

Abstract
Background
Digit sucking, tongue thrust swallowing, and mouth breathing are potential risk factors for development of malocclusion. The purpose of this study was to verify the prevalence of different occlusal traits among 5–7-year-old children and assess their relationship with oral habits.
Material/Methods
The study included 503 pre-school children (260 boys and 243 girls) with a mean age of 5.95 years. Different occlusal traits were verified by intraoral examination. Oral habits were diagnosed using data gathered from clinical examination of occlusion and extra-oral assessment of the face, combined with a questionnaire for parents.
Results
The study demonstrated that 71.4% of the children presented with 1 or more attributes of malocclusion and 16.9% had oral habits. The vertical and sagittal malrelation of incisors, as well as spacing, were the predominant features.
This study showed that digit suckers have higher incidence of anterior open bite (P=0.013) and posterior crossbite (P=0.005). The infantile type of swallowing demonstrated strong association (P=0.001) with anterior open bite.
Conclusions
Non-nutritive sucking habits and tongue thrust swallowing are significant risk factors for the development of anterior open bite and posterior crossbite in pre-school children.
MeSH Keywords: Child, Preschool, Dental Occlusion, Tongue Habits
Background
Malocclusion is common in children and prevalence in different age groups ranges from 20% to 93% [1–4]. Most epidemiological studies of occlusion traits are concentrated on the permanent dentition [5]. Studies assessing the deciduous and mixed dentition stages, when interceptive treatment and developing occlusion guidance measures are typically prescribed, are much less common. Nevertheless, some studies reported that as early as 3 years of age prevalence of malocclusion is as high as 70–82.5% [3,6,7]. Among pre-school children, the most common conditions are anterior open bite (AOB), excessive overjet (OJ), Class II malocclusions, and posterior crossbite (CB) [3,6,8,9].
Malocclusions are believed to be caused by a combination of inherited and environmental factors acting together. Oral habits are among the most evident examples of environmental etiology of malocclusion [10,11]. It is well accepted that nonnutritive sucking habit persisting beyond 3 years of age are implicated in the development of AOB [3,12]. However, data on the prevalence of oral habits among pre-school children are inconsistent and ranges from 1.1% to 67.9% [13–16]. This could be because most of these studies used retrospective questionnaires to characterize the presence or absence of oral habits. The use of a single retrospective questionnaire makes it difficult for parents to accurately assess the presence of habits, and, in turn, makes it difficult to estimate their effects on occlusion. The validity of such data is somewhat questionable [9].
Since oral habits like digit sucking, tongue thrust swallowing, and mouth breathing are modifiable factors, reliable data and knowledge of how such behaviors contribute to malocclusion is important for its cessation and prevention [17].
The purpose of this study was to determine the prevalence of different occlusal traits among 5–7-year-old pre-school children and assess their relationship with oral habits, using data gathered from clinical examination of occlusion and extra-oral assessment of the face, combined with a questionnaire for parents.
Material and Methods
The study was approved by Bioethics Committee of the Lithuanian University of Health Sciences (No. 2003-87/03).
Subjects
The inclusion criteria were as follow. Subjects should: 1) be 5–7 years old; 2) have central permanent or deciduous incisors; 3) be non-syndromic and non-cleft patients; and 4) have no history of orthodontic treatment.
The sample size calculation was based on data from a study by Warren et al. [9], which was chosen because it consisted of children in mixed dentition stages and analyzed relationships between non-nutritive sucking habits and occlusion. They found a 55% prevalence of malocclusion and 51% of children had a predominant digit-sucking habit at the early mixed dentition stage. Assuming prevalence of malocclusion and oral habits as not less than 50%, the sample size calculation indicated that 384 subjects would be sufficient to detect a prevalence of malocclusion and sucking habit with a power of 95% (alpha <0.05).
Clinical examination
All clinical examinations were made by the same investigator (KK) in the nursery room of selected kindergartens in natural daylight, using latex gloves, a sterile dental mouth mirror, and an orthodontic ruler. Registration of the occlusal characteristics was carried out according to the principles developed by the Federation Dentaire Internationale [18], consisting of an objective measurement of the occlusal traits. This method has been adapted to the primary dentition and a brief description is outlined below.
Incisal segments (Figure 1)
Figure 1.
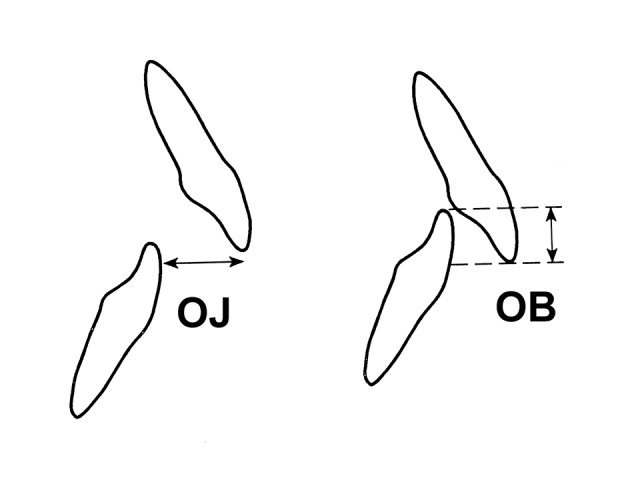
Relationship of incisors: OJ (overjet) – sagittal overlap, OB (overbite) – vertical overlap.
The OJ at the level of the central incisors was measured by a metric ruler to the closest millimeter. The amount of vertical overlap of the upper incisors on the lower incisors was marked with a pencil and measured with a metric ruler to the closest millimeter. The amount of AOB was measured directly.
Lateral segments (Figure 2)
Figure 2.
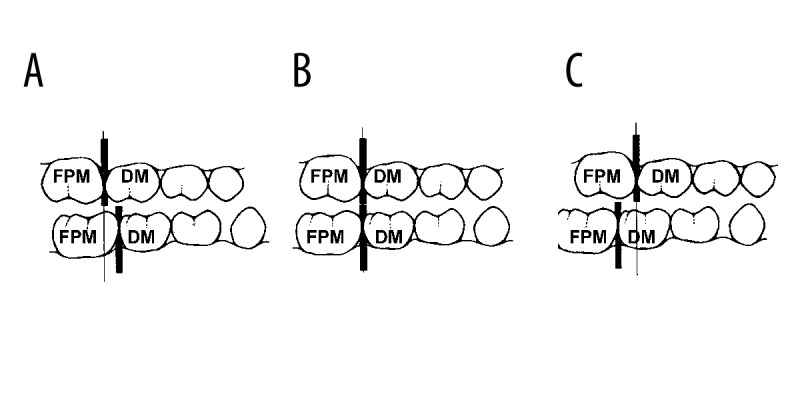
Sagittal relationship of the molars. FPM – first permanent molar, DM – deciduous molar. (A) Mesial step of DM and Angle Class I of FPM. (B) Flash terminal plane of DM. (C) Distal step of DM and Angle Class II of FPM.
Sagittal relationship of first permanent molars was evaluated according to Angle classification. Terminal plane relationship of deciduous second molars was measured between perpendicular projections on the occlusal plane, from the distal surfaces of the maxillary and mandibular second deciduous molars. A flush terminal plane was considered when the distance between perpendiculars was less than 1 mm in either direction. A difference equal to 1 mm or more was classified as distal or a mesial step, depending of the direction of the deviation. The relationship was not assessed in case of prematurely lost second deciduous molars.
The transverse relation of the lateral segments was measured by direct inspection: 1 of 3 separate relationships was recorded: (i) normal relationship; (ii) buccal crossbite; and (iii) lingual crossbite. The existence of a buccal or lingual crossbite was registered each time 1 or several teeth in the lateral segment were involved. Upper midline shift was registered if the midline was displaced by at least 1 mm (Figure 3).
Figure 3.
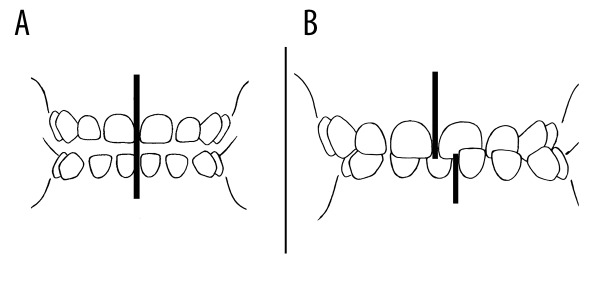
(A) Normal dental midline. (B) Dental midline shift.
Spacing exceeding 1 mm was registered as present.
Oral habits were diagnosed using methods validated by other studies assessing data from the parents’ questionnaire [19,20] and updated by extra-oral examination of the face. Mouth-breathing patterns and thumb-sucking were diagnosed only if our clinical examination indicated and parents confirmed the presence of those habits in the questionnaires.
Mouth breathing
Extraoral observation of the face was completed in a relaxed position of the children (watching a cartoon movie). Lip incompetence at rest, the tension of the oral muscles while closing the lips, and dilated nostrils when asked to breath through the nose were considered for a diagnosis of mouth-breathing.
Digit sucking
This non-nutritive sucking habit was diagnosed after inspection of the fingers to see if they were asymmetric or had other signs indicating persisting sucking.
Infantile type of swallowing
Hyper-activity of the perioral muscles and the tongue protrusion between upper and lower incisors or cuspids with no molar contact during swallowing was registered as infantile swallowing. The children were asked to swallow their saliva 3 times during the same visit. When in doubt, another swallow was requested until the observer was satisfied with the judgment.
Statistics
Intra-observer method error was tested by examining 50 randomly selected children in the 3 kindergartens twice. Quantitative measurements (OJ, OB) were analyzed using a method suggested by Bland and Altman [21] and an unweighted kappa statistics for the categorical data.
The absolute and percentage frequencies were obtained for data analysis. Chi-square analysis was used for binary variables and an odds ratio with a 95% confidence interval was calculated to measure the strength of associations for binary variables. Each sagittal, vertical, and transverse occlusal trait was dichotomized in contrast with the others and correlated with oral habits. The level of probability was set at alpha=0.05. Differences in probabilities of less than 5% (P<0.05) were considered to be statistically significant.
Results
The initial sample consisted of 709 children registered in 17 kindergartens. Parents of 101 children refused to participate in the study; 64 children were absent on the day of the examination; 37 children were excluded from the study because of not fully erupted, decayed, or missing central incisors; and 4 because of using pre-orthodontic trainers. Thus, 503 children (mean age of 5.95±0.61 years) participated in the study.
The intra-observer agreement for the presence of posterior crossbite, terminal plane of second deciduous molars and spacing was excellent (unweighted kappa=0.91, 0.86 and 0.89, respectively), and was good for oral habits (unweighted kappa was not less than=0.79). The error of measurements given in ±2SD of the differences between the repeated measurements was ±0.68 mm for OJ and ±0.42 mm for OB and was considered to be not clinically significant.
The study demonstrated that 71.4% of the children presented with 1 or more attributes of malocclusion and 16.9% had oral habits. The prevalence of occlusal traits is presented in Table 1. The vertical and sagittal malrelation of incisors was a predominant feature. Overjet exceeding 2 mm was found in almost half and increased overbite (>3 mm) was found in 31.0% of the subjects. The 4 fully erupted permanent molars were found in only 21.9% of children. Class I and Class II molar relationship was equally distributed in the sample and Class III was registered in only 4 subjects. Spacing was a common feature in the study group. Analysis of interrelationship between different occlusal characteristics demonstrated that the only statistically significant correlation was between the distal terminal plane of deciduous molars and increased overjet (P=0.001). The chi-squared test confirmed that there is no evidence (P>0.05) to suggest a difference in prevalence of occlusal traits and oral habits between genders, except for posterior CB (P=0.03) and infantile swallowing (P=0.01), which were more frequent in girls.
Table 1.
The prevalence of malocclusion and differences between genders.
| Occlusal traits | Total | Boys | Girls | P | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |||
| Sagittal relationship | ||||||||
| Incisors (OJ) | ||||||||
| Edge-to-edge | 47 | 9.3 | 27 | 10.4 | 20 | 8.2 | NS* | |
| 0–2 mm | 205 | 40.8 | 106 | 40.7 | 99 | 40.8 | NS* | |
| >2 mm | 232 | 46.1 | 119 | 45.8 | 113 | 46.5 | NS* | |
| < 0 mm | 19 | 3.8 | 8 | 3.1 | 11 | 4.5 | NS* | |
| Deciduous molars | ||||||||
| Right side | PLDM | 19 | 3.8 | 12 | 4.6 | 7 | 2.9 | NS* |
| MS | 262 | 52.1 | 134 | 51.5 | 128 | 52.7 | NS* | |
| DS | 125 | 24.9 | 66 | 25.4 | 59 | 24.3 | NS* | |
| FTP | 97 | 19.3 | 48 | 18.5 | 49 | 20.2 | NS* | |
| Left side | PLDM | 22 | 4.4 | 13 | 5.0 | 9 | 3.7 | NS* |
| MS | 243 | 48.3 | 131 | 50.4 | 112 | 46.1 | NS* | |
| DS | 125 | 24.9 | 59 | 22.7 | 66 | 27.2 | NS* | |
| FTP | 113 | 22.5 | 57 | 21.9 | 56 | 23.0 | NS* | |
| Permanent molars | ||||||||
| Right side | Not erupted | 393 | 78.1 | 204 | 78.5 | 189 | 77.8 | NS* |
| Class I | 52 | 10.3 | 30 | 11.5 | 22 | 9.1 | NS* | |
| Class II | 54 | 10.7 | 24 | 9.2 | 30 | 12.3 | NS* | |
| Class III | 4 | 0.8 | 2 | 0.8 | 2 | 0.8 | NS* | |
| Left side | Not erupted | 391 | 77.7 | 201 | 77.3 | 190 | 78.2 | NS* |
| Class I | 55 | 10.9 | 33 | 12.7 | 22 | 9.1 | NS* | |
| Class II | 53 | 10.5 | 24 | 9.2 | 29 | 11.9 | NS* | |
| Class III | 4 | 0.8 | 2 | 0.8 | 2 | 0.8 | NS* | |
| Vertical relationship of incisors (OB) | ||||||||
| Edge-to-edge | 45 | 9.0 | 28 | 10.8 | 17 | 7.0 | NS* | |
| 1–3 mm | 289 | 57.4 | 151 | 58.0 | 138 | 56.8 | NS* | |
| >3 mm | 156 | 31.0 | 78 | 30.0 | 78 | 32.1 | NS* | |
| <0 mm | 13 | 2.6 | 3 | 1.2 | 10 | 4.1 | NS* | |
| Transversal relationship | ||||||||
| Incisors | Normal | 393 | 78.1 | 211 | 81.2 | 182 | 74.9 | NS* |
| Midline shift | 110 | 21.9 | 49 | 18.8 | 61 | 25,1 | NS* | |
| Molars | Normal | 468 | 93.0 | 245 | 94.2 | 223 | 91.8 | NS* |
| BCB | 34 | 6.8 | 14 | 5.4 | 20 | 8.2 | 0.03 | |
| LCB | 1 | 0.2 | 1 | 0.4 | 0 | 0.0 | NS* | |
| Spacing | ||||||||
| No spaces | 30 | 5.9 | 8 | 3.1 | 22 | 9.1 | NS* | |
| Diastema | 264 | 52.5 | 140 | 53.8 | 124 | 51.0 | NS* | |
| Other spaces | 209 | 41.6 | 112 | 43.1 | 97 | 39.9 | NS* | |
The difference between genders with a P>0.05 value is not statistically significant (NS).
OJ – overjet; OB – overbite; PLDM – prematurely lost deciduous molars; MS – mesial step; DS – distal step; FTP – flash terminal plane; BCB –buccal crossbite; LCB – lingual crossbite.
Table 2 depicts the prevalence of oral habits. Almost one-fifth of the children had oral habits. The most frequent was mouth-breathing (10.1%).
Table 2.
The prevalence of oral habits and distribution between genders.
| Oral habits | Total | Boys | Girls | P | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | ||
| Normal functions | 418 | 83.1 | 219 | 84.2 | 199 | 81.9 | NS* |
| Mouth-breathing | 51 | 10.1 | 32 | 12.3 | 19 | 7.8 | NS* |
| Infantile-swallowing | 27 | 5.4 | 7 | 2.7 | 20 | 8.2 | 0.01** |
| Finger sucking | 7 | 1.4 | 2 | 0.8 | 5 | 2.1 | NS* |
The difference between genders with a P>0.05 value is not statistically significant (NS).
Infantile swallowing is more frequent in girls than in boys (P=0,01). The difference is statistically significant.
Effect of the oral habits on the dentition. This study showed that digit suckers have higher incidence of AOB (P=0.013) and posterior CB (P=0.005). Children with infantile type of swallowing had a significantly higher prevalence of AOB (P=0.001). Associations were also found between mouth breathing and formation of molar Class III sagittal relationship (P=0.027).
Discussion
The present study aimed to provide detailed insight into the prevalence of clinically relevant occlusal traits and their relationship with oral habits at the early occlusion development stages. An effort was made to ensure accuracy of oral habit diagnostics, based not only on a questionnaire for parents, but also on clinical observation. For results showing consistency, the STROBE Statement checklist was used [22].
Studies on the prevalence of occlusal anomalies in the age group of 5–7-year-olds are rare and results vary greatly, from 36% to almost 80% [3,4,23]. We found that 71.4% of children had some kind of abnormal occlusal trait. The inconsistency of results between different studies might be due to a different incidence of malocclusion between populations, but also due to different methods of malocclusion registration. The most precise and reliable method to evaluate occlusal traits is measurement on articulated study models, as in the study by Warren et al. [9], who found that 55% of children had malocclusion. We did not use study models due to the very young age of the children in the study sample. The higher prevalence of malocclusion in our study (71.4% vs. 55%) can probably be explained by the different mean age of the study samples (5.95 vs. 8.6 years), as we must consider possible self-correction of some occlusal traits with growth at later developmental stages [3].
Our study shows that digit sucking has an impact on occlusal development, and a statistically significant association was found with AOB and posterior CB. Such findings are not surprising, as numerous studies [9,10,12,13,16,19,24] have linked non-nutritive sucking habits to malocclusion. However, in contrast to previous data indicating prevalence of non-nutritive sucking habits as high as 51.0% [9] or even 88% [3], we found it only in 1.4% of the study sample. This discrepancy could be explained at least by 2 reasons. First, in our study, sucking habit was validated only when results from the parents’ questionnaire and clinical observation were concordant. Almost all other studies were based mainly on a parents’ questionnaire [6,11,13–15]. We found that disagreement between the parents’ questionnaire and clinical observation establishing diagnosis of digit sucking was 28.5% and 19.6% for mouth breathing. Thus, only results from self-reported data can be questioned. Secondly, our study sample composition depended on the willingness of the children and their parents to join the study. Most available reports [3,4,10] on oral habits used data from routine longitudinal medical studies, in which information about these habits was collected along with the other data and were not focused on oral conditions. The participation of volunteers might be a source of bias in the study, because it can be speculated that parents with malocclusion were more motivated to take part in the study. On the other hand, very concerned parents could have already consulted an orthodontist and decided to refuse to participate. This self-selection could have affected the representativeness of the sample, but it is difficult to assess the direction and magnitude of its influence. We believe the relatively large sample size allowed us to reduce this type of bias to a minimum.
We found that mouth breathing was the most prevalent condition (10.1%) with a possible potential negative effect on occlusion (molar Class III sagittal relationship). This is in agreement with many other studies, because nasal obstruction and mouth breathing have proven negative effects on development of the cranio-facial complex [25,26]. However, it should be borne in mind that we found only 4 children with molar Class III, so these associations should be interpreted with caution.
The infantile type of swallowing was established in 5.4% of the sample. The role of infantile swallowing for AOB formation is not clear. The prevalent opinion is that duration of the pressure of the tongue on the anterior teeth during swallowing is too short to have an influence on the eruption of anterior teeth, and therefore the formation of AOB [27,28]. According to Proffit [28], AOB itself is more likely to cause the infantile swallowing pattern rather than vice versa. In contrast, the ultrasonography assesment of swallowing type provided data indicating that infantile swallowing is an important factor for AOB formation [29]. We found that tongue thrust swallowing is associated with AOB formation (P=0.001) and this in agreement with recent reports [30]. Tongue thrust swallowing has been assumed to be a contributing factor in the relapse of orthodontic treatment results and should be controlled during the treatment and retention periods [31].
The important advantage of the present study is the accuracy of oral habit registration, based not only on the questionnaire for parents, but also on clinical observation. Without this attention to the details of clinical assessment, prevalence of oral habits may not reflect everyday dental practice. From a clinical standpoint, our results suggest that prevalence of some habits, like digit sucking, might be overestimated and conditions such as mouth breathing may be overlooked. Therefore, further studies are warranted on even larger populations, in order to produce consistent and clinically relevant data.
Conclusions
The prevalence of malocclusion among 5–7-year-old pre-school children is 71.4%.
There was a significant association between sucking habits and anterior open bite, as well as posterior crossbite. Tongue thrust swallowing is more likely to be a contributing factor for anterior open bite development.
Footnotes
Source of support: Departmental sources
References
- 1.Ciuffolo F, Manzoli L, D’Attilio M, et al. Prevalence and distribution by gender of occlusal characteristics in a sample of Italian secondary school students: a cross-sectional study. Eur J Orthod. 2005;27:601–6. doi: 10.1093/ejo/cji043. [DOI] [PubMed] [Google Scholar]
- 2.Baubiniene D, Sidlauskas A, Miseviciene I. The need for orthodontic treatment among 10–11 and 14–15-year-old Lithuanian schoolchildren. Medicina (Kaunas) 2009;45:814–21. [PubMed] [Google Scholar]
- 3.Dimberg L, Lennartsson B, Soderfeldt B, Bondemark L. Malocclusions in children at 3 and 7 years of age: a longitudinal study. Eur J Orthod. 2013;35:131–37. doi: 10.1093/ejo/cjr110. [DOI] [PubMed] [Google Scholar]
- 4.Gois E, Vale M, Paiva S, et al. Incidence of malocclusion between primary and mixed dentitions among Brazilian children. A 5-year longitudinal study. Angle Orthod. 2012;82:495–500. doi: 10.2319/033011-230.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Sidlauskas A, Lopatiene K. The prevalence of malocclusion among 7–15-year-old Lithuanian schoolchildren. Medicina (Kaunas) 2009;45:147–52. [PubMed] [Google Scholar]
- 6.Kohler L, Holst K. Malocclusion and sucking habits of four-year-old children. Acta Paediatr Scand. 1973;62:373–79. doi: 10.1111/j.1651-2227.1973.tb08122.x. [DOI] [PubMed] [Google Scholar]
- 7.Ravn J. Occlusion in the primary dentition in 3-year-old children. Scand J Dent Res. 1975;83:123–30. doi: 10.1111/j.1600-0722.1975.tb01189.x. [DOI] [PubMed] [Google Scholar]
- 8.Thilander B, Myrberg N. The prevalence of malocclusion in Swedish schoolchildren. Scand J Dent Res. 1973;81:12–21. doi: 10.1111/j.1600-0722.1973.tb01489.x. [DOI] [PubMed] [Google Scholar]
- 9.Warren J, Slayton L, Yonesu T, et al. Effects of nonnutritive sucking habits on occlusal characteristics in the mixed dentition. Pediatr Dent. 2005;27:445–50. [PubMed] [Google Scholar]
- 10.Klocke A, Nanda R, Kahl-Nieke B. Anterior open bite in the deciduous dentition: Longitudinal follow-up and craniofacial growth considerations. Am J Orthod Dentofacial Orthop. 2002;122:353–58. doi: 10.1067/mod.2002.126898. [DOI] [PubMed] [Google Scholar]
- 11.Mistry P, Moles D, O’Neill J, Noar J. The occlusal effects of digit sucking habits amongst school children in Northamptonshire (UK) J Orthod. 2010;37:87–92. doi: 10.1179/14653121042939. [DOI] [PubMed] [Google Scholar]
- 12.Svedmyr B. Dummy sucking. A study of its prevalence, duration and malocclusion consequences. Swed Dent J. 1979;3:205–10. [PubMed] [Google Scholar]
- 13.Quashie-Williams R, DaCosta O, Isiekwe M. Oral habits, prevalence and effects on occlusion of 4–15 year old school children in Lagos, Nigeria. Nigerian Postgrad Med J. 2010;17:113–17. [PubMed] [Google Scholar]
- 14.Shetty S, Munshi A. Oral habits in children-a prevalence study. J Indian Soc Pedod Prev Dent. 1998;16:61–66. [PubMed] [Google Scholar]
- 15.Kharbanda O, Sidhu S, Sundaram K, Shukla D. Oral habits in school going children of Delhi: a prevalence study. J Indian Soc Pedod Prev Dent. 2003;21:120–24. [PubMed] [Google Scholar]
- 16.Farsi N, Salama F. Sucking habits in Saudi children: prevalence, contributing factors and effects on the primary dentition. Pediatric Dent. 1997;19:28–33. [PubMed] [Google Scholar]
- 17.Vig K, Fields H. Facial growth and management of orthodontic problems. Pediatr Clin North Am. 2000;47:1085–123. doi: 10.1016/s0031-3955(05)70259-5. [DOI] [PubMed] [Google Scholar]
- 18.Baum L, Horowitz H, Summers C, et al. A method for measuring occlusal traits. Intern Dent J. 1973;23:530–37. [Google Scholar]
- 19.Ovsenik M. Incorrect orofacial functions until 5 yearsof age and their association with posterior crossbite. Am J Orthod Dentofacial Orthop. 2009;136:375–81. doi: 10.1016/j.ajodo.2008.03.018. [DOI] [PubMed] [Google Scholar]
- 20.Jalaly T, Ahrari F, Amini F. Effect of togue thrust swallowing on position of anterior teeth. J Dent res Dent Clin Dent Prospects. 2009;3:73–77. doi: 10.5681/joddd.2009.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Bland J, Altman D. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet. 1986;1:307–10. [PubMed] [Google Scholar]
- 22.von Elm E, Altman D, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. PloS Med. 2007;4(10):e296. doi: 10.1371/journal.pmed.0040296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Johannsdottir B, Wisth P, Magnusson T. Prevalence of malocclusion in 6 year old Icelandic children. Acta Odontol Scand. 1997;55:398–402. doi: 10.3109/00016359709059206. [DOI] [PubMed] [Google Scholar]
- 24.Katz C, Rosenblatt A, Gondim P. Nonnutritive sucking habits in Brazilian children: effects on deciduous dentition and relationship with facial morphology. Am J Orthod Dentofacial Orthop. 2004;126:53–57. doi: 10.1016/j.ajodo.2003.06.011. [DOI] [PubMed] [Google Scholar]
- 25.Gois E, Ribeiro-Junior H, Vale M, et al. Influence of nonnutritive sucking habits, breathing pattern and adenoid size on the development of malocclusion. Angle Orthod. 2008;78:647–54. doi: 10.2319/0003-3219(2008)078[0647:IONSHB]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 26.Souki B, Pimenta G, Souki M, et al. Prevalence of malocclusion among mouth breathing children: do expectations meet reality? Int J Pediatr Otorhinolaryngol. 2009;73:767–73. doi: 10.1016/j.ijporl.2009.02.006. [DOI] [PubMed] [Google Scholar]
- 27.Mason RM. Myths that persist about orofacial myology. Int J Orofacial Myology. 2011;37:26–38. [PubMed] [Google Scholar]
- 28.Proffit W, Fields H, Sarver D. Contemporary orthodontics. Mosby/Elsevier; St Louis, Mo, Edinburgh: 2007. pp. 153–54. [Google Scholar]
- 29.Peng C, Jost-Brinkmann P, Yoshida N, et al. Differential diagnosis between infantile and mature swallowing with ultrasonography. Eur J Orthod. 2003;25:451–56. doi: 10.1093/ejo/25.5.451. [DOI] [PubMed] [Google Scholar]
- 30.Dixi U, Shetty R. Comparison of soft-tissue, dental, and skeletal characteristics in children with and without tongue thrusting habit. Contemp Clin Dent. 2013;4:2–6. doi: 10.4103/0976-237X.111585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Yashiro K, Takada K. Tongue muscle activity after orthodontic treatment of anterior open bite: a case report. Am J Orthod Dentofacial Orthop. 1999;115:660–66. doi: 10.1016/s0889-5406(99)70292-1. [DOI] [PubMed] [Google Scholar]