rare and controversial, motor neuron disease has additionally been described as a complication of HIV, even as the initial manifestation of HIV infection. Although no pathologic evidence exists for virus or viral proteins being the cause of this entity, reports of cure with initiation of cART make attention to the occurrence in HIV of this otherwise fatal disease warranted.4
Human T-cell lymphotropic virus
Human T-cell lymphotropic virus (HTLV) is a human retrovirus transmitted by bodily fluids that infects T lymphocytes and is the causative agent in adult T-cell leukemia and HTLV-1-associated myelopathy/tropical spastic paraparesis (HAM/TSP). Although the number of individuals estimated to be infected with the virus is approximately 20 million, less than 5% of individuals have symptomatic neurologic disease.5 Human T-cell lymphotropic virus 1-associated myelopathy/TSP typically presents as a slowly progressive paraparesis with bladder dysfunction and sensory abnormalities. Patients have spastic weakness in lower extremities and hyperreflexia. Disease progression is faster in women for unclear reasons, particularly prior to menopause, and in patients who are immunocompromised. Diagnosis remains challenging, as up to 40% to 65% of patients in endemic regions who are suspected to have HAM/TSP are HTLV-1 seronegative.6 In addition to HAM/TSP, HTLV-1 has more recently been noted to have implications in other aspects of the nervous system. Associations with polymyositis and inclusion body myositis as well as polyneuropathies in a stocking and glove distribution with autonomic disturbances have been described.7,8 Rare reports of HTLV-1 motor neuron disease have also been reported, with lymphocytic infiltrates throughout the CNS and loss of anterior horn cells.9 Isolated cases of myasthenia gravis-like syndrome associated with HTLV-1 have also been reported in the literature.10 Treatment is supportive.
Herpes Viruses
The herpes viruses are double-stranded DNA viruses that can produce symptoms after years of lying dormant. The ability of these viruses to cause CNS disease and transverse myelitis is well documented,11 but they also impact the PNS and have been implicated in radiculopathies and cranial neuropathies. Three of these viruses, varicella-zoster virus (VZV), and herpes simplex virus types 1 and 2 (HSV-1 and HSV-2), are neurotropic and reside in neural ganglia.
Herpes simplex virus
Herpes simplex virus 1 and HSV-2 are acquired via contact with mucosal surfaces. Herpes simplex virus 1 is primarily acquired in childhood, and HSV-2 causes most cases of genital herpes, although incidence of HSV-1 causing genital herpes is rising.12 Peripheral nervous system manifestations of primary HSV infection are rare, but reactivation of the infection can lead to both CNS and PNS diseases.
Herpes simplex virus 2 has a propensity to lie dormant in sacral root ganglia and can cause a sacral radiculitis known as Elsberg syndrome.13,14 Typical presentation includes acute urinary retention, constipation, and sensory lumbosacral symptoms. Sexually active women are preferentially affected. Cerebrospinal fluid (CSF) shows a lymphocytic pleocytosis and elevated CSF protein, and HSV-2 polymerase chain reaction (PCR) from the CSF is often positive. The syndrome may be a result of reactivation of the dormant virus, as the positive HSV-2 immunoglobulin (Ig) M antibodies in the serum are not thought to indicate primary infection in this setting.14 Magnetic resonance imaging (MRI) can be normal, but in some cases may show lower spinal cord edema and hyperintensity on T2-weighted images with contrast enhancement of the sacral radicular fibers.15 Symptoms usually remit within several weeks, although antiviral treatment may shorten the symptomatic period.16 Recurrence of symptoms has been reported.17
Varicella-zoster virus
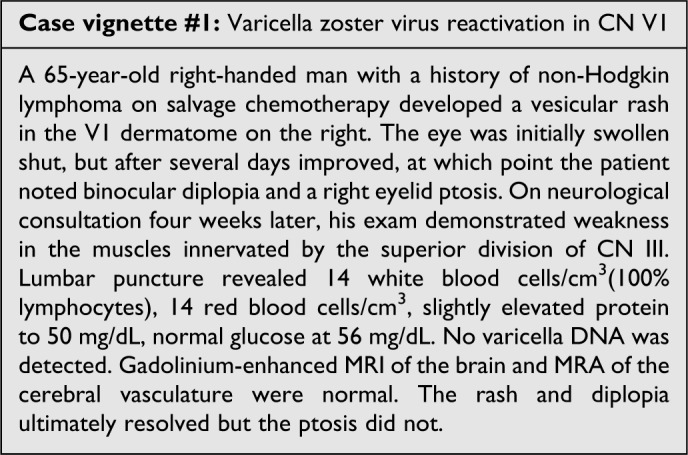
Varicella-zoster virus is the cause of varicella and herpes zoster. Primary infection with VZV typically occurs in childhood and is characterized by a viral exanthem. Guillain-Barré syndrome (GBS) is a rare complication of primary infection18 and even more rarely reported in association with herpes zoster. Reactivation of VZV occurs primarily in the elderly patients and immunosuppressed, manifesting as the dermatomal rash of shingles; rarely, the manifestation is as dermatomal pain without rash or zoster sine herpete. In the PNS, the most commonly reported complication is postherpetic neuralgia, which is a dermatomal distribution pain following shingles. It is unclear whether this syndrome is due to the persistence of the viral infection or due to damage caused to sensory ganglia. Motor neuropathy in the extremities is rare but has been reported, particularly when reactivation is in the cervical or lumbar nerve root ganglia. Weakness and sensory changes in the cranial nerves (CNs) can occur, such as weakness of the facial muscles associated with zoster otitis in the Ramsay-Hunt syndrome, sensory changes associated with CN V, or ophthalmoplegia of CN III.12 An illustration of this presentation is provided in the vignette subsequently (Figure 1). Pain may be refractory to treatment, but options for symptom relief include pregabalin, tricyclic antidepressants, gabapentin, topical lidocaine, anticonvulsants, and/or capsaicin, just as in other neuropathic pain syndromes. Diagnosis of VZV neuropathy is primarily clinical, although in challenging cases, titers of VZV IgG and IgM in the serum and CSF can be compared to assess intrathecal production of the virus.1 Varicella-zoster virus DNA in the CSF can also be tested but has low sensitivity. Vaccine is recommended for children and for adults older than 60 years of age and is the best preventive strategy for postherpetic neuralgia in the latter population, but it remains unclear how long the immunity from the zoster vaccine lasts. In immunocompetent individuals, early treatment of VZV infection is recommended with antiviral agents such as acyclovir, valacyclovir, and famciclovir for 7 days. In immunocompromised individuals or patients older than 60 years of age, therapy should be continued until all lesions have resolved. Glucocorticoids as adjunctive treatment remain controversial, with some studies showing accelerated early healing. Corticosteroid use has not been shown to reduce the incidence of postherpetic neuralgia and given the possible side effects of steroid use, it should be instituted with caution.19
Figure 1.
Cytomegalovirus
Unlike VZV and HSV, cytomegalovirus (CMV) is a lymphotrophic herpes virus. In immunocompetent patients, CMV has been associated with GBS. In an analysis of 506 patients with GBS, 12.4% were felt to have CMV-GBS, and the incidence of CMV-GBS was estimated to be 2.2 cases per 1000 cases of primary CMV infection.20 In immunosuppressed patients, CMV has been implicated in causing a myelomeningoradiculitis, mononeuritis multiplex and a painful distal neuropathy.12 The myelomeningoradiculitis is characterized by progressive lower extremity numbness and weakness as well as sphincter dysfunction, closely mimicking GBS. Indeed, EMG studies in these patients show acute denervation and abnormal spontaneous activity.21 However, pathology shows cytomegalic inclusions in Schwann cells and invasion of the cauda equina nerve roots by endoneurial fibroblasts.22 Magnetic resonance imaging may be normal but may also show enhancement of the lower spinal cord leptomeninges.21 Cerebrospinal fluid analysis is variable, with CSF pleocytosis ranging from the hundreds to thousands with a polymorphonuclear (PMN) predominance, elevated protein, and positive CMV PCR (sensitivity 92% and specificity 94%).1 Treatment is with intravenous (IV) ganciclovir and immune reconstitution, although efficacy remains uncertain and prognosis is often poor regardless. In an analysis of 13 patients with advanced HIV and presumed CMV-GBS who were treated with ganciclovir, only 1 patient regained independent ambulation and median survival was 2.7 months.21
Another syndrome associated with immunocompromise and CMV infection is mononeuritis multiplex, characterized by multifocal asymmetric sensorimotor deficits.12 This is often seen in advanced HIV infection. Biopsy may show multifocal necrotizing vasculitis of the epineural arteries with intranuclear and intracytoplasmic inclusion bodies, but the sensitivity of biopsy remains poor.23 Treatment is with ganciclovir and/or foscarnet, and some have argued for indefinite therapy in patients who are immunocompromised.24
Epstein-Barr virus
Epstein-Barr virus (EBV) is also a lymphotropic herpes virus. Infection of the PNS is rare but has been associated with GBS, acute myeloradiculitis, and encephalomyeloradiculitis. In a serologic study of 100 patients with GBS, 8 had EBV-specific IgM.25 Rare case reports of more systemic neurologic involvement of EBV in the form of a myeloradiculitis or an encephalomyeloradiculitis are also documented in the literature. Majid et al reported on 4 such cases, all of which had a CSF mononuclear predominant pleocytosis, elevated CSF protein, and EBV DNA in the CSF.26 All 4 cases received antiviral treatment with either acyclovir or ganciclovir, and 2 of the 4 cases received steroids.
Overall, it is unclear whether the neurologic manifestations of EBV are from the virus itself or from parainfectious inflammatory mechanisms. There is no definitive treatment for EBV myeloradiculitis, and antivirals have not been demonstrated to impact disease course, but the utility of immune modulation with corticosteroids and IVIg is not clear.
Flaviviridae
West Nile virus
West Nile virus (WNV) belongs to a group of RNA viruses called Flaviviruses and in the PNS, WNV has been associated with a flaccid paralysis syndrome similar to poliomyelitis. West Nile virus is transmitted by a mosquito vector and has been reported in all 48 contiguous States and Canada, with 91% of neurologic infections occurring between July and September.27 Approximately 25% of patients infected with WNV will be symptomatic, with the most common symptoms being headache, low-grade fevers, and a morbilliform or maculopapular rash. Approximately 1% of the symptomatic patients will have neuroinvasive disease, and the majority of patients with neuroinvasive disease present with encephalitis.28 Acute flaccid paralysis makes up only 3% of neuroinvasive WNV cases, but mortality is as high as 12% in these cases.27 Burton et al reviewed 26 cases of WNV in Canada and found 11 had neuromuscular disease. Of these patients, 7 had acute flaccid paralysis, with EMG showing absence of compound muscle action potentials and motor units but with fibrillation potentials, consistent with anterior horn cell involvement.29 Other patients had a rapidly progressive asymmetric flaccid paralysis involving the upper extremities and face or lower extremities, and EMG showed reduced motor amplitudes in multiple nerves, denervation, and increased F-wave latencies with normal sensory studies. Of the 11 patients, 3 had reduced motor and sensory nerve amplitudes, reduced conduction velocities, conduction block, and increased F-wave latencies, consistent with a demyelinating neuropathy with secondary axonal degeneration. Cerebrospinal fluid analysis in patients with WNV shows a PMN or mononuclear pleocytosis (mean 200 cells/μL), elevated protein, and normal glucose.11 Diagnosis is typically made by serologic testing, although serum IgG persists for many years and as such may be indicative only of prior infection. However, repeat serologies several weeks apart demonstrating at least a 4-fold increase indicate acute infection. Additionally, viral RNA in the CSF is diagnostic of acute WNV, and CSF serologies are also specific; viral RNA clears rapidly, although, and intrathecal antibodies take weeks to develop, creating a window of absence in terms of evidence of WNV infection. Treatment is supportive, as none of the treatments that have been tried, including WNV IV Ig and ribavirin, have proved effective.
Hepatitis C virus
Hepatitis C virus (HCV) is an RNA virus with a predilection for the liver and lymphocytes, although HCV has also been implicated in nervous system disease, as well. Approximately 170 million people are estimated to have HCV, and up to 50% develop cryoglobulinemia as an extrahepatic manifestation of the disease.30,31 Cryoglobulinemia refers to the presence of circulating Igs that below a certain temperature can precipitate in small blood vessels. Although some patients are asymptomatic, others may develop symptoms including arthralgias, palpable purpura, and peripheral neuropathy.32 In patients with mixed cryoglobulinemia, peripheral neuropathy is usually a moderate axonal sensory polyneuropathy. In a study of 51 patients with HCV in Italy, evidence of cryoglobulinemia was found in 78%. Electrophysiologic and histologic studies were performed in these patients, which showed that peripheral neuropathy was found in both cryoglobulinemia-positive and -negative patients, but the severity of disease, both clinically and electrophysiologically, was greater in the group with cryoglobulinemia, and polyneuropathy, as opposed to mononeuropathy, was more prevalent in the group with cryoglobulinemia. In this study, histology was consistent with a vasculitic process in both cryoglobulinemia positive and negative patients, and authors postulated that an ischemic etiology for the peripheral neuropathy could be at play.33 Others have postulated that a cytopathic or immunologic process may contribute to the peripheral neuropathy.34 Treatment of symptomatic hepatitis C was traditionally with steroids and recombinant interferon α2b; however, newer treatments have been developed and are being used in some countries. The impact of these newer medications on the PNS is still unclear, but several studies have looked at the impact of the older regimen, which utilized steroids and recombinant interferon α2b, in patients with peripheral neuropathy. In these studies, although analysis of patients soon after treatment did not show worsening of neuropathy, retrospective analysis of patients treated with this regimen at 3 and 8 years showed progression of the neuropathy despite stable cryoglobulin levels. It remains unclear whether the worsening of the neuropathy is due to the disease process itself or whether this may be an effect of treatment.35,36
Rhabdovirdiae
Rabies virus
Rabies is caused by a RNA virus that is typically transmitted by the bite of an infected animal. In the United States, human rabies is rare, with only 2 cases reported in 2010. However, worldwide, according to the US Centers for Disease Control (CDC) and the WHO, there are an estimated 55 000 deaths from rabies per year, with 95% occurring in Africa and Asia. The virus has an incubation period usually lasting from 20 to 90 days during which the virus replicates within muscle at the site of inoculation. It then binds to nicotinic acetylcholine receptors at the neuromuscular junction and travels retrograde along the peripheral nerves to dorsal root ganglia, where further replication occurs followed by rapid spread to the CNS.37 For approximately 67% of patients, presentation will be with focal weakness and pain followed by psychosis, hydrophobia, and aerophobia, with autonomic instability. The other 33% of patients will have “paralytic” rabies in which they present with an acute flaccid paralysis with rapidly progressive encephalopathy.38 Diagnosis is by PCR of the virus using samples from the saliva, hair, or nuchal skin containing hair follicles or by rabies virus antigen detection from skin biopsy at the nape of the neck. Postexposure prophylaxis with human rabies immune globulin and vaccination are recommended to prevent disease,37 but once neurological symptoms develop there is no proven therapy, and prognosis is almost invariably poor. There has been 1 reported survival after neurological symptomatology manifested, and this patient was treated with a strategy of induced coma and antivirals until natural immunity waxed, known as the Milwaukee protocol.39 This has been attempted in subsequent patients, albeit without success.
Spirochetes With Clinical Implications in the PNS
Borrelia burgdorferi
Borrelia burgdorferi, the causative agent in Lyme disease in the United States, is a spirochete transmitted by Ixodes ticks. Transmission occurs by attachment of the nymph stage tick to its host for a prolonged period, typically greater than 36 hours.40 Lyme disease is predominantly seen in Northern latitudes, with cases reported in the Eastern, Midwestern, and Western United States, as well as throughout Europe and Russia. In 2011, the CDC reported the highest incidence of Lyme in Delaware, closely followed by Vermont, New Hampshire, Maine, and Connecticut.41 In Europe, at least 5 different strains of the Borrelia bacterium are present, which cause a slightly variable disease profile.40 Infection tends to occur in the late spring and summer when ticks are in the nymph stage and more actively feeding.
The classic presentation of Lyme disease is the early development of the erythema migrans rash, a “bull’s eye”-shaped erythematous rash with central clearing, approximately 7 to 14 days after tick detachment. Arthralgias, neck pain, and headache are common features, and fevers may be present. Early reports suggested that approximately 10% of patients develop a neurologic manifestation of the infection,42 although more recent reports suggest that neurologic sequelae are less frequent.41
Within the PNS, Lyme has been reported to cause radiculopathies, cranial neuropathies, mononeuropathies, and diffuse polyneuropathies (Figure 2). Cranial neuropathies and painful radiculopathies are by far the most common and are typically seen within the first 1 to 2 months of infection,43 as described in the case vignette (Figure 3). Involvement of almost every CN has been described in case reports, with the most prevalent being CN VII.43,44 In a prospective analysis by Halperin of 74 patients with Lyme borreliosis, 3% had Bell palsy and 6% had radicular pain.45 In a study of 102 patients in Sweden with facial palsy, 34 were found to have Lyme disease.46 Bannwarth syndrome, a painful lymphocytic meningoradiculitis, has been associated with Lyme disease and is more frequently seen in Europe.43,47
Figure 2.

Polyradiculitis in acute neurological Lyme disease. Axial T1 magnetic resonance imaging of the thoracolumbar spine at the level of L1 before (left) and after (right) the administration of gadolinium demonstrate diffuse, abnormal enhancement of the lumbosacral nerve roots (arrow heads).
Figure 3.
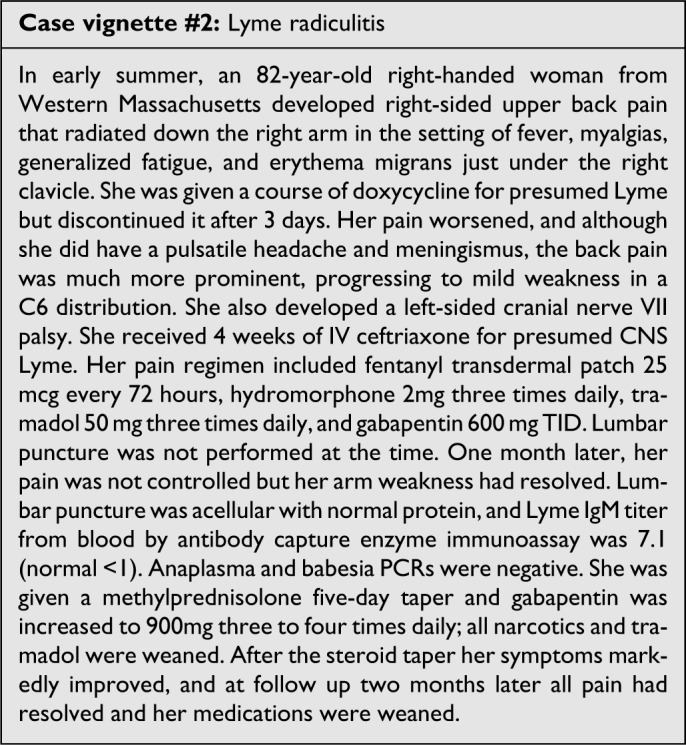
Lyme neuroborreliosis should be suspected in patients with meningitic symptoms or multiple CN palsies in endemic areas who have had a preceding rash. Serologic tests with an enzyme-linked immunosorbent assay (ELISA) and a Western blot for confirmation are typically positive at the time of presentation. In patients with peripheral neuropathy as their only symptom, routine screening for Lyme is not helpful given that testing will be positive if the patient was previously exposed to Lyme and does not indicate causality. In differentiating Lyme from aseptic meningitis, factors that have been associated with a higher likelihood of Lyme infection include lower fevers at the time of presentation, longer duration of symptoms prior to presentation, cranial neuropathy, preceding rash, and higher CSF protein.48–50 The Infectious Disease Society of America (IDSA) recommends a 2-tiered approach at diagnosis, beginning with a Lyme ELISA, which, if positive, should prompt testing for Lyme IgG and IgM in the serum if <30 days from symptom onset or Lyme IgG alone if >30 days from symptom onset. There is a high rate of false positives with Lyme IgM. Lyme PCR in the CSF has variable sensitivity and is currently not approved by the Food and Drug Administration (FDA) for diagnosis. There appears to be little evidence for relapse of Lyme disease in patients who have been infected. In a study by Nadelman et al of 22 paired consecutive episodes of erythema migrans, none of the paired episodes showed the same strain of B burgdorferi on culture, suggesting reinfection as opposed to relapse.51
According to the IDSA guidelines, treatment of localized or early, disseminated Lyme disease in the United States in the absence of neurologic manifestations can be treated with doxycycline, amoxicillin, or cefuroxime axetil for 14 days. However, in the cases of Lyme meningitis or other manifestations of early neurologic Lyme disease, recommended treatment is with IV antibiotics with ceftriaxone (2 g once/d for 14-28 days), with cefotaxime or penicillin being acceptable alternatives. For patients who are intolerant of β-lactam antibiotics, doxycycline (200-400 mg/d in 2 divided doses orally for 10-28 days) may be adequate, but evidence is insufficient. Retreatment is not recommended unless relapse is proven by objective measures, and at this time, there is no convincing evidence to support the use of long-term antibiotic therapy in patients with post-Lyme syndromes.52
Bacteria With Clinical Implications in the PNS
Campylobactor jejuni
Campylobacter jejuni is a gram-negative bacteria that has long been described to have an antecedent association with GBS, with certain subtypes, such as O:19 in the United States, carrying increased risk.53 There are multiple case–control studies that have examined the prevalence of C jejuni as an antecedent infection in patients with GBS. Estimates of C jejuni in patients with Guillain-Barré range from 20% to 40%;54,55 however, the risk of developing GBS after Campylobacter is quite low, estimated at only 1:1000.56 The mechanism by which C jejuni leads to Guillain-Barré is hypothesized to involve molecular mimicry as well as a cross-reactive immune response.53 Treatment of GBS is with IV Ig or plasmapheresis.57
Corynebacterium diphtheriae
Diphtheria, caused by the gram positive Corynebacterium diphtheriae, has been largely eliminated in countries with vaccination schedules but remains a global threat. In 2012, according to the WHO, there were 4489 reported cases of diphtheria, with 2500 deaths. Adults are particularly susceptible to diphtheria, given waning immunity in adulthood in many individuals.1 Spread is primarily via respiratory droplets, and the bacteria typically infect the pharynx and tonsils. The bacteria produce an exotoxin, which, while unable to cross the blood–brain barrier, can have deleterious effects on the PNS in up to 75% of cases, with the severity of presentation correlating with the severity of respiratory symptoms.58 Neuropathies of the CNs, particularly of the soft palate, can develop and lead to aspiration and regurgitation. Distal sensorimotor polyneuropathy can also occur secondary to paranodal and segmental myelin degeneration with late axonal degeneration.59 Diagnosis by culture is difficult, but serological tests are available. Therapy is with diphtheria antitoxin, and early treatment is critical.
Brucella spp.
Brucellosis is infection caused by Brucella bacteria, which are small, gram-negative coccobacilli. Typically, this infection is acquired via consumption of unpasteurized milk or by contact with infected animal products. Symptoms include fevers, myalgias, and arthralgias but can also include thrombocytopenia, anemia, hepatitis, and endocarditis.60 Neurologic manifestations are rare, but when they do occur can affect virtually any part of the nervous system. In the PNS, patients can develop cranial neuropathies, radiculopathies, and peripheral neuropathies. In 1 review of 154 patients with neurobrucellosis, 19% had CN involvement, with involvement of CN VIII most common, followed by CN VI and VII. Cerebrospinal fluid culture was positive in only 14% of patients, and thus serologic tests remain the most clinically useful evaluation.60 Typically, diagnosis is made clinically in patients with systemic brucellosis and neurologic symptoms. Optimal treatment of neurobrucellosis is unclear, although most regimens recommend prolonged treatment for >2 months with triple antibiotic therapy, typically ceftriaxone, rifampin, and doxycycline.61
Clostridium botulinum
Clostridium botulinum is a spore-forming anaerobic, gram-positive bacterium with an ability to produce neurotoxins. Although there are 7 different types of neurotoxins produced, all act under a similar mechanism, binding irreversibly to presynaptic nerve endings in the PNS and thus inhibiting release of acetylcholine.62 Botulism can occur as foodborne botulism, wound botulism, infant botulism, and as a potential bioterrorism agent. Symptoms represent cholinergic blockade, with nausea, constipation, dry mouth, and diplopia. If untreated, this can then be followed by a symmetric descending paralysis, starting with the CNs, then affecting the upper extremities, respiratory muscles, and lower extremities. Sensory systems are unaffected. Cerebrospinal fluid is normal, helping to differentiate botulism from GBS, and the edrophonium chloride test, used in myasthenia gravis, is also negative.63 If there is a high suspicion for botulism, confirmatory tests include mouse inoculation and stool culture through the CDC. Treatment is with mechanical ventilation and antitoxin.
Mycobacteria With Clinical Implications in the PNS
Mycobacterium tuberculosis
Tuberculosis (TB) is caused by Mycobacterium tuberculosis, a bacillus that typically infects the lungs but can spread to the nervous system. According to the WHO 2012 report, there were almost 9 million new cases of TB in 2011. Estimates of nervous system involvement of TB range from 1% to 10% of cases with TB.64,65
Tuberculosis has been associated with basilar leptomeningitis, pachymeningitis, tuberculomas, and myelitis.11,65 Cranial nerve palsies are a common complication of tuberculous meningitis, with CN VI being the most frequently involved, although involvement of multiple CNs can occur. In a study done on 158 patients with TB meningitis in India, 38% had CN involvement and 10% had involvement of 2 or more CNs.66 Aside from CN dysfunction, TB involvement of the spinal cord in Potts disease can lead to myelitis and to radicular symptoms.67 Diagnosis of TB in the nervous system remains challenging, as yield from acid-fast bacilli (AFB) stain or culture from the CSF is low.68 Treatment of TB including CNS TB involves a 4-drug regimen with rifampin, isoniazid, pyrazinamide, and ethambutol for 2 months followed by 7 to 10 months of isoniazid and rifampin. Data on steroids remain uncertain, with most studies indicating that patients who are not infected with HIV should be given a regimen that includes dexamethasone.68
Mycobacterium leprae
Leprosy has long been known to have effects on the PNS. It is caused by the AFB Mycobacterium leprae. In the United States, few cases of endemic leprosy have been reported, but cases in Texas and Louisiana have occurred, with possible transmission from infected armadillos. Typical route of transmission of the disease is thought to be through nasal droplet infection, although this has not been definitively proven.69 The bacillus has a predilection for Schwann cells, but damage to the PNS can also occur through an immune-mediated response.70 Typical presentation is with a mononeuropathy or a symmetric polyneuropathy. The disease is classified on a spectrum of the patient’s immune response, ranging from tuberculoid leprosy (paucibacillary), in which the patient mounts a strong cell-mediated immune response to the disease, to lepromatous (multibacillary), in which the patients are only able to mount a low cell-mediated immune response to the disease. Lepromatous leprosy tends to have late presentation of neural lesions, at which point patients develop bilateral symmetrical distal neuropathies. Histology shows relative preservation of nerve architecture with foamy cells in the perineum of nerves and numerous bacilli. Borderline leprosy can have multiple nerves involved, with more rapid nerve involvement than in lepromatous leprosy. Tuberculoid leprosy tends to present with asymmetrical nerve enlargement, usually proximal to the skin lesions, and histology shows destruction of nerve architecture with granulomas in nerves.70,71 Reaction syndromes can occur wherein patients have flares in cell-mediated immune response (type 1 reaction) or flares in systemic inflammatory response to large amounts of antibody–antigen complexes (type 2 reaction).1 Diagnosis of leprosy is primarily by the presence of 1 of the 3 factors: anesthetic skin lesions, enlarged peripheral nerves, and AFB on biopsy. Approximately 10% of patients have pure neural leprosy, in which peripheral neuropathy occurs in the absence of skin lesions. Electromyography shows prolongation of distal latencies and segmental slowing of conduction velocities early in the disease, and later disease can show increased insertional activity and polyphasic, large-amplitude, and long-duration motor units with reduced recruitment.70 Serologic tests with phenolic glycolipid 1 have low sensitivity in some forms of leprosy and thus use remains limited to certain situations. Gold standard is with histological diagnosis.72 Treatment depends on the number of lesions and whether or not presentation is paucibacillary or multibacillary and includes a multidrug regimen with dapsone, rifampin, ofloxacin, minocycline, or clofazimine depending on classification. Steroids have been shown to aid in neural recovery, although optimal dose and duration remain under study.73 Additionally, immunosuppressants may be needed in type 1 reactions, and thalidomide may be needed for type 2 reactions.
Parasites With Clinical Implications in the PNS
Chagas Disease
Chagas disease is caused by the parasite Trypanosoma cruzi and is transmitted by insects that feed off the blood of humans. It is found in South America, Central America, and southern parts of North America. Acute infection is typically asymptomatic, but at 20 to 40 days after infection, fever, enlargement of the liver and lymph nodes, and subcutaneous edema can develop. The chronic infection is associated with degeneration of the ganglia of the autonomic nervous system, leading to megacolon, megaesophagus, and cardiac abnormalities, all of which can develop 10 to 30 years after initial infection.74 Additionally, sensory peripheral neuropathy may be associated with the disease, as demonstrated by a study of patients with trypanosomiasis by Genovese et al.75 The mechanism by which Chagas disease causes autonomic nervous system pathology is debated, although some studies have suggested binding of autoantibodies to the nicotinic acetylcholine receptor and others have suggested a direct effect of the parasitemia.74,76 Diagnosis of chronic Chagas disease is based on detection of IgG antibodies to T cruzi antigens. Treatment of acute infection is with benznidazole and nifurtimox, but the benefit of treatment in patients with chronic Chagas remains unclear.74
Complications of Treatment With Antibiotics and Antivirals
Unfortunately, numerous agents used to treat infections may have untoward side effects that manifest in the PNS. These are mostly associated with length-dependent small fiber neuropathies, and many medications have been implicated.
An FDA warning was published in 2013 to warn against the development of peripheral neuropathy with fluoroquinolone antibiotics. It is not clear how often this occurs or which patients are at risk.77 Symptoms are typically of a distal, symmetric, burning pain starting in the soles of the feet and ascending in a length-dependent fashion. The medication should be substituted with another suitable antibiotic to prevent further damage. Treatment is otherwise supportive with neuropathic pain medication often as first-line therapy, but pain control can be difficult.
Although the risk of peripheral neuropathy from fluoroquinolones is newly recognized, isoniazid, used in the treatment and prevention of TB, has long been known to be associated with a peripheral neuropathy. The neuropathy develops secondary to isoniazid-related antagonism of pyridoxine (vitamin B6), leading to axonal degeneration. One large study of 24 221 patients in South Africa found that 0.21% of patients treated with isoniazid developed a peripheral neuropathy, but other studies suggested rates of 2% to 10% depended on the dose given.78 Rapid removal of the drug or preventive treatment with vitamin B6 can help to reduce the chance of long-term impairment. Aside from isoniazid, other anti-TB medications have effects on the PNS. Optic neuropathy has been associated with ethambutol, and aminoglycosides can induce neuromuscular blockade in select patients and thus should particularly be avoided in patients with myasthenia gravis.
Treatment of HIV requires use of multiple antiretroviral agents, some of which have side effects on the PNS. The toxicity of these agents is mostly related to mitochondrial toxicity. As such, the dideoxynucleoside agents such as didanosine, zalcitabine, and stavudine are considered the most toxic to the nervous system among HIV treatment modalities. Zidovudine has been implicated quite commonly, as well. The neuropathy usually begins several months after antiretroviral therapy begun, and treatment is with substitution of the offending medication and supportive care. Distinguishing this syndrome from the distal symmetric neuropathy associated with HIV can be challenging and is usually based on the temporal relationship of the symptoms with beginning treatment. Stavudine is also associated with a Guillain-Barré-like syndrome deemed HIV-associated neuromuscular weakness syndrome, which typically presents with lactic acidosis.2
Finally, linezolid has garnered significant attention for neuropathy associated with its use. This also typically presents as burning pain in the soles of the feet that spreads proximally with continued exposure. The majority of cases described in the literature have been in patients who were treated for greater than 28 days with the antibiotic, as demonstrated in the vignette (Figure 4). The frequency of this side effect is not known, and symptoms may improve or at least arrest after discontinuation of the drug.79
Figure 4.

Conclusion
Despite their relative rarity, affectations of the PNS by infectious diseases represent a potentially treatable group of diseases. Although commonly associated with other manifestations of infection, these entities may occur independently and as such a high index of suspicion and early initiation of definitive treatment may preempt long-term sequelae. Additionally, adjunctive use of immune modulation may, in select cases, improve outcomes. However, for most diseases, further clinical studies are warranted to optimize outcomes of infectious PNS disease. Finally, a cautionary point is that use of some antimicrobial agents may actually prompt similar PNS diseases, and early cessation of offending medications is the best intervention to arrest nervous system damage.
Footnotes
Declaration of Conflicting Interests: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
References
- 1. Estanislao L, Hart P, Simpson D. HIV neuropathy and selected infectious neuropathies. Continuum. 2003;9 (6):118–145 [Google Scholar]
- 2. Kranick SM, Nath A. Neurologic complications of HIV-1 infection and its treatment in the era of antiretroviral therapy. Contin Lifelong Learn Neurol. 2012;18 (6):1319–1337 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Abboud O, Saliba I. Isolated bilateral facial paralysis revealing AIDS: a unique presentation. Laryngoscope. 2008;118 (4):580–584 [DOI] [PubMed] [Google Scholar]
- 4. Lyons J, Venna N, Cho T. A typical nervous system manifestations of HIV. Semin Neurol. 2011;31 (3):254–265 [DOI] [PubMed] [Google Scholar]
- 5. Goncalves DU, Proietti FA, Ribas JGR, et al. Epidemiology, treatment, and prevention of human T-cell leukemia virus type 1-associated diseases. Clin Microbiol Rev. 2010;23 (3):577–589 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Araujo AQ, Silva MTT. The HTLV-1 neurological complex. Lancet Neurol. 2006;5 (12):1068–1076 [DOI] [PubMed] [Google Scholar]
- 7. Nascimento O, Marques W. Human T-cell leukemia virus (HTLV)-associated neuropathy. Handb Clin Neurol. 2013;115:531–541 [DOI] [PubMed] [Google Scholar]
- 8. Gabbai AA, Wiley CA, Oliveira AS, et al. Skeletal muscle involvement in tropical spastic paraparesis/HTLV-1-associated myelopathy. Muscle Nerve. 1994;17 (8):923–930 [DOI] [PubMed] [Google Scholar]
- 9. Silva MTT, Leite ACC, Alamy AH, Chimelli L, Andrada-Serpa MJ, Araujo AQC. ALS syndrome in HTLV-I infection. Neurology. 2005;65 (8):1332–1333 [DOI] [PubMed] [Google Scholar]
- 10. Lalive PH, Allali G, Truffert A. Myasthenia gravis associated with HTLV-I infection and atypical brain lesions. Muscle Nerve. 2007;35 (4):525–528 [DOI] [PubMed] [Google Scholar]
- 11. Cho T, Vaitkevicius H. Infectious myelopathies. Contin Lifelong Learn Neurol. 2012;18 (6):1392–1416 [DOI] [PubMed] [Google Scholar]
- 12. Steiner I. Herpes virus infection of the peripheral nervous system. Peripheral Nerve Disorders. 2013;115:543–558 [DOI] [PubMed] [Google Scholar]
- 13. Elsberg CA. Experiences in spinal surgery: observation upon 60 laminectomies for spinal disease. Surg Gynecol Obstet. 1931;16:117–135 [Google Scholar]
- 14. Eberhardt O, Kuker W, Dichgans J, Weller M. HSV-2 sacral radiculitis (Elsberg syndrome). Neurology. 2004;63 (4):758–759 [DOI] [PubMed] [Google Scholar]
- 15. Ellie E, Rozenberg F, Dousset V, Beylot-Barry M. Herpes simplex virus type 2 ascending myeloradiculitis: MRI findings and rapid diagnosis by the polymerase chain method. J Neurol Neurosurg Psychiatry. 1994;57 (7):869–870 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Krishna A, Devulapally P, Ghobrial I. Meningitis retention syndrome. J Community Hosp Intern Med Perspect. 2012;2 (1):1–3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Aurelius E, Forsgren M, Gille E, Skoldenberg B. Neurologic morbidity after herpes simplex type 2 meningitis: a retrospective study of 40 patients. Scand J Infect Dis. 2002;34:278–283 [DOI] [PubMed] [Google Scholar]
- 18. Cresswell F, Eadie J, Longley N, Macallan D. Severe Guillain–Barré syndrome following primary infection with varicella zoster virus in an adult. Int J Infect Dis. 2010;14 (2):e161–e163 [DOI] [PubMed] [Google Scholar]
- 19. Solomon CG, Cohen JI. Herpes zoster. N Engl J Med. 2013;369 (3):255–263 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Orlikowski D, Porcher R, Sivadon-Tardy V, et al. Guillain-Barre syndrome following primary cytomegalovirus infection: a prospective cohort study. Clin Infect Dis. 2011;52 (7):837–844 [DOI] [PubMed] [Google Scholar]
- 21. So YT, Olney RK. Acute lumbosacral polyradiculopathy in acquired immunodeficiency syndrome: experience in 23 patients. Ann Neurol. 1994;35 (1):53–58 [DOI] [PubMed] [Google Scholar]
- 22. Behar R, Wiley C, McCutchan J. Cytomegalovirus polyradiculoneuropathy in acquired immune deficiency syndrome. Neurology. 1987;37 (4):557–561 [DOI] [PubMed] [Google Scholar]
- 23. Roullet E, Assuerus V, Gozlan J, et al. Cytomegalovirus multifocal neuropathy in AIDS analysis of 15 consecutive cases. Neurology. 1994;44 (11):2174–2174 [DOI] [PubMed] [Google Scholar]
- 24. Kim Y, Hollander H. Polyradiculopathy due to cytomegalovirus: report of two cases in which improvement occurred after prolonged therapy and review of the literature. Clin Infect Dis. 1993;17 (1):32–37 [DOI] [PubMed] [Google Scholar]
- 25. Dowling PC, Cook SD. Role of infection in Guillain-Barré syndrome: laboratory confirmation of herpes viruses in 41 cases. Ann Neurol. 1981;9 (suppl):44–55 [DOI] [PubMed] [Google Scholar]
- 26. Majid A, Galetta S, Sweeney C, et al. Epstein-Barr virus myeloradiculitis and encephalomyeloradiculitis. Brain. 2002;125 (pt 1):159–165 [DOI] [PubMed] [Google Scholar]
- 27. Lindsey NP, Staples JE, Lehman JA, Fischer M. Surveillance for human west Nile virus disease—United States, 1999-2008. MMWR Surveill Summ. 2010;59 (2):1–17 [PubMed] [Google Scholar]
- 28. Petersen LR. West Nile virus: review of the literature. JAMA. 2013;310 (3):308–315 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Burton JM, Kern RZ, Halliday W, et al. Neurological manifestations of West Nile virus infection. Can J Neurol Sci. 2003;31 (2):185–193 [DOI] [PubMed] [Google Scholar]
- 30. Monaco S, Ferrari S, Gajofatto A, Zanusso G, Mariotto S. HCV-related nervous system disorders. Clin Dev Immunol. 2012;2012:1–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Cacoub P, Saadoun D, Limal N, Leger JM, Maisonobe T. Hep C virus infection and mixed cryoglobulinaemia vasculitis: a review of neurological complications. AIDS. 2005;19 (suppl 3):S128–S134 [DOI] [PubMed] [Google Scholar]
- 32. Mayo MJ, Kaplan NM, Palmer BF. Extrahepatic manifestations of hepatitis C infection. Am J Med Sci. 2003;325 (3):135–148 [DOI] [PubMed] [Google Scholar]
- 33. Nemni R, Sanvito L, Quattrini A, Santuccio G, Camerlingo M, Canal N. Peripheral neuropathy in hepatitis C virus infection with and without cryoglobulinaemia. J Neurol Neurosurg Psychiatry. 2003;74 (9):1267–1271 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Bonetti B, Scardoni M, Monaco S, Rizzuto N, Scarpa A. Hepatitis C virus infection of peripheral nerves in type II cryoglobulinaemia. Virchows Arch. 1999;434 (6):533–535 [DOI] [PubMed] [Google Scholar]
- 35. Briani C, Chemello L, Zara G, et al. Peripheral neurotoxicity of pegylated interferon alpha: a prospective study in patients with HCV. Neurology. 2006;67 (5):781–785 [DOI] [PubMed] [Google Scholar]
- 36. Ammendola A, Sampaolo S, Ambrosone L, et al. Peripheral neuropathy in hepatitis-related mixed cryoglobulinemia: electrophysiologic follow-up study. Muscle Nerve. 2005;31 (3):382–385 [DOI] [PubMed] [Google Scholar]
- 37. Jackson AC. Rabies. Neurol Clin. 2008;26 (3):717–726 [DOI] [PubMed] [Google Scholar]
- 38. Hemachudha T, Ugolini G, Wacharapluesadee S, Sungkarat W, Shuangshoti S, Laothamatas J. Human rabies: neuropathogenesis, diagnosis, and management. Lancet Neurol. 2013;12 (5):498–513 [DOI] [PubMed] [Google Scholar]
- 39. Willoughby RE, Jr, Tieves KS, Hoffman GM, et al. Survival after treatment of rabies with induction of coma. N Engl J Med. 2005;352 (24):2508–2514 [DOI] [PubMed] [Google Scholar]
- 40. Stanek G, Wormser GP, Gray J, Strle F. Lyme borreliosis. Lancet. 2012;379 (9814):461–473 [DOI] [PubMed] [Google Scholar]
- 41. Gerber MA, Shapiro ED, Burke GS, Parcells VJ, Bell GL. Lyme disease in children in southeastern Connecticut. N Engl J Med. 1996;335 (17):1270–1274 [DOI] [PubMed] [Google Scholar]
- 42. Steere A. Lyme disease. N Engl J Med. 1989;321 (9):586–596 [DOI] [PubMed] [Google Scholar]
- 43. Halperin JJ. Lyme disease and the peripheral nervous system. Muscle Nerve. 2003;28 (2):133–143 [DOI] [PubMed] [Google Scholar]
- 44. Clark J, Carlson RD, Sasaki CT, Pachner AR, Steere AC. Facial paralysis in Lyme disease. Laryngoscope. 1985;95 (11):1341–1345 [PubMed] [Google Scholar]
- 45. Halperin J. Lyme neuroborreliosis. Peripheral nervous system manifestations. Brain. 1990;113 (4):1207–1221 [DOI] [PubMed] [Google Scholar]
- 46. Bremell D, Hagberg L. Clinical characteristics and cerebrospinal fluid parameters in patients with peripheral facial palsy caused by Lyme neuroborreliosis compared with facial palsy of unknown origin (Bell’s palsy). BMC Infect Dis. 2011;11(1):1–6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Pfister HW, Einhäupl K, Preac-Mursic V, Wilske B, Schierz G. The spirochetal etiology of lymphocytic meningoradiculitis of Bannwarth (Bannwarth’s syndrome). J Neurol. 1984;231 (3):141–144 [DOI] [PubMed] [Google Scholar]
- 48. Eppes SC, Nelson DK, Lewis LL, Klein JD. Characterization of Lyme meningitis and comparison with viral meningitis in children. Pediatrics. 1999;103 (5):957–960 [DOI] [PubMed] [Google Scholar]
- 49. Tuerlinckx D, Bodart E, Jamart J, Glupczynski Y. Prediction of Lyme meningitis based on a logistic regression model using clinical and cerebrospinal fluid analysis: a European study. Pediatr Infect Dis J. 2009;28 (5):394–397 [DOI] [PubMed] [Google Scholar]
- 50. Shah SS, Zaoutis TE, Turnquist J, Hodinka RL, Coffin SE. Early differentiation of Lyme from enteroviral meningitis. Pediatr Infect Dis J. 2005;24 (6):542–545 [DOI] [PubMed] [Google Scholar]
- 51. Nadelman RB, Hanincová K, Mukherjee P, et al. Differentiation of reinfection from relapse in recurrent Lyme disease. N Engl J Med. 2012;367 (20):1883–1890 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52. Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the infectious diseases society of America. Clin Infect Dis. 2006;43 (9):1089–1134 [DOI] [PubMed] [Google Scholar]
- 53. Nyati KK, Nyati R. Role of Campylobacter jejuni infection in the pathogenesis of Guillain-Barré syndrome: an update. Biomed Res Int. 2013;2013:1–13 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Rees JH, Soudain SE, Gregson NA, Hughes RA. Campylobacter jejuni infection and Guillain–Barré syndrome. N Engl J Med. 1995;333 (21):1374–1379 [DOI] [PubMed] [Google Scholar]
- 55. Mishu B, Ilyas AA, Koski CL, et al. Serologic evidence of previous Campylobacter jejuni infection in patients with the Guillain-Barré syndrome. Ann Intern Med. 1993;118 (12):947–953 [DOI] [PubMed] [Google Scholar]
- 56. Van Doorn PA, Ruts L, Jacobs BC. Clinical features, pathogenesis, and treatment of Guillain-Barré syndrome. Lancet Neurol. 2008;7 (10):939–950 [DOI] [PubMed] [Google Scholar]
- 57. Hughes RA, Swan AV, van Doorn PA. Intravenous immunoglobulin for Guillain-Barré syndrome. In: The Cochrane Collaboration, Hughes RA, eds. Cochrane Database of Systematic Reviews. Chichester, UK: John Wiley & Sons, Ltd; 2012;7 [DOI] [PubMed] [Google Scholar]
- 58. Hadfield TL, McEvoy P, Polotsky Y, Tzinserling VA, Yakovlev AA. The pathology of diphtheria. J Infect Dis. 2000;181 (suppl 1):S116–S120 [DOI] [PubMed] [Google Scholar]
- 59. Cléange A, Meyrignac C, Roualdes B, Degos JD, Gherardi RK. Diphtheritic neuropathy. Muscle Nerve. 1995;18 (12):1460–1463 [DOI] [PubMed] [Google Scholar]
- 60. Gul HC, Erdem H, Bek S. Overview of neurobrucellosis: a pooled analysis of 187 cases. Int J Infect Dis. 2009;13 (6):e339–e343 [DOI] [PubMed] [Google Scholar]
- 61. Guven T, Ugurlu K, Ergonul O, et al. Neurobrucellosis: clinical and diagnostic features. Clin Infect Dis. 2013;56 (10):1407–1412 [DOI] [PubMed] [Google Scholar]
- 62. Shapiro RL, Hatheway C, Swerdlow DL. Botulism in the United States: a clinical and epidemiologic review. Ann Intern Med. 1998;129 (3):221–228 [DOI] [PubMed] [Google Scholar]
- 63. Sobel J. Botulism. Clin Infect Dis. 2005;41 (8):1167–1173 [DOI] [PubMed] [Google Scholar]
- 64. Dye C. Global burden of tuberculosis: estimated incidence, prevalence, and mortality by country. JAMA. 1999;282 (7):677–686 [DOI] [PubMed] [Google Scholar]
- 65. Phypers M, Harris T, Power C. CNS tuberculosis: a longitudinal analysis of epidemiological and clinical features. Int J Tuberc Lung Dis. 2006;10 (1):99–103 [PubMed] [Google Scholar]
- 66. Sharma P, Garg RK, Verma R, Singh MK, Shukla R. Incidence, predictors and prognostic value of cranial nerve involvement in patients with tuberculous meningitis: a retrospective evaluation. Eur J Intern Med. 2011;22 (3):289–295 [DOI] [PubMed] [Google Scholar]
- 67. Le Page L, Feydy A, Rillardon L, et al. Spinal tuberculosis: a longitudinal study with clinical, laboratory, and imaging outcomes. Semin Arthritis Rheum. 2006;36 (2):124–129 [DOI] [PubMed] [Google Scholar]
- 68. Thwaites GE, Hien TT. Tuberculous meningitis: many questions, too few answers. Lancet Neurol. 2005;4 (3):160–170 [DOI] [PubMed] [Google Scholar]
- 69. Rodrigues LC, Lockwood DN. Leprosy now: epidemiology, progress, challenges, and research gaps. Lancet Infect Dis. 2011;11 (6):464–470 [DOI] [PubMed] [Google Scholar]
- 70. Ooi W, Shrinivasan J. Leprosy and the peripheral nervous system. Muscle Nerve. 2004;30 (4):393–409 [DOI] [PubMed] [Google Scholar]
- 71. Agrawal A, Pandit L, Dalal M, Shetty JP. Neurological manifestations of Hansen’s disease and their management. Clin Neurol Neurosurg. 2005;107 (6):445–454 [DOI] [PubMed] [Google Scholar]
- 72. Britton WJ, Lockwood D. Leprosy. Lancet. 2004;363 (9416):1209–1219 [DOI] [PubMed] [Google Scholar]
- 73. Wagenaar I, Brandsma W, Post E, et al. Two randomized controlled clinical trials to study the effectiveness of prednisolone treatment in preventing and restoring clinical nerve function loss in leprosy: the TENLEP study protocols. BMC Neurol. 2012;12 (1):159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74. Rassi A, Rassi A, Marcondes de Rezende J. American trypanosomiasis (Chagas disease). Infect Dis Clin North Am. 2012;26 (2):275–291 [DOI] [PubMed] [Google Scholar]
- 75. Genovese O, Ballario C, Storino R, Segura E, Sica RE. Clinical manifestations of peripheral nervous system involvement in human chronic Chagas disease. Arq Neuropsiquiatr. 1996;54 (2):190–196 [DOI] [PubMed] [Google Scholar]
- 76. Goin JC, Venera G, Bonino M, Sterin-Borda L. Circulating antibodies against nicotinic acetylcholine receptors in chagasic patients. Clin Exp Immunol. 1997;110 (2):219–225 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77. Kuehn B. FDA warning and study highlight fluoroquinolone risks. JAMA. 2013;310 (10):1014. [DOI] [PubMed] [Google Scholar]
- 78. Kass JS, Shandera WX. Nervous system effects of antituberculosis therapy. CNS Drugs. 2010;24 (8):655–667 [DOI] [PubMed] [Google Scholar]
- 79. Rho J, Sia I, Crum B, Dekutoski M, Trousdale R. Linezolid-associated peripheral neuropathy. Mayo Clin Proc. 2004;79 (7):927–930 [DOI] [PubMed] [Google Scholar]