

Introduction
Patients often struggle to understand written medication instructions and management points due to the complexity of the information.1 As shown in a study conducted at 2 urban public hospitals, approximately 42% of patients were unable to understand written medication instructions.2 Patients with type 2 diabetes mellitus are particularly susceptible to this problem, as most are on more than one medication and are also encouraged to increase their self-management of this chronic condition. Misunderstanding medications and poor compliance with diabetes management can result in unfavourable outcomes.3-5
Since patient information on diabetes is mainly available in text format, it is important to develop counselling tools to enhance patient-provider communication. Pictograms have the ability to overcome communication barriers and provide simple yet necessary information. Numerous studies have shown that pictograms may improve medication safety, medication compliance and overall health outcomes in the general public.6,7
Pictograms have also been shown to increase the short- and long-term (after 4 weeks) memory of complex medical instructions in patients, especially when the printed information is presented along with verbal information.8,9 According to Paivio’s dual coding theory,10 the verbal system and nonverbal system work in association, and the activation of one system triggers the activation of the other. This suggests that pictures have the ability to further activate the understanding of verbal information, therefore optimizing information interpretation and message recollection.10 The use of pictorial aids such as illustrations can make health education literature more accessible, while remaining interesting enough to appeal to individuals at all levels of reading ability.11 The use of pictograms in patient information leaflets is preferred by patients and significantly improves their understanding of the material presented.12
The use of pictographic counselling tools for diabetic patients is meant to supplement written and oral information for those people who are limited in their ability to read. Difficulties in processing written instructions may be attributed to age, low literacy and comorbidities such as retinopathy. Pictograms and pictographic symbols should only use those details that are most important and provide the most information. The purpose is to lead the patient in the right direction by using symbols that build on the most characteristic concepts of reality,13 just as the traffic signs seen on the roads and streets are pictorial representations of key information understood by all drivers as an essential element of road safety. The pictograms for this study were designed with the following characteristics in mind, aiming for optimal uptake from patients with minor eye diseases: use of mainly black and white or high-contrast colours; clear and simple images; avoidance of shading, coloured images or coloured backgrounds; and use of plain large font.14 This tool was designed for patients accustomed to interpreting road signs and other commonly available pictograms; in other words, the tool catered to most North Americans with a reading level of grades 6 to 7.
The purpose of the study was to evaluate and validate selected components of a pictogram-based diabetes education tool for use in counselling patients with type 2 diabetes mellitus. Pictogram-associated information recall was assessed to see if the use of pictograms improved recollection of diabetes counselling points. According to the American National Standards Institute (ANSI) standard for validation of individual pictograms, pictorial symbols must reach a criterion of at least 85% correct to achieve validation in a comprehension test.15
Methods
Patients with type 2 diabetes mellitus (as diagnosed by a physician) and between 18 and 85 years old were recruited in offices of consenting primary care physicians in the Greater Moncton area (Moncton, New Brunswick) under the auspices of the Regional Health Authority’s Diabetes Education Centre (DEC). Patients unable to communicate verbally (aphasic, hearing impairment), those with conditions affecting recall ability or with visual impairment preventing viewing pictograms, as well as those deemed too ill or frail to attend visits, were excluded.
Written consent was obtained from patients as well as their primary care physicians, and an individual interview was scheduled with the study assessor (a certified diabetes educator). During the initial interview session, the patient with diabetes was shown 8 pictograms relating to prevention and treatment of “heart disease and stroke” and 7 pictograms relating to the prevention and treatment of “nerve damage,” in association with diabetes. The pictograms used in this study were designed by 2 pharmacists using their expertise of key diabetes counselling points, and incorporated recommendations from focus groups of patients, pharmacists, pharmacy technicians, clerical support staff and graphic designers. The designs catered to most North Americans with a reading level of grades 6 to 7.
Validation
Using a structured interview tool, the assessor asked the patient how each pictogram relates to management of his or her diabetes. The assessor recorded the number of correct responses (one for each pictogram shown to the patient) and the number of incorrect responses. For each incorrect response received, the assessor educated the patient to improve his or her understanding of key aspects of managing diabetes, hoping the patient would use the pictogram as a future visual cue during a follow-up interview.
Recall
A follow-up interview assessing the recall of pictograms was scheduled within 8 weeks of the initial interview for all participants, using a cued recall technique. Cued recall is the use of cues such as pictures or pictograms to recollect information. The participants were once again shown the same pictograms relating to the prevention and treatment of “heart disease and stroke” and “nerve damage,” and the number of correct responses was again recorded. Demographic data such as sex, age, mother tongue, time since diagnosis of diabetes, highest level of education completed, reading habits (self-reported use of electronic or print media) and ethnicity were also collected for each participant.
The data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 20.0 (SPSS, Inc., an IBM Company, Chicago, IL). Categorical variables were summarized using frequencies and percentages.
Results
Seventeen participants were recruited, and all (100%) were white. Twelve (75%) participants were female and 15 (88%) specified English as their mother tongue. The mean ± SD age was 61 ± 11 years. Sixteen participants (94%) had a high level of education (at least high school completed), and 16 (94%) were accustomed to reading some form of media (electronic or print). The mean ± SD value of time since diabetes diagnosis was 5.43 ± 6.31 years (ranging between 1 month and 22 years). The mean time interval between initial interview and follow-up interview was 67 days (ranging between 28 and 100 days).
Participants correctly interpreted (85% or higher) each of the 8 pictograms for the heart disease and stroke module during both initial and follow-up visits (Figure 1). Participants achieved correct interpretation of 28.6% (2 of 7) of pictograms in the nerve damage module during the initial visit and 100% of the pictograms during the follow-up visit (Figure 2).
Figure 1.
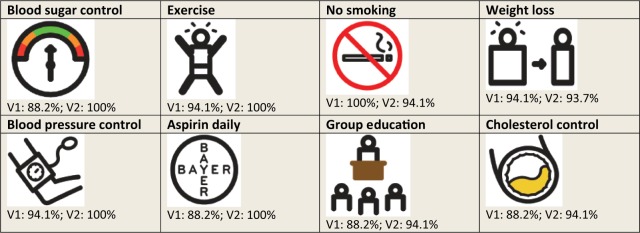
Heart disease and stroke module: percent of correct pictogram interpretation for the 17 participants.
V1 = correct responses at visit 1; V2 = correct responses at visit 2
Figure 2.
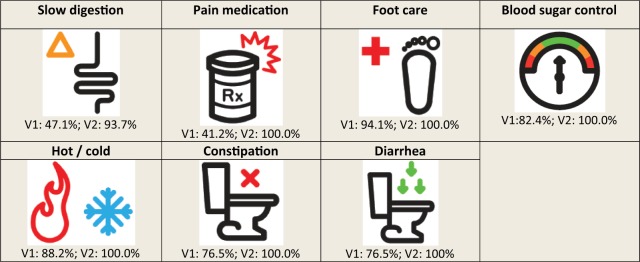
Nerve damage module: percent of correct pictogram interpretation for the 17 participants.
V1 = correct responses at visit 1; V2 = correct responses at visit 2
The percentage of correct overall pictogram interpretations was significantly higher at the second visit (94.9% vs 82.8% at visit 1; 12.2% difference; 95% confidence interval [CI], 4.7-19.7; p < 0.003), predicting a significant increase in information recall. When analyzed individually, only the pictograms “pain medication” and “slow digestion” had a significant improvement in interpretation at the second visit.
Of 13 participants who responded to the question about satisfaction with the counselling tool, 11 (84.6%) were satisfied and 2 (15.4%) were neutral. Three participants did not respond to the question, and 1 was lost to follow-up.
Discussion
Pictograms may have the potential to assist patients’ understanding of the complications of diabetes, but they must be validated prior to their use. This study found that the overall ratings for the heart disease and stroke pictograms appear to support their validity in our study population. However, only 2 of 7 nerve damage pictograms were considered valid at the initial visit. Information regarding neurological effects of diabetes may not be as familiar as that about cardiovascular complications, and the current pictograms may not be representative of these symptoms or self-care strategies. In addition, heart disease and stroke awareness and education tend to get wider exposure in general health media compared with diabetic neuropathy symptoms. The overall pictogram interpretation was significantly higher during recall, which is in agreement with Paivio’s dual coding theory.10 Pictograms enhanced the understanding of verbally communicated diabetes management information and therefore increased participants’ recollection of spoken information. However, this result might not have been the same if free recall method had been used. Free recall is repeating information complete from memory without the use of cues such as pictograms or other pictorial aids. This method would not include the nonverbal system, and so Paivio’s dual coding theory10 would not apply. This was confirmed in numerous pictogram studies, where cued recall produced higher information recollection than free recall in all individuals regardless of the level of schooling.15,16
Proper patient counselling is still a necessity for the optimization of information recollection. In this study, proper counselling of diabetes management occurred for every incorrect response received during the initial visit, therefore providing the verbal aspect of the study. The combination of counselling and pictograms improved patient-to-pictogram association, as well as patients’ understanding of key management points, and further promoted patients’ recall ability, therefore explaining the statistically significant increase in correct responses during the follow-up visit. This result is in contrast to the outcome of other studies where participants were required to independently study the information on their own without guidance.15,17 Independent study of any material could cause information misinterpretations and misunderstandings that would reduce participants’ ability to recall or correctly recall the content. Thus, prior training promotes better recall ability and is essential to testing participants’ recall. Due to the use of both proper information counselling and cued recall in this study, there was an increase in pictogram recollection of diabetes management information.
Our study had several limitations. No association was explored between correct responses and actual adherence in diabetes self-care. Participants’ literacy levels were not assessed at enrollment; they self-reported their highest level of formal schooling and whether they read newspapers or magazines or accessed the Internet. Our study cannot make any inferences about the usefulness of these specific pictograms in low-literacy individuals; however, the recall ability should still be high in low-literacy population, as concluded by previous studies. Although our sample size was small and homogeneous (all English-speaking whites), the findings are consistent with key studies published on pictogram validation.8,9
Implementation of the positive results in this study could offer an innovative option for diabetes educators when working with patients possessing limited health literacy abilities and diabetes management programs that are primarily text based or designed at higher literacy levels. Subsequent studies would need to follow patients for longer periods of time (i.e., months to years), using the pictogram tool as reinforcement for good practices in diabetes self-management and to potentially improve clinical outcomes. Future research in this area would include validation of the remaining 5 modules of this diabetes education program.
Conclusion
Our study provides some preliminary validation of the “heart disease and stroke” and “nerve damage” modules of a diabetes patient education tool. When combined with proper counselling, the heart disease and stroke pictograms produced excellent patient understanding during both initial and follow-up visits. More than half of the pictograms used for nerve damage were not well understood by participants during the initial visit. However, with both counselling and cued recall, participants’ recollection of information during follow-up visits showed statistically significant improvements. ■
Acknowledgments
We thank Elena Pascuet of CHEO for her assistance in the statistical analysis of our study data; Shelley Jones, RN, CDE, of Horizon Health Network for her work in administering the pictograms to study subjects in the Diabetes Clinic; Paula Ryder, RN, BN, MBA, CDE, of Horizon Health Network and Heidi Staples, BScPharm, MSc, CDE, formerly of Horizon Health Network and now with the Canadian Agency for Drug and Technologies in Health, for their work in reviewing the study protocol.
Footnotes
Author Contributions:Dr. Vaillancourt was responsible for the design of pictograms, the study design, data analysis and review of the manuscript. Dr. Doucette was responsible for the study design, data collection, data analysis and review of the manuscript. Li Sha Li was responsible for the data analysis, review and writing of the manuscript. Marion Berthenet was responsible for the data analysis, review and writing of the manuscript.
Declaration of Conflicting Interests:The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding:The authors declared the following financial support for the research, authorship and/or publication of this article: funding received from Medbuy Corporation.
References
- 1. Rootman I, Gordon-El-Bihbety D. A vision for a health literate Canada: report of the Expert Panel on Health Literacy. Ottawa (ON): Canadian Public Health Association; 2008. Available: www.cpha.ca/uploads/portals/h-l/report_e.pdf (accessed August 19, 2014). [Google Scholar]
- 2. Albright J, de Guzman C, Acebo P, et al. Readability of patient education materials: implications for clinical practice. Appl Nurs Res 1996;9:139-43 [DOI] [PubMed] [Google Scholar]
- 3. Wild S, Roglic G, Green A, et al. Global prevalence of diabetes: estimates for the year 2000 and projections for 2030. Diabetes Care 2004;27:1047-53 [DOI] [PubMed] [Google Scholar]
- 4. Schillinger D, Grumbach K, Plette J, et al. Association of health literacy with diabetes outcomes. JAMA 2002;288:475-82 [DOI] [PubMed] [Google Scholar]
- 5. Kavanagh KL. Health literacy in diabetes care: explanation, evidence and equipment. Diabetes Manag (Lond) 2011;1:191-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Revol M, Vaillancourt R, Pouliot A. Evaluation, validation and modification of pictograms depicting potential side effects to medications. J Comm Healthc 2013;6:79-89 [Google Scholar]
- 7. Yin HS, Dreyer BP, Schaick LV, et al. Randomized controlled trial of a pictogram-based intervention to reduce liquid medication dosing errors and improve adherence among caregivers of young children. Arch Pediatr Adolesc Med 2008;162:814-22 [DOI] [PubMed] [Google Scholar]
- 8. Houts PS, Bachrach R, Witmer JT, et al. Using pictographs to enhance recall of spoken medical instructions. Patient Educ Couns 1998;35:83-8 [DOI] [PubMed] [Google Scholar]
- 9. Houts PS, Witmer JT, Egeth HE, et al. Using pictographs to enhance recall of spoken medical instructions II. Patient Educ Couns 2001;43:231-42 [DOI] [PubMed] [Google Scholar]
- 10. Paivio A. Imagery and verbal processes. New York (NY): Holt, Rinehart and Winston; 1971 [Google Scholar]
- 11. Michielutte R, Bahnson J, Dignan MB, Schroeder E. The use of illustrations and narrative text style to improve readability of a health education brochure. J Cancer Educ 1992;7:251-60 [DOI] [PubMed] [Google Scholar]
- 12. Mansoor LE, Dowse R. Effect of pictograms on readability of patient information materials. Ann Pharmacother 2003;37:1003-9 [DOI] [PubMed] [Google Scholar]
- 13. Pictogram. Available: www.pictogram.se (accessed March 13, 2014).
- 14. Good medicine for seniors: guidelines of plain language and good design in prescription medication. Ottawa (ON): Canadian Public Health Association; 2002. Available: www.cpha.ca/uploads/portals/h-l/goodmed_e.pdf (accessed March 15, 2014). [Google Scholar]
- 15. Wilby K, Marra CA, da Silva JH, et al. Randomized controlled trial evaluating pictogram augmentation of HIV medication information. Ann Pharmacother 2011;45:1378-83 [DOI] [PubMed] [Google Scholar]
- 16. Houts PS, Bachrach R, Witmer JT, et al. Using pictograms to enhance recall of spoken medical instructions. Patient Educ Couns 1998;35:83-8 [DOI] [PubMed] [Google Scholar]
- 17. Dowse R, Ehlers M. The evaluation of pharmaceutical pictograms in a low-literate South African population. Patient Educ Couns 2000;45:87-9 [DOI] [PubMed] [Google Scholar]