

Abstract
Brucellosis is a zoonotic disease with widespread prevalence. It presents with in various range and often with the presence of non-specific clinical signs and symptoms. Brucellosis also may cause different manifestations in eyes such as uveitis, keratitis, conjunctivitis and neuro-ophthalmic defects. Ocular brucellosis is rare among children. Herein, we present a 7-year-old girl with systemic and ocular brucellosis. After treatment with systemic steroid and antibiotics, her signs and symptoms disappeared. Since early treatment is important in preventing permanent visual loss and the other complications of ocular brucellosis, examination of the eyes in brucellosis patients must always be noticed by clinicians working in this field.
Keywords: Chorioertinitis, ocular brucellosis, ocular manifestations, uveitis
INTRODUCTION
Brucellosis is a highly contagious zoonotic disease caused by ingestion of unsterilized milk or raw meat from infected animals or in close contact with their secretions; however, this disease is more prevalent in some parts in the world especially Middle East, the Mediterranean, Mexico, and Central and South America.[1] Isfahan has been one of the most important endemic areas of Brucellosis in central Iran for many years.[2]
Most cases in the world are caused by B. melitensis, which is the most virulent subtype of Brucella species.[1] Brucellosis has different clinical manifestations that mostly include: Fever, sweating, low back pain, malaise, and arthralgia. These symptoms may be varied from mild to severe.[3]
Two different clinical courses were recognized for this disease: Acute brucellosis (duration <8 weeks) and chronic brucellosis (duration ≥8 weeks).[1] The diagnosis of brucellosis should be considered in the setting of otherwise unexplained chronic fever and nonspecific complaints.
Moreover, brucellosis can cause different manifestations in eyes such as uveitis (anterior uveitis, posterior uveitis, intermediate uveitis, panuveitis), conjunctivitis and neuro-ophthalmic defects (papilledema, papillitis, third cranial nerve paresis).[1]
The history should include details regarding possible sources of exposure to Brucella, including contact with animal tissues or ingestion of unpasteurized milk or cheese and raw meat. Laboratory tests for diagnosis of brucellosis include specimen culture, serologic test, and polymerase chain reaction (PCR). Ideally, the diagnosis is made by culturing the specimen for detection of the organism.[4] Most of the serological studies for the diagnosis of brucellosis are based on antibody detection.[5] Serum agglutination test is the best modality for serology testing. It is generally agreed that a titer of >1:160 in the presence of a compatible illness supports the diagnosis of brucellosis.[6]
Treatment recommendations for children consist of combination therapy with a tetracycline (for children ≥8 years) or trimethoprim-sulfamethoxazole (TMP-SMX, for children <8 years) and at least one other drug including rifampin, gentamicin, or streptomycin, depending upon the site of infection.[7,8,9]
CASE REPORT
A 7-year-old girl was admitted to Feiz hospital (Isfahan, Iran) with the chief complaint of decreased vision, pain and photophobia in right eye since last week. Vision in left eye was 20/20, versus 20/400 in the right eye. No afferent pupillary defect was detected but pupillary reaction to the light in right eye optic disc (OD) was sluggish.
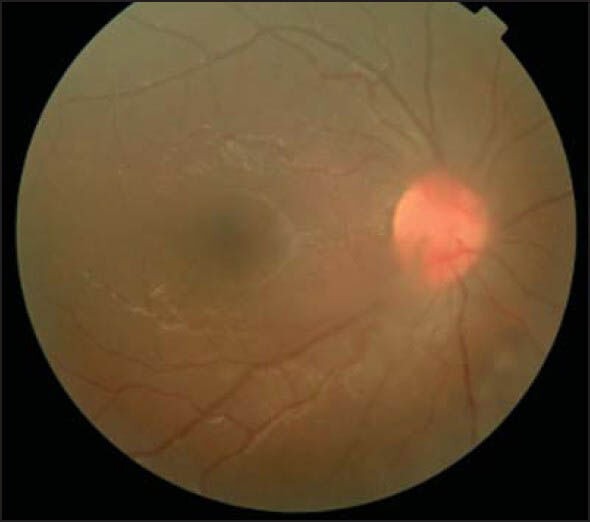
In slit lamp examination, left eye was normal but right eye had ciliary injection, episcleritis, fine keratic precipitate (KP) on corneal endothelium, 2 plus flare, 4 plus cell reaction and 0.5 mm hypopyon in anterior chamber. Iris was normal without nodules. However, vitreous had 4 plus vitritis and 2 plus haziness. Optic disc and posterior pole were normal but at the periphery of retina some patches of choriretinitis were observed [Figure 1].
Figure 1.

Vitreous haziness in the first day
In the medical history, she had wrist pain, fever and anorexia started since two months ago. We examined her some laboratory tests for ruling out certain diseases like juvenile rheumatoid arthritis (JRA) and systemic lupus erythematous sarcoidosis, tuberculosis and syphilis. Based on these evidences and the history of contact with sheep, some specific laboratory tests for brucellosis were evaluated. 2-mercaptoethanol (2ME) brucella agglutination test (1/160), Wright agglutination test (1/160) and Combs Wright (1/320) showed high titer of antibodies; and the result of reponemal test, Tuberculosis Skin Test and chest x-ray, the Angiotensin-converting enzyme, Rheumatoid Factor (RF) and Antinuclear Antibody Test (ANA) were negative. Accordingly, systemic brucellosis was diagnosed for her.
We referred her to pediatrician and consulted him about the patient. After consultation, systemic treatment with rifampin and sulfadiazine/trimethoprim in concomitant with eye drops of betamethasone every 3 hours and tropicamide every 6 hours were administered for her. There after 5 days of systemic treatment, we started with systemic prednisolone 1 mg/kg (oral) and followed her weekly.
After 2 weeks of the treatment, she started to show improvement, and 2 months later of systemic treatment and local steroid therapy, the signs and symptoms disappeared and her vision was back to normal (final visual acuity was 20/20) [Figure 2]. No recurrence of ocular manifestations were detected during the follow-up period until now and thus we ruled out other problem like JRA.
Figure 2.
Decreased vitreous haziness after two weeks of treatment
DISCUSSION
Brucellosis presents with a various ranges and often with the presence of non-specific clinical signs and symptoms including ocular manifestations. In a cohort study performed in Turkey, ocular involvements were detected in 21% of brucellosis patient. The most frequent manifestation was anterior uveitiis followed by choroiditis and panuveitis.[10]
In one study from Peru, the most frequent manifestation of ocular brucellosis was reported to be uveitis, mostly posterior uveitis.[1] In our case, ocular manifestations were presented as episcleritis, panuveitis, and chorioretinitis. Furthermore, ocular damage occurs mainly in chronic phase of the disease, just as in this case.
Woods and Rolando concluded, ocular brucellosis is a rare disease occurring among children (0.003%)[1] and our patient was seven years and further being a child.
Woods and Rolando mentioned that the host-pathogen interaction of human and Brucella species occurs through two mechanisms: Direct invasion of the ocular tissue by the microorganism through sending septic emboli to the uveal tissue, and by formation of immunoglobulin and circulating complexes. In the above mentioned studies, improvement in visual acuity was seen with systemic steroid, which supports the interposition of immune components in ocular manifestations of brucellosis.[1,11] It seems that in our present case, the second mechanism has the main role, since the signs and symptoms have started to disappear after steroid therapy.
CONCLUSION
We conclude that uveitis may be a manifestation of the brucellosis and the treatment forthis systemic disease is needed for preventing systemic complications, and also examination of eyes in brucellosis patients must always be done by the clinicians working in this field. Hence early treatment is very important for preventing permanent visual loss and the other complications of ocular brucellosis.
AUTHORS’ CONTRIBUTIONS
All authors have contributed in designing and preparation of the first draft of the manuscript. All authors have read and approved the content of the manuscript and confirmed the accuracy or integrity of any part of the work.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Rolando I, Olarte L, Vilchez G, Lluncor M, Otero L, Paris M, et al. Ocular manifestations associated with brucellosis: A 26-year experience in Peru. Clin Infect Dis. 2008;46:1338–45. doi: 10.1086/529442. [DOI] [PubMed] [Google Scholar]
- 2.Zeinalian Dastjerdi M, Fadaei Nobari R, Ramazanpour J. Epidemiological features of human Brucellosis in central Iran, 2006-2011. Public Health. 2012;126:1058–62. doi: 10.1016/j.puhe.2012.07.001. [DOI] [PubMed] [Google Scholar]
- 3.Andriopoulos P, Tsironi M, Deftereos S, Aessopos A, Assimakopoulos G. Acute Brucellosis: Presentation, diagnosis, and treatment of 144 cases. Int J Infect Dis. 2007;11:52–7. doi: 10.1016/j.ijid.2005.10.011. [DOI] [PubMed] [Google Scholar]
- 4.Ariza J, Corredoira J, Pallares R, Viladrich PF, Rufi G, Pujol M, et al. Characteristics of and risk factors for relapse of Brucellosis in humans. Clin Infect Dis. 1995;20:1241–9. doi: 10.1093/clinids/20.5.1241. [DOI] [PubMed] [Google Scholar]
- 5.Gómez MC, Nieto JA, Rosa C, Geijo P, Escribano MA, Muñoz A, et al. Evaluation of seven tests for diagnosis of human Brucellosis in an area where the disease is endemic. Clin Vaccine Immunol. 2008;15:1031–3. doi: 10.1128/CVI.00424-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Young EJ. An overview of human Brucellosis. Clin Infect Dis. 1995;21:283. doi: 10.1093/clinids/21.2.283. [DOI] [PubMed] [Google Scholar]
- 7.Khuri-Bulos NA, Daoud AH, Azab SM. Treatment of childhood Brucellosis: Results of a prospective trial on 113 children. Pediatr Infect Dis J. 1993;12:377–81. doi: 10.1097/00006454-199305000-00005. [DOI] [PubMed] [Google Scholar]
- 8.Lubani MM, Dudin KI, Sharda DC, Ndhar DS, Araj GF, Hafez HA, et al. A multicenter therapeutic study of 1100 children with Brucellosis. Pediatr Infect Dis J. 1989;8:75–8. [PubMed] [Google Scholar]
- 9.Bosilkovski M. Clinical manifestations, diagnosis, and treatment of brucellosis. UpToDate. 2014. Jan, [Last accessed on 2013 Sept 13]. available in http://www.uptodate.com/contents/clinical-manifestations-diagnosis-and-treatment-of-brucellosis?
- 10.Sungur GK, Hazirolan D, Gurbuz Y, Unlu N, Duran S, Duman S. Ocular involvement in brucellosis. Can J Ophthalmol. 2009;44:598–601. doi: 10.3129/i09-019. [DOI] [PubMed] [Google Scholar]
- 11.Woods A. Experimental brucellar uveitis. Am J Ophthalmol. 1953;36:1025–42. doi: 10.1016/0002-9394(53)91883-2. [DOI] [PubMed] [Google Scholar]