

Abstract
Aim:
The aim was to measure the prevalence of smoking and identify its potential predictors among military personnel in Kingdom of Saudi Arabia (KSA).
Materials and Methods:
This cross-sectional study was carried out among military personnel in the five military regions of KSA between January 2009 and January 2011. The sample of 10,500 military personnel in the Saudi Armed Forces was equally divided among the five regions with a ratio 3:7 for officers and soldiers. A multistage stratified random sampling was used to recruit participants in the four services of the armed forces in the five regions. Information on sociodemographic characteristics with a detailed history of smoking was collected by means of a self-administered questionnaire. Bivariate analysis was used to identify the factors associated with smoking, and multiple logistic regression analysis to discover its potential predictors.
Results:
About 35% of the sample was current smokers, with higher rates among soldiers. The eastern region had the highest rate (43.0%), and the southern region the lowest (27.5%). Navy personnel had a higher risk of being current smokers (40.6%), and the air defense the lowest risk (31.0%). Multivariate analysis identified working in the navy, and low income as positive predictors of current smoking, while residing in the southern region, older age, years of education, being married, and having an officer rank were negative (protective) factors.
Conclusion:
Smoking is prevalent among military personnel in KSA, with higher rates in the Navy and Air Force, among privates, younger age group, lower education and income, and divorced/widowed status. Measures should be taken to initiate programs on smoking cessation that involve changes in the environment that is likely to promote this habit.
Keywords: Military, officers, Saudi, smoking, soldiers
INTRODUCTION
Cigarette smoking is an established risk factor for many diseases although it is amenable to prevention. The rates of smoking have shown decreasing trends in adults in many countries since 1965,[1] yet the rates at which youngsters, particularly military recruits start smoking are on the rise.[2] This has been attributed to the use of smoking as a means of coping with stress experienced in military settings, to the extent that smoking has been alluded to as “part of the military culture.”[3] In military settings smoking is used to combat anxiety, monotony, lack of sleep, and peer influence, which is another important reason for smoking.[4] The military has, therefore, with the large numbers, dispersion throughout the world, and high receptiveness been the target of the tobacco industry for decades.[5]
The prevalence rates of smoking among military personnel show wide variations among countries. Very high rates have been reported in the Lithuanian army, reaching 70%.[6] In the Greek Navy, 59.5% are current smokers.[7] The rates found in the French army were 54.1%,[8] Italian 54.4%,[9] and Polish 40-65%.[10] A lower prevalence rate of 39% was reported among USA soldiers.[11] Moreover, Grier et al.[12] have reported a decrease in the number of cigarettes smoked per day in USA premilitary service from 2000 to 2006. The UK had one of the lowest rates, with 31.3% of soldiers being current smokers.[13]
The effect of smoking on military personnel is deleterious. Apart from the associated organic physical disorders with more hospitalizations,[14] smoking has a negative impact on fitness and productivity.[15] Smokers have been shown to have lower mental capacities and fitness for duty,[16] less readiness, substance abuse, and legal problems.[17,18] Given these harmful effects and the consequent considerable costs, the US Department of Defense set a priority to reduce smoking in its military forces.[19]
The Kingdom of Saudi Arabia (KSA) is a country where smoking is considered socially undesirable for religious and cultural reasons. Nonetheless, the prevalence rate of smoking in a population-based sample of adult men (30 years or older) in the Eastern province of KSA has reached 28.7%.[20] Given this relatively high prevalence rate in the general population, and the absence of data concerning smoking in the Saudi army, the aim of this study was to measure the prevalence of smoking among military personnel in KSA, and to identify the potential predictors.
MATERIALS AND METHODS
This work was part of a national study surveying chronic diseases and their risk factors among military personnel in the five military regions of KSA: Eastern, western, northern, southern, and central. A detailed methodology of the main survey has previously been reported.[21] The study used a descriptive cross-sectional design. The sample consisted of 10,500 military personnel of any rank serving in the Saudi Armed Forces during the time of the study. This sample size was large enough to measure the prevalence of any disease or risk factor of 10% or more, with a 2% absolute precision, at 95% level of confidence, with a design effect of 2.5, and compensating for a dropout rate of approximately 20%. The sample was equally divided among the five regions with a ratio 3:7 for officers and soldiers. A multistage stratified random sampling was used to recruit participants. Each of the five regions included four services of the armed forces: Air, land, navy, and air defense. From each of these within each region, a systematic random sample was recruited. The sample size which was equal in the five regions with 2100 subjects each was distributed according to the different forces as follows: 3:3:3:1.5 for air, land, navy, and air defense in each region. It was also allocated according to rank at 3:7 for officers and enlisted personnel (soldiers). However, in the actual fieldwork, the percentages of officers to soldiers (enlisted men) varied among services, so that the overall ratio of officers to soldiers was <3:7.
The main study utilized the World Health Organization STEPwise approach to chronic disease risk factor surveillance.[22] The current study used the data of the first step of this approach, which involved information about the sociodemographic characteristics of the participants with a detailed smoking history covering smoking status, duration and amount, age at start, and age at quitting if applicable. The determination of the smoking status was based on the Centers for Disease Control and Prevention guidelines (CDC, 2009).[23] Accordingly, a person is considered a smoker if he has smoked at least 100 cigarettes in his entire life; if he was smoking during the time of the survey he was classified as “current smoker”, and if not he was classified as an “ex-smoker.” A “never smoker” is someone who reported never having smoked 100 cigarettes. The questionnaire was self-administered in Arabic. All questions were of the closed type except for those that dealt with numbers such as the age, number of cigarettes, years of smoking, and so forth. The tool was pilot-tested in Riyadh (central region) for clarity and feasibility and was finalized accordingly. The front page of the tool consisted of an informed consent form that was signed by the eligible person willing to participate. All principles of the Helsinki Declaration were followed, and the pertinent authorities approved the study protocol. The project lasted from January 2009 to January 2011.
The data management for the whole project was carried out using the Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, USA) version 14.0. Chi-square test was used in bivariate analysis to identify the factors associated with the smoking status. Then, multiple logistic regression analysis was carried out to identify the potential predictors of smoking with adjusted odds ratios (OR). Statistical significance was set at P < 0.05.
RESULTS
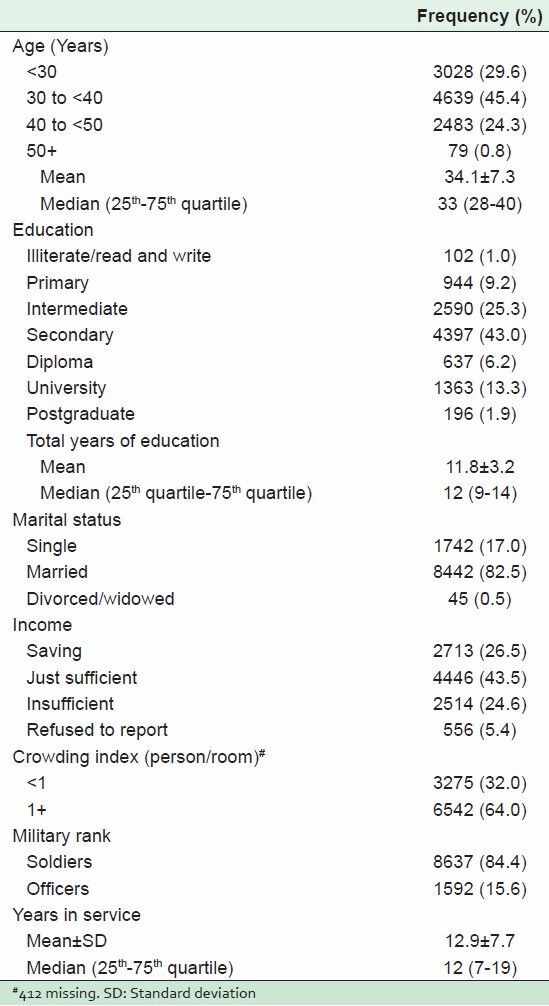
The survey sample included 10,229 participants with valid completed forms, a response rate of 97.4%. As Table 1 indicates, slightly less than half of the sample were in the age group of 30 to <40 years (median 33), and had secondary/diploma level of education, with a median of 12 years; most were married (82.5%). Approximately one-fourth of the sample considered their income sufficient to save, while another quarter reported insufficient income. Concerning work, most of the sample (84.4%) consisted of enlisted men and the median duration of military service was 12 years.
Table 1.
Sociodemographic and job characteristics of the survey sample (n=10,229)
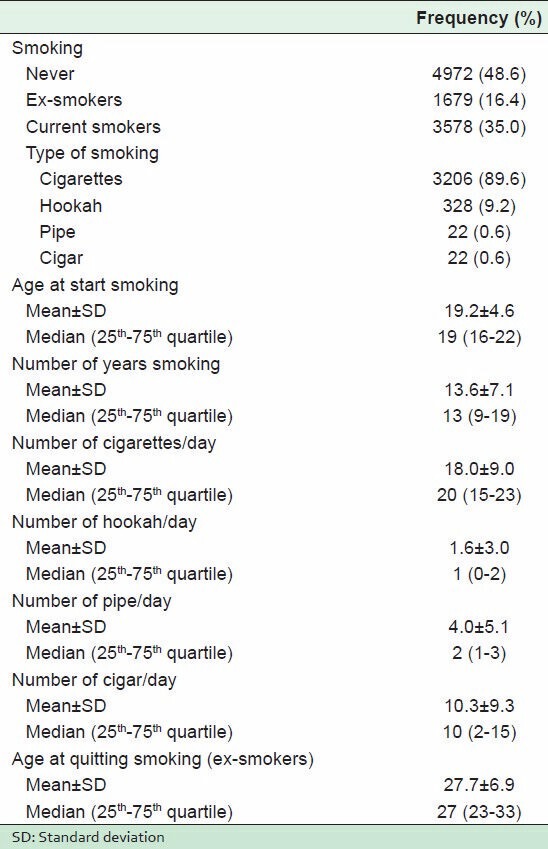
Regarding smoking, Table 2 shows that slightly less than half of the sample (48.6%) reported having never smoked while almost one-third (35%) were current smokers. The most common smoking type of smoke after cigarettes was hookah. The median age at initiation was 19 years and at quitting 27 years. The average duration of smoking was 13 years, with a median consumption of one packet (20 cigarettes)/day.
Table 2.
Smoking habits in the survey sample (n=10,229)
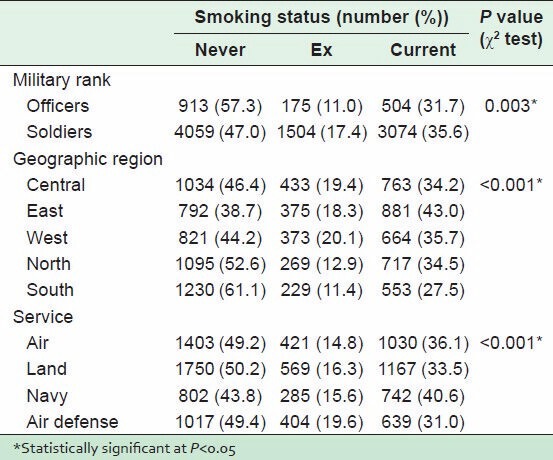
Bivariate analysis revealed some statistically significant differences among the military ranks (P = 0.003) as well as the geographic regions and the forces (P < 0.001). Table 3 demonstrates higher rates of current smoking among soldiers compared with officers. Furthermore, the eastern region had the highest rate of current smokers, whereas the southern region had the lowest. With regard to the various services, the highest rates of current smokers were in the navy and the lowest in the air defense.
Table 3.
Comparison of smoking habits by military ranks, regions, and forces
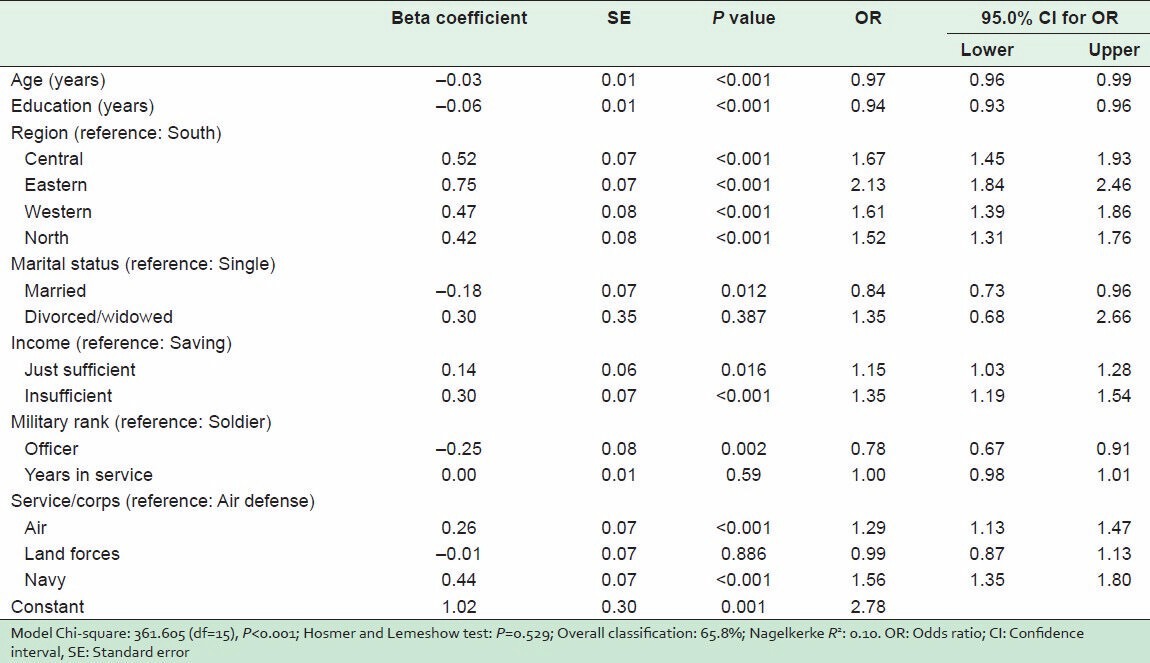
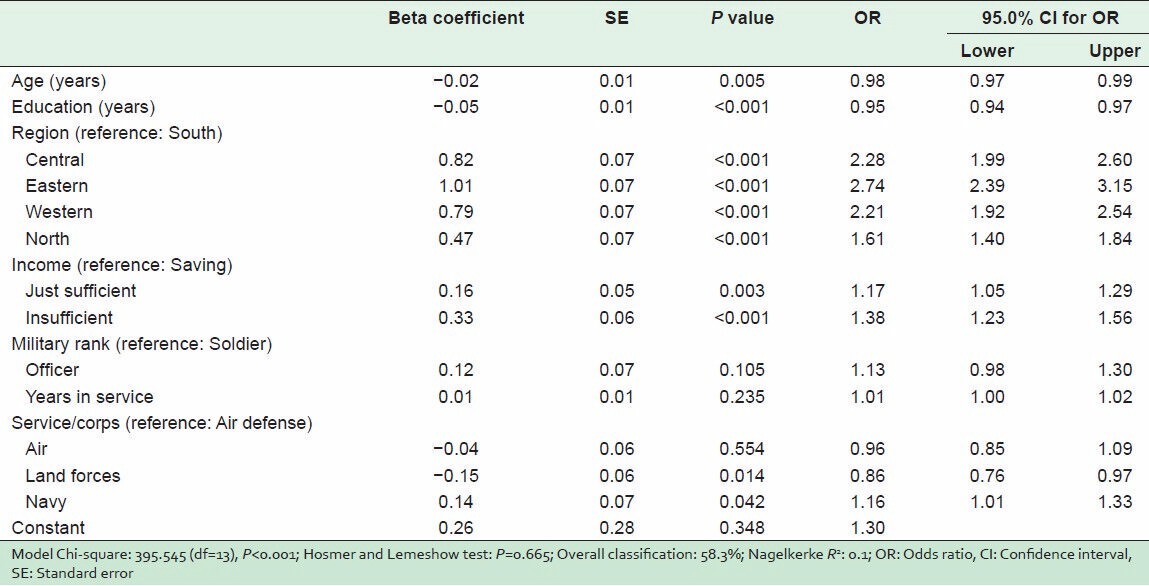
Multivariate analysis identified older age, more years of education, being married, and being an officer as independent statistically significant negative predictors of current smoking that is, protective factors [Table 4]. The most protective of these factors were being of officer rank (adjusted OR = 0.78, 95% confidence interval [CI]: 0.67-0.91) and being married (adjusted OR = 0.84, 95% CI: 0.73-0.96). However, living in any region other than the southern region was statistically significant positive predictor of current smoking, with the highest risk being domiciled in the eastern region (adjusted OR = 2.13, 95% CI: 1.84-2.46). The table also shows that working in the navy, or the air force was a positive predictor of current smoking, compared with air defense. Lastly, the insufficiency of income positively predicted current smoking, and the risk increased as income became less adequate. Meanwhile, the years of military service had no significant association with current smoking.
Table 4.
Predictors of current smoking in the survey sample (n=10,229)
The multivariate analysis was repeated for the prediction of the state of “ever smoking” [Table 5]. It revealed similar findings on the analysis of current smoking regarding age, years of education, geographic region, and income. Meanwhile, the effects of the military rank and of the marital status lost their statistical significance. As regards the nature of the service, work in the navy was still a positive predictor of “ever smoking,” but working in the land forces became protective (adjusted OR = 0.86, 95% CI: 0.76-0.97).
Table 5.
Predictors of “ever smoking” in the survey sample (n=10,229)
DISCUSSION
This nationwide survey showed a high rate of smoking among military personnel in the KSA. The most important personal predictors of being a current smoker were the individual's age, level of education, marital status, income, and the region of residence. Regarding work-related factors, the predictors were the individual's military rank, and the type of service, but not the years of military service.
The survey results indicated that slightly more than one-third (35%) of the participants were current smokers. The rate was close to the figure reported among US army personnel (38%),[24] but lower than what was reported among the military in Syria (43.2-55.1%),[25] in Italy (54.4%),[9] and much lower than what was reported from Turkey (63.7%).[26]
The relatively low rate found in our study could be attributed to the influence of the conservative culture and the social intolerance of smoking on the religious basis. However, the very high prevalence - almost double - in Turkey makes this explanation debatable since both countries are Islamic. On the other hand, the difference between the rates in the Saudi military and those of Turkey may be explained on societal rather than on religious grounds. For instance, a study of religious officials in Turkey showed that approximately 15% of them were current or ex-smokers, and only 43.6% thought it was forbidden by Islam.[27] Hence, although research has demonstrated a close negative relationship between religious belief and smoking,[28] the societal norms seem to have a stronger impact on starting or quitting the habit.[29] The current study's finding of the independent effect of the region on smoking is a further confirmation of this explanation. The lowest prevalence of smoking in the southern region and the highest in the eastern region with an adjusted OR of more than double reflects the differences in the level of conservatism between the two regions.
Another potential predictor of smoking identified in this study is the type of armed force or service. The results of the study revealed that serving in the navy was associated with an almost 1½ times higher risk of being a current smoker. The effect is less obvious for the risk of being current or ex-smoker ("ever smoker"), which implies that quitting smoking is less likely among those who serve in the navy. The finding could be attributed to the nature of the work in the navy with long hours of leisure and associated boredom. This means that work in the navy is said to “encourage” smoking.[30] In this situation, smoking is a means of coping, although it is negative. Our results are in accord with previous studies that demonstrated higher rates of smoking in the navy in Australia particularly those deployed overseas,[31] as well as in Greece,[7] and in the USA.[32]
According to this study results, serving in the air force was second to the navy in the probability of being a current smoker. The stress of the job, pace of work, and tension could be the factors underlying the higher rates of smoking, which is an attempt to relax and relieve anxiety. The finding agrees with a US study on the high prevalence of smoking among personnel in the Air Force, and its relation to the stress of being deployed to high-threat combat environment.[33] Smoking is also said to help to stay alert.[34]
In addition to the type of service in the armed forces, rank seems to have an influence on smoking. Our results indicate that being an officer reduced the probability of being a “current smoker” by approximately one-fifth, meaning that the other ranks were more vulnerable to smoking than officers. A French study reported similar findings of higher rates of smoking among privates.[8] Similarly, in a US army study, there were more “current smokers” in the enlisted ranks than in the officer corps.[24]
However, the military rank's effect on current smoking status in this study was insignificant when current and ex-smokers were combined into “ever smoked,” indicating that the probability of the cessation of smoking was higher among officers than privates. This might be attributed to higher awareness and better health behavior, in addition to a tendency to being “role model” for subordinates. In line with this, a study of the US military personnel demonstrated more attempts to quit among officers compared with enlisted personnel. In addition, they had higher rates of the use of smokeless tobacco.[35]
The duration of military service had no influence on the smoking status of the participants of this study. This might be explained by the fact that the duration of service correlates with other independent predictors such as age, rank, and income. This finding is similar to that reported in a study in Turkey where the years of service was not a significant predictor of smoking.[26] However, a study in Italy revealed a positive association between the duration of military service and the prevalence of smoking.[9] This issue needs further investigation.
This study identified certain sociodemographic characteristics as independent predictors of smoking among participants. The probability of smoking decreased with advancing age, higher level of education, being married, and having a higher income. These findings agree with previous studies in military settings, such as those done in France,[8] Australia,[31] and Taiwan[36] that showed a higher prevalence of smoking in respondents who were younger and less educated. In addition, a study in USA[32] showed a higher prevalence of smoking among singles. In KSA, a study among civilians demonstrated the association between smoking and all these factors.[20] The relation with income has been explained by the negative economic impact of smoking on smokers, of greater financial strain and more problems.[37] Concerning the influence of marital status, a recent study carried out among youngsters in the United Arab Emirates revealed that most of the participants of both genders expressed their unwillingness to have a future spouse who smoked, reflecting a general objection to smoking.[38]
The study findings lead to the conclusion that smoking in the Saudi army is closer to the lower rates reported among the military internationally. However, the rate would be high if current and ex-smokers are combined to account for the possible bias of under-reporting, which is a limitation of this study. Smoking is higher in the Navy and Air Force and among privates, and increased with younger age, lower education and income, and status of being divorced/widowed. Measures should be taken to initiate programs for smoking cessations. Changes should be made to conditions that promote this smoking habit or culture such as smoking breaks and accessibility to tobacco and the provision of smoking areas at work premises. Special attention should be given to more vulnerable groups such as noncommissioned officers, younger age, those with lower education, and income. Future research is needed to assess the effectiveness of interventions aimed at changing the environment that promotes this habit.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Giovino GA. Epidemiology of tobacco use in the United States. Oncogene. 2002;21:7326–40. doi: 10.1038/sj.onc.1205808. [DOI] [PubMed] [Google Scholar]
- 2.Haddock CK, Lando HA, Pyle SA, Debon M, Weg MV, Klesges RC, et al. Prediction of adult-onset smoking initiation among U.S. Air force recruits using the pierce susceptibility questionnaire. Am J Prev Med. 2005;28:424–9. doi: 10.1016/j.amepre.2005.02.010. [DOI] [PubMed] [Google Scholar]
- 3.Nelson JP, Pederson LL. Military tobacco use: A synthesis of the literature on prevalence, factors related to use, and cessation interventions. Nicotine Tob Res. 2008;10:775–90. doi: 10.1080/14622200802027123. [DOI] [PubMed] [Google Scholar]
- 4.Hussain NA, Akande M, Adebayo ET. Prevalence of cigarette smoking and knowledge implications among Nigerian soldiers of its health. East Afr J Public Health. 2010;7:81–3. doi: 10.4314/eajph.v7i1.64701. [DOI] [PubMed] [Google Scholar]
- 5.Joseph AM, Muggli M, Pearson KC, Lando H. The cigarette manufacturers' efforts to promote tobacco to the U.S. military. Mil Med. 2005;170:874–80. doi: 10.7205/milmed.170.10.874. [DOI] [PubMed] [Google Scholar]
- 6.Kelbauskas E, Kelbauskiené S, Paipaliené P. Smoking and other factors influencing the oral health of Lithuanian Army recruits. Mil Med. 2005;170:791–6. doi: 10.7205/milmed.170.9.791. [DOI] [PubMed] [Google Scholar]
- 7.Mazokopakis EE, Vlachonikolis IG, Lionis CD. Smoking behavior of Greek warship personnel. Mil Med. 2003;168:929–33. [PubMed] [Google Scholar]
- 8.Marimoutou C, Queyriaux B, Michel R, Verret C, Haus-Cheymol R, Mayet A, et al. Survey of alcohol, tobacco, and cannabis use in the French army. J Addict Dis. 2010;29:98–106. doi: 10.1080/10550880903436028. [DOI] [PubMed] [Google Scholar]
- 9.Di Nicola M, Occhiolini L, Di Mascio R, Vellante P, Colagrande V, Ballone E. Smoking habits in a sample of young Italian soldiers. Mil Med. 2006;171:69–73. doi: 10.7205/milmed.171.1.69. [DOI] [PubMed] [Google Scholar]
- 10.Jedrzejko M. Tobacco use by career soldiers of the Polish Armed Forces - the start of a breakthrough? Przegl Lek. 2004;61:1184–8. [PubMed] [Google Scholar]
- 11.Ornelas S, Benne PD, Rosenkranz RR. Tobacco use at Fort Riley: A study of the prevalence of tobacco use among active duty soldiers assigned to Fort Riley, Kansas. Mil Med. 2012;177:780–5. doi: 10.7205/milmed-d-11-00131. [DOI] [PubMed] [Google Scholar]
- 12.Grier T, Knapik JJ, Canada S, Canham-Chervak M, Jones BH. Tobacco use prevalence and factors associated with tobacco use in new U.S. Army personnel. J Addict Dis. 2010;29:284–93. doi: 10.1080/10550887.2010.489445. [DOI] [PubMed] [Google Scholar]
- 13.Owers RC, Ballard KD. "What else is there to do." - A qualitative study of the barriers to soldiers stopping smoking? J R Army Med Corps. 2008;154:152–5. doi: 10.1136/jramc-154-03-03. [DOI] [PubMed] [Google Scholar]
- 14.Woodruff SI, Conway TL, Shillington AM, Clapp JD, Lemus H, Reed MB. Cigarette smoking and subsequent hospitalization in a cohort of young U.S. Navy female recruits. Nicotine Tob Res. 2010;12:365–73. doi: 10.1093/ntr/ntq007. [DOI] [PubMed] [Google Scholar]
- 15.Hoffman KM, Haddock CK, Poston WS, Taylor JE, Lando HA, Shelton S. A formative examination of messages that discourage tobacco use among junior enlisted members of the United States military. Nicotine Tob Res. 2008;10:653–61. doi: 10.1080/14622200801978730. [DOI] [PubMed] [Google Scholar]
- 16.Shamrei VK, Marchenko AA, Fomin SA. Prevention of tobacco addiction in the Armed Forces. Voen Med Zh. 2011;332:4–8. [PubMed] [Google Scholar]
- 17.Zajc I, Brajdic D, Biocic J, Bošan-Kilibarda I, Kopic V, Siber S, et al. The effect of tobacco use on oral health and dental readiness in the Croatian Army. J Addict Dis. 2011;30:159–68. doi: 10.1080/10550887.2011.554783. [DOI] [PubMed] [Google Scholar]
- 18.Haddock CK, Pyle SA, Poston WS, Bray RM, Stein RJ. Smoking and body weight as markers of fitness for duty among U.S. military personnel. Mil Med. 2007;172:527–32. doi: 10.7205/milmed.172.5.527. [DOI] [PubMed] [Google Scholar]
- 19.Richey PA, Klesges RC, Talcott GW, Debon M, Womack C, Thomas F, et al. Efficacy of a smoking quit line in the military: Baseline design and analysis. Contemp Clin Trials. 2012;33:959–68. doi: 10.1016/j.cct.2012.04.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Al-Turki KA, Al-Baghli NA, Al-Ghamdi AJ, El-Zubaier AG, Al-Ghamdi R, Alameer MM. Prevalence of current smoking in Eastern province, Saudi Arabia. East Mediterr Health J. 2010;16:671–6. [PubMed] [Google Scholar]
- 21.Al-Dahi S, Al-Khashan H, Al Madeer MA, Al-Saif K, Al-Amri MD, Al-Ghamdi O, et al. Assessment of Framingham cardiovascular disease risk among militaries in the Kingdom of Saudi Arabia. Mil Med. 2013;178:299–305. doi: 10.7205/MILMED-D-12-00079. [DOI] [PubMed] [Google Scholar]
- 22.WHO. WHO STEPwise approach to chronic disease risk factor surveillance-Instrument v2.0. Department of Chronic Diseases and Health Promotion. 2008. [Last accessed on 2008 Feb 11]. Available from: http://www.who.int/chp/steps .
- 23.Centers for Disease Control and Prevention (CDC). State-specific secondhand smoke exposure and current cigarette smoking among adults-United States, 2008. MMWR Morb Mortal Wkly Rep. 2009;58:1232–5. [PubMed] [Google Scholar]
- 24.Cunradi CB, Moore RS, Ames G. Contribution of occupational factors to current smoking among active-duty U.S. Navy careerists. Nicotine Tob Res. 2008;10:429–37. doi: 10.1080/14622200801889002. [DOI] [PubMed] [Google Scholar]
- 25.Maziak W, Mzayek F, Devereaux AV. The dynamics of cigarette smoking during military service in Syria. Int J Tuberc Lung Dis. 2001;5:292–6. [PubMed] [Google Scholar]
- 26.Tekbas F, Vaizoglu SA, Guleç M, Hasde M, Güler C. Smoking prevalence in military men, and factors affecting this. Mil Med. 2002;167:742–6. [PubMed] [Google Scholar]
- 27.Sucakli MH, Ozer A, Celik M, Kahraman H, Ekerbicer HC. Religious officials' knowledge, attitude, and behavior towards smoking and the new tobacco law in Kahramanmaras, Turkey. BMC Public Health. 2011;11:602. doi: 10.1186/1471-2458-11-602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Garrusi B, Nakhaee N. Religion and smoking: A review of recent literature. Int J Psychiatry Med. 2012;43:279–92. doi: 10.2190/PM.43.3.g. [DOI] [PubMed] [Google Scholar]
- 29.Yong HH, Savvas S, Borland R, Thrasher J, Sirirassamee B, Omar M. Secular versus religious norms against smoking: Which is more important as a driver of quitting behaviour among Muslim Malaysian and Buddhist Thai smokers? Int J Behav Med. 2013;20:252–8. doi: 10.1007/s12529-012-9225-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Cronan TA, Conway TL, Kaszas SL. Starting to smoke in the Navy: When, where and why. Soc Sci Med. 1991;33:1349–53. doi: 10.1016/0277-9536(91)90278-k. [DOI] [PubMed] [Google Scholar]
- 31.Barton CA, McGuire A, Waller M, Treloar SA, McClintock C, McFarlane AC, et al. Smoking prevalence, its determinants and short-term health implications in the Australian Defence Force. Mil Med. 2010;175:267–72. doi: 10.7205/milmed-d-09-00287. [DOI] [PubMed] [Google Scholar]
- 32.Lynch JP, Hanson K, Kao TC. Health-related behaviors in young military smokers. Mil Med. 2004;169:230–5. doi: 10.7205/milmed.169.3.230. [DOI] [PubMed] [Google Scholar]
- 33.Talcott GW, Cigrang J, Sherrill-Mittleman D, Snyder DK, Baker M, Tatum J, et al. Tobacco use during military deployment. Nicotine Tob Res. 2013;15:1348–54. doi: 10.1093/ntr/nts267. [DOI] [PubMed] [Google Scholar]
- 34.Widome R, Joseph AM, Polusny MA, Chlebeck B, Brock B, Gulden A, et al. Talking to Iraq and Afghanistan war veterans about tobacco use. Nicotine Tob Res. 2011;13:623–6. doi: 10.1093/ntr/ntr028. [DOI] [PubMed] [Google Scholar]
- 35.Peterson AL, Severson HH, Andrews JA, Gott SP, Cigrang JA, Gordon JS, et al. Smokeless tobacco use in military personnel. Mil Med. 2007;172:1300–5. doi: 10.7205/milmed.172.12.1300. [DOI] [PubMed] [Google Scholar]
- 36.Lin YS, Wu DM, Lai HR, Shi ZP, Chu NF. Influence of knowledge and attitudes on smoking habits among young military conscripts in Taiwan. J Chin Med Assoc. 2010;73:411–8. doi: 10.1016/S1726-4901(10)70089-7. [DOI] [PubMed] [Google Scholar]
- 37.Pyle SA, Haddock CK, Poston WS, Bray RM, Williams J. Tobacco use and perceived financial strain among junior enlisted in the U.S. Military in 2002. Prev Med. 2007;45:460–3. doi: 10.1016/j.ypmed.2007.05.012. [DOI] [PubMed] [Google Scholar]
- 38.Bello SU, Jibril MA, Hassam HA, Haisan F, Al Zaabi J, Zangon Daura HS, et al. Smokers and marriage: Attitude of youth in the United Arab Emirates. Asian Pac J Cancer Prev. 2012;13:953–6. doi: 10.7314/apjcp.2012.13.3.953. [DOI] [PubMed] [Google Scholar]