

Successful management of endoscopic retrograde cholangiopancreatography (ERCP)-related duodenal perforations, up to 20 mm, has been reported using several endoscopic devices [Von Renteln et al. 2010; Buffoli et al. 2012; Dogan et al. 2013; Donatelli et al. 2013; Meduri et al. 2014], however, surgery remains the standard of care management of larger defects [Wu et al. 2006; Lee et al. 2013]. Here we report, to the best of the authors’ knowledge, the first case of successful treatment of a large duodenal perforation (>20 mm) during ERCP, using several Ovesco clips.
A 66-year-old white man was addressed for biliary drainage due to important cholestasis secondary to a liver metastatic lesion of an urothelial cancer treated by surgery and chemotherapy.
During ERCP and while delivering the third plastic 10F stent (Figure 1) a movement of the endoscope provoked a large retroperitoneal duodenal perforation occupying 1/3 of the duodenal wall (Figure 2), opposite to the papilla at the early beginning of second duodenum. The size of perforation was important, mostly because the duodenal wall is thin and injury provoked a mucosal laceration with tearing of the wall. The decision to deliver a plastic stent instead of a metal one was taken given the poor prognosis of the patient, and namely because the stenosis was evaluated as ‘Bismuth IV’, and in the case of no improvement of liver function tests, a radiological percutaneous transhepatic approach would be compromised. Then the duodenoscope together with the partially delivered stent were immediately retrieved. A standard gastroscope loaded with an 11t Ovesco (OTSC®; Ovesco Endoscopy GmbH, Tübingen, Germany), under CO2 insufflation, was introduced but unfortunately the duodenal tear was too large, both in length and width, making it impossible to aspirate both edges of the tear in the cap or approach using a Twin Grasper®. A coloscope loaded with a 14t Ovesco was subsequently introduced and endoscopic suturing was started between the greater omentum and one edge of the duodenal tear (Figure 3). Since a closure defect persisted at the other end as shown after contrast-medium injection (Figure 4), the gastric Ovesco was delivered while aspirating the omentum incarcerated between the first colic clip and the free edge of the perforation, achieving full closure without contrast-medium extravasation (Figure 5). A nasogastric tube was left in place in soft aspiration. The patient was then transferred to the intensive care unit (ICU), for surveillance, where he remained for 7 days before being discharged. During his stay in the ICU, no fever was detected, the liver function tests were improved, and no further ERCP was needed to add the third stent. We only noticed a transient rise of the C-reactive protein, before its complete normalization, and CT scan as well as water-soluble contrast upper-studies performed on days 2 and 5 postoperatively were normal (Figure 6). Oral nutrition was started on day 6. At 1 month after endoscopy, the patient is fully asymptomatic.
Figure 1.

Hilar stenosis with 2 plastic stents in place. The guidewire in the left duct is about be placed, in order to deliver the third stent.
Figure 2.
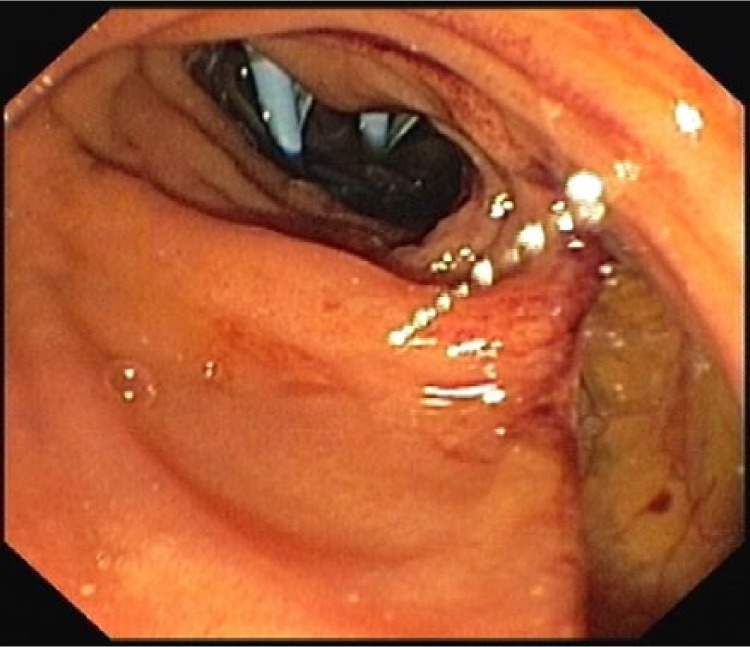
Large duodenal defect.
Figure 3.

Colic clip Ovesco in place incarcerating greater omentum.
Figure 4.

Contrast-medium extravasation at the one end of the duodenal perforation despite colic Ovesco placement, given the large size of the defect.
Figure 5.
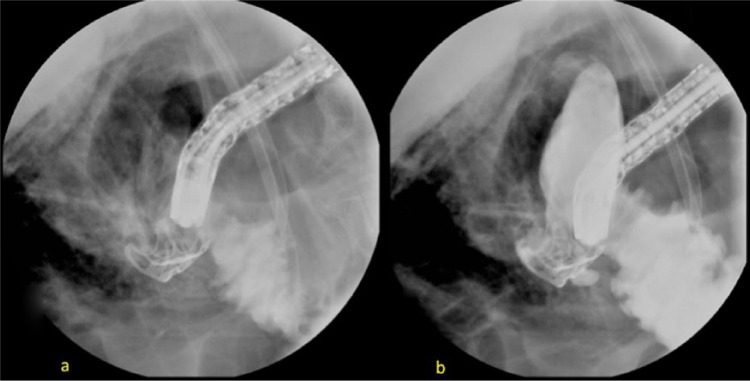
Watertight closure achieved using a ‘bridge technique’ using Ovesco on Ovesco.
Figure 6.
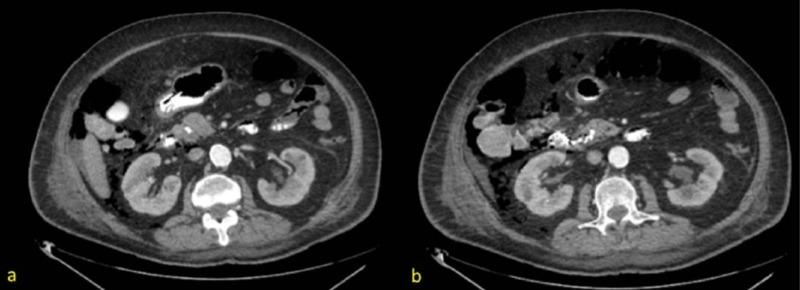
CT scan showing clips in place with no extravasation of contrast medium.
In conclusion OTSC is a surgery-sparing device, and colic and gastric clips together can be a useful tool for the closure of large duodenal defects. However, the use of a colic Ovesco should be considered too, mainly because of its size, for upper gastrointestinal interventions in an expert’s hands.
Footnotes
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement: The authors have no conflicts of interest to declare.
Contributor Information
Gianfranco Donatelli, Unité d’Endoscopie Interventionnelle, Hôpital Privé des Peupliers, Générale de Santé, 8 Place de l’Abbé G. Hénocque 75013, Paris, France.
Jean-Loup Dumont, Unité d’Endoscopie Interventionnelle, Hôpital Privé des Peupliers, Générale de Santé, Paris, France.
Bertrand Marie Vergeau, Unité d’Endoscopie Interventionnelle, Hôpital Privé des Peupliers, Générale de Santé, Paris, France.
Renaud Chiche, Service de Chirurgie Viscérale et Digestive, Clinique Geoffroy Saint-Hilaire, Générale de Santé, Paris, France.
Jean-Jacques Quioc, Service de Gastro-entérologie, Hôpital Privé de l’Ouest Parisien, Générale de Santé, Trappes, France.
Thierry Tuszynski, Unité d’Endoscopie Interventionnelle, Hôpital Privé des Peupliers, Générale de Santé, Paris, France.
Bruno Meduri, Unité d’Endoscopie Interventionnelle, Hôpital Privé des Peupliers, Générale de Santé, Paris, France.
References
- Buffoli F., Grassia R., Iiritano E., Bianchi G., Dizioli P., Staiano T. (2012) Endoscopic “retroperitoneal fatpexy” of a large ERCP-related jejunal perforation by using a new over-the-scope clip device in Billroth II anatomy (with video). Gastrointest Endosc 75: 1115–1117 [DOI] [PubMed] [Google Scholar]
- Dogan U., Keskin M., Soker G., Akin M., Yalaki S. (2013) Endoscopic closure of an endoscope-related duodenal perforation using the over-the-scope clip. Turk J Gastroenterol 24: 436–440 [DOI] [PubMed] [Google Scholar]
- Donatelli G., Vergeau B., Dritsas S., Dumont J., Tuszynski T., Meduri B. (2013) Closure with an over-the-scope clip allows therapeutic ERCP to be safely performed after acute duodenal perforation during diagnostic endoscopic ultrasound. Endoscopy 45(Suppl. 2 UCTN): E392–E393 [DOI] [PubMed] [Google Scholar]
- Lee T., Han J., Park S. (2013) Endoscopic treatments of endoscopic retrograde cholangiopancreatography-related duodenal perforations. Clin Endosc 46: 522–528 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meduri B., Vergeau B., Dumont J., Tuszynski T., Dritsas S., Dhumane P., et al. (2014) Endoscopic ultrasound-guided fine needle aspiration and endoscopic biliary drainage following closure of a duodenal perforation with an over-the-scope clip. Endoscopy 46(Suppl. 1 UCTN): E69–E70 [DOI] [PubMed] [Google Scholar]
- Von Renteln D., Rudolph H., Schmidt A., Vassiliou M., Caca K. (2010) Endoscopic closure of duodenal perforations by using an over-the-scope clip: a randomized, controlled porcine study. Gastrointest Endosc 71: 131–138 [DOI] [PubMed] [Google Scholar]
- Wu H., Dixon E., May G., Sutherland F. (2006) Management of perforation after endoscopic retrograde cholangiopancreatography (ERCP): a population-based review. HPB (Oxford) 8: 393–399 [DOI] [PMC free article] [PubMed] [Google Scholar]