

Abstract
Background
Use of contraception is influenced by many processes most by the women's empowerment. Women's decision making power and their autonomy within the household is the most important factor affecting contraceptive use. This paper aims to analyze the relationship between these two indicators of women's empowerment and the use of contraception.
Methods
This cross sectional study was conducted by personally interviewing 385 currently married women selected by systematic sampling on a pretested and validated questionnaire. Two indices, women's decision-making power index and women's autonomy index, were constructed and association with contraception use analyzed.
Results & Conclusion
The study gives the evidence that decision making power is low in the respondents with 48.2% (95% CI 43.34, 53.31) of them having low level of power, while 27.6% (95% CI 23.24, 32.16) have medium level and 3.6% (95% CI 2.08, 5.88) having high level of power. 22.4% (95% CI 18.39, 26.70) of women do not have any autonomy as against 43.9% (95% CI 38.99, 48.89) with low level, 25% (95% CI 20.80, 29.44) with medium autonomy and 8.7% (95% CI 6.29, 11.98) scoring above 7 (high level of autonomy). In the study population it was found that 273 (70.7%, 95% CI 66.2, 75.28) of the respondents were using contraceptives. Women's autonomy, years of marriage and number of children were significant variables.
Keywords: Women empowerment, Autonomy, Contraceptive
Introduction
Women's rights and issues have become a subject of serious concern of both academicians and policy makers and have received tremendous attention in the planning, discussions and forums at national and global platforms in both developed and developing countries. A recent policy research report by the World Bank identifies gender equality both as a development objective in itself, and as a means to promote growth, reduce poverty and promote better governance.1 Many international conferences like the Beijing Platform for Action, the Beijing+5 declaration and resolution, the Cairo Program of Action, the Millennium Declaration, and the Convention on the Elimination of All Forms of Discrimination against Women [CEDAW] have emphasized the need for supporting women's empowerment in the policy statements. The social position of women, especially in the developing world, still needs much attention. The National Population Policy 2000, specifically identified the low status of women in India as an important barrier to the achievement of population and maternal and child welfare goals.2 Since the 1994 International Conference on Population and Development, women's empowerment has been recognized as important to their access to reproductive health services, including family planning. Women's decision making power and women's autonomy together represent — women empowerment. Use of contraception is influenced by many processes but the women's decision-making power and their autonomy within the household perhaps is the most important factor affecting contraceptive use.3,4 This paper aims to analyze the relationship between these two indicators of women's empowerment and the use of contraception.
Material and methods
A cross sectional study was conducted by personally interviewing currently married women attending the gynecology and obstetrics outpatient services in a tertiary care hospital with the primary objective to study how contraceptive method use among currently married women varies by the empowerment indices. Women's empowerment was assessed by computing the decision-making power index and autonomy index. A National level survey (National Family Health Survey-3) showed that 54% women who participate in 3–4 household decisions use contraceptive methods compared to 37% of women who participate in no decisions in the household and use contraceptive method.
Assuming 5% desired precision, 95% confidence interval and 0.05 level of significance, the minimum sample size required for the study was 382 women. Responses of 385 currently married women were studied by personal interview technique on a validated questionnaire used by NFHS-3. Women were selected by systematic sampling procedure and data collected over a period of 4 months. Information on the demographic parameters like woman's age, woman's years of education, husband's years of education, number of children, sex of children, age at first child birth, years of marriage and woman's employment status were assessed. This survey included questions related to wife's autonomy and decision-making power in the family along with the information on the women's use of contraceptives. Wife's decision-making power is considered to be wife's ability to express their opinion and influence on family decision-making processes.5,6 The indicators for women's autonomy are in reference to women's capacity of taking initiatives and actions without asking for their partner's approval.7,8 The outcome variable was the contraceptive use by the women and the predictor variables for contraceptive use were the demographic variables with the main emphasis on the two indices of women empowerment namely women's autonomy and women's decision-making power. Contraceptive use was assessed by asking the respondents if they used any contraceptive method along with the method used namely the traditional or modern. The known confounders were adjusted by carrying out logistic regression analysis.
Women's decision making power index and autonomy index
To assess wife's power in decision-making process the survey included six questions – regarding who in the couple make decisions about some of the family issues like: how many children to have; how to rear them; what daily expenses should be incurred; what relatives and friends should be visited; when the couple would have sex and visiting health care facility. Each answer category represents a different level of wife's power and it was assigned a value 0 if it is the husband alone or others who makes such a decision, a value of 1 when the couple together makes the decision and a value of 2 if it is only the wife who makes the decision. Thus the power index was formulated by adding the values for each question. This — Decision-making Power Index ranged from 0 to 12, which was categorized as — No Power who scored 0, — Low who scored between 1 and 4, – Medium who scored between 5 and 8 and — High for those respondents scoring 9–12.5,8 The autonomy index was formulated by asking the respondent whether or not the wife needs her husband's permission for going outside alone, going outside with children, deciding about daily expenses, visiting relatives and friends, working, studying, using contraceptives and participating in community activities. For each of these variables there are two possible values, 0 if the women ask her husband permission and 1 if she does not. It is assumed that those women who do not require husband's permission are autonomous while those who require it are not autonomous.
The autonomy index was constructed by adding the scores for each variable 8. The index ranged from 0 to 9, which was categorized as — No Autonomy who scored 0, — Low who scored between 1 and 3, — Medium who scored between 4 and 6 and — High for those respondents scoring 7–9.5,8 The statistical test used was proportion with 95% confidence interval for various indicators. Logistic regression was used to analyze the relationship between various indices and use of contraception.
Results
The mean age of the respondent was 30.4 years (SD 6.9) with more than 78% (n = 300) with high school and above education. 70% of the husbands were high school passed and 26% were graduates. Only 43% (n = 166) of the wives were working ladies whereas the rest were non-working. Results were formulated with respect to women's decision-making power and women's autonomy indicators and then associated with the contraceptive use. The survey findings indicate that family decision-making process is jointly shared by both the partners. About 68.5% (n = 264) of the respondents expressed that both members jointly take the decision. The distribution of the respondents on the power index is shown in Fig. 1. There is a small proportion of respondents 3.6% who have high decision-making power. In other words women are more concentrated in the first tail of power distribution with 48.2% (n = 186, 95% CI 43.34, 53.31) of them having low level of power (1–3 in the index), while 27.6% (n = 106, 95% CI 23.24, 32.16) have medium level of power (4–6 in the index) and 3.6% (n = 14, 95% CI 2.08, 5.88) having high level of power (7–10 in the index). 20.6% (n = 79, 95% CI 16.71, 24.77) have no decision making power. Going out alone as compared to going out with children is less autonomous as 75.3% of them require husband's permission for going out alone as against only 19.2% who require permission while going out with children. 74% of the respondents cannot use contraceptive methods without asking for their husband's permission. 52% of the respondents have scored 3. The distribution shows that 22.4% (n = 86, 95% CI 18.39, 26.70) of women do not have any autonomy. Also it can be seen 43.9% (n = 169, 95% CI 38.99, 48.89) have scored 1–3 (low level of autonomy), 25% (n = 96, 95% CI 20.80, 29.44) have scored 4–6 (medium autonomy) or less and 8.7% (n = 34, 95% CI 6.29, 11.98) scoring above 7 (high level of autonomy). The frequency distribution of respondents on autonomy index is shown in Fig. 1. The empowerment index was compared by the proportion of respondent's using contraceptives. The respondents were asked regarding the method of contraception and the reasons for using contraception. In the study population it was found that 273 (70.7%, 95% CI 66.2, 75.28) of the respondents were using contraceptives. 113 (29.3%, 95% CI 24.96, 34.05) did not use any form of contraception as against 265 (69%, 95% CI 64.07, 73.31) using modern methods and 7 (1.7%, 95% CI 0.79, 3.56) using traditional method of contraception. Limiting the family represents the reason for using contraception in 87.8% of the women while spacing for 12.2% of the women. Of the respondents who were not using contraceptives 11% were pregnant or amenorrheic, 13% had health concerns, 34% were not aware of the contraceptive methods and 29% wanted more children whereas 13% said it was not required. Logistic regression was used to analyze the relationship between various indices and use of contraception. Table 1 presents the results of the logistic regression. The model explains 67% of the variation in the contraceptive use. Women's autonomy, years of marriage and number of children are significant variables. Surprisingly power index, age, women's education, husband's education and employment of women found no significant effect on use of contraception.
Fig. 1.
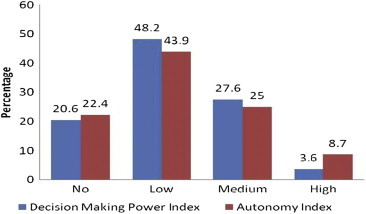
Distribution of respondents on Decision Making Power Index and Autonomy Index.
Table 1.
Logistic regression analysis: dependent variable–contraceptive use.
| Significance | Odds ratio (95% confidence interval) | |
|---|---|---|
| Control Variables Women's Age | ||
| <25 Years | 0.688 | 1.00 |
| 25–35 Years | 0.682 | 1.45 (0.09, 8.62) |
| >35 Years | 0.686 | 0.57 (0.05, 3.23) |
| Women's Education | ||
| None | 0.107 | 1.00 |
| Primary | 0.056 | 41.75 (0.00, 82.64) |
| High school | 0.027 | 31.12 (2.56, 64.21) |
| Graduate/PG | 0.665 | 2.20 (0.02, 91.26) |
| Husband's education | ||
| Primary | 0.749 | 1.00 |
| High school | 0.604 | 2.81 (0.29, 39.42) |
| Graduate/PG | 0.870 | 1.31 (0.01, 54.36) |
| Number of children** | 0.04** | 2.75 (1.69, 3.64) |
| Years of marriage** | 0.04** | 0.84 (0.00, 0.92) |
| Employment | 0.15 | 3.68 (0.82, 12.30) |
| Power index | 0.13 | 0.66 (0.00, 6.59) |
| Autonomy index** | 0.03** | 0.63 (0.01, 0.82) |
**Significant at 5% level of significance.
Discussion
Empowerment of women has widely been acknowledged as a major factor that contributes to better demographic outcomes.9 However most studies examined few aspects of women empowerment and contraceptive use. This study addressed all the aspects of women empowerment and confirmed the association between women's autonomy and women's use of contraception. Gender-based power inequalities can restrict open communication between partners about reproductive health decisions as well as women's access to reproductive health services, which contributes to poor health outcomes. The importance of spousal communication is often emphasized in family planning programs and research. It is the first step in a rational fertility decision-making process.10 In developing countries most communities afford inferior positions to women.9 In effect women are either under collective decision-making with their partners or completely rely on the male partner's decision on issues that affect their reproductive life. This paper also confirms that decision-making power is low in the respondents with 48.2% of them having low level of power. On autonomy index also the respondents have done poorly with 43.9% having scored low on autonomy index. This study is limited by the data available to measure women's empowerment. Information was gathered from women's responses to questions about usual practices in their household, which could have added the risk of social desirability bias. Another limitation of this study is related to the cross-sectional nature of data. Because the study is cross sectional in nature the temporal relationship between the two variables cannot be determined. Despite these limitations, our study found important associations between women's autonomy and use of contraception, which have significant implications.
Conclusions
This research has highlighted key issue of contraceptive use and women's empowerment in terms of autonomy index and power index. The survey findings indicate as expected that family decision-making process is jointly shared by both the partners and it can be concluded that women's autonomy plays a significant role in the utilization of the family planning services.
Conflicts of interest
All authors have none to declare.
Acknowledgment
The authors are immensely grateful to all the women who have contributed to the study. We also wish to thank our medico social worker Mrs Kumkar for all the help extended by her.
References
- 1.World Bank . Oxford University Press; New York: 2001. Engendering Development—Through Gender Equality in Rights, Resources, and Voice. A Policy Research Report. [Google Scholar]
- 2.Ministry of Health and Family Welfare (MOHFW) MOHFW; New Delhi: 2005. Annual Report 2004–2005. [Google Scholar]
- 3.Roy T.K., Niranjan S. Indicators of women's empowerment in India. Asia-Pacific Popul J. September 2004;19(3):23–38. [Google Scholar]
- 4.Nancy Riley. Gender, power and population Change & Verbar. Popul Bull. May 1997;52 [PubMed] [Google Scholar]
- 5.National Family Health Survey Subject Reports, Number 3. March 1997. [Google Scholar]
- 6.International Institute for Population Sciences (IIPS) and Macro International . Vol. I. 2007. (National Family Health Survey (NFHS-3), 2005–06: India). [Google Scholar]
- 7.Kantor P. Women's empowerment through home-based work: evidence from India. Dev Change. 2003;34(3):425–445. [Google Scholar]
- 8.Irene Casique. Paper Presented at the XXIV IUSSP General Population Conference, Salvador, Bahia. August 2001. What difference does it make? Women‘s autonomy and power and use of contraception in Mexico. [Google Scholar]
- 9.Dyson T., Moore M. Kinship structure, female autonomy, and demographic behavior in India. Popul Dev Rev. 1983;9(1):35–60. [Google Scholar]
- 10.Mott F.L., Mott S. Household fertility decisions in West Africa: a comparison of male and female survey results. Stud Fam Plan. 1985;16(2):88–99. [PubMed] [Google Scholar]