

Abstract
Secure e-mailing between Kaiser Permanente physicians and patients is widespread; primary care providers receive an average of 5 e-mails from patients each workday. However, on average, secure e-mailing with patients has not substantially impacted primary care provider workloads. Secure e-mail has been associated with increased member retention and improved quality of care. Separate studies associated patient portal and secure e-mail use with both decreased and increased use of other health care services, such as office visits, telephone encounters, emergency department visits, and hospitalizations. Directions for future research include more granular analysis of associations between patient-physician secure e-mail and health care utilization.
Keywords: communication, electronic health record, electronic mail
WITH THE ADVENT of electronic health records (EHRs) and patient portals, physicians and patients are experiencing fundamental changes in care modalities. Under meaningful use regulation and incentives, more physicians and health care organizations are beginning to experience the promises of these technologies (Centers for Medicare & Medicaid Services, 2012).
Kaiser Permanente is farther along than many health care organizations in incorporating an integrated EHR and associated functionalities, such as secure patient-physician electronic mail, into ambulatory care. KP HealthConnect™. Kaiser Permanente's EHR, has been available in ambulatory care in all regions since early 2008, and secure patient-physician e-mail has been available since 2009. Fully 49% of recorded encounters between primary care providers (PCPs) and patients at Kaiser Permanente occur virtually—16% by telephone and 33% through secure e-mail (internal data). The EHR increases the utility of telephone encounters by making all relevant patient data readily available to PCPs and helps create a more complete clinical context. However, this report focuses on virtual care that occurs via secure e-mail between physicians and patients.
The use of secure e-mail to provide ambulatory care raises important questions about quality, patient satisfaction, provider workloads, and utilization of other health care services. In this report, we outline what is currently known at Kaiser Permanente about secure e-mail between physicians and patients and describe the focus of our future efforts to assess the impact on value and quality of this important care modality.
SECURE E-MAIL BETWEEN PHYSICIANS AND PATIENTS AT KAISER PERMANENTE
Secure e-mail occurs through a patient portal (kp.org) integrated with KP HealthConnect. To securely message providers through the patient portal, Kaiser Permanente members must first register and be authenticated; in September 2013, 47% of Kaiser Permanente members had done so. In the third quarter of 2013, 27% of all portal-registered members sent 1 or more secure e-mail messages to physicians and other providers; an average of 873 e-mails were sent per 1000 registered members.
EFFECT OF SECURE E-MAILING WITH PATIENTS ON QUALITY OF CARE
A 2010 Kaiser Permanente study examined the effect of secure patient-physician e-mail on 9 Healthcare Effectiveness Data and Information Set (HEDIS) effectiveness of care measures for diabetes and hypertension (Zhou et al., 2010). The population included more than 35 000 adult members in the Kaiser Permanente Southern California region who used secure e-mail with their PCPs during a retrospective observation period that began 2 years before secure e-mail was available in the region and ended 23 months after it became available to all members. The effect on HEDIS scores of secure e-mail between PCPs and patients was analyzed using regression modeling and a matched-control analysis. In the latter, patients who used secure e-mail with their physicians and patients who had not used secure e-mail were matched by their baseline status on HEDIS measures, age, gender, PCP, and diagnostic cost group score. Within each matched pair, the rates at which 9 HEDIS measures were met 2 months after patients began using secure e-mail with providers were compared.
Results
In the regression analysis, use of secure patient-physician e-mail was associated with improved performance for each HEDIS measure, and performance improvements on individual measures ranged from 4.0% to 11.1%. In the matched-control analysis, secure patient-physician e-mail was associated with statistically significant performance improvements on 7 of 9 measures. A slight improvement in tighter (<130/80 mm Hg) blood pressure control among members with diabetes did not achieve statistical significance, and, among patients with hypertension but not diabetes, performance on the HEDIS hypertension control measure was similar in secure e-mail users and nonusers. The results also suggested a possible association between more e-mail with physicians and better quality; compared to a single thread, 2 or more secure patient-physician e-mail threads in a 2-month period was associated with a greater likelihood of better performance on 4 measures (glycemic screening and control and low-density lipoprotein cholesterol and nephropathy screening).
Interpretation
Use of secure e-mail between physicians and patients was associated with improved performance on HEDIS effectiveness of care measures, but the mechanisms underlying this association are unclear. They may include increasing continuity of care, patient-physician connectedness, and supporting patient self-management. In addition, secure messaging takes place on the patient portal, where patients can also refill prescriptions using a mail-order pharmacy and view laboratory results, medication lists, and educational material; the impact of these functionalities in improving patient outcomes is inseparable from that of secure messaging. For instance, refilling prescriptions online is associated with better medication adherence, which is likely to affect outcomes (Duru et al., 2010; Sarkar et al., 2014). However, as 1 Kaiser Permanente member participating in a focus group on secure messaging stated, “I feel more in control over my medical condition. I have access to information, access to people I need to consult with, so it puts me back in charge.”
EFFECT OF PATIENT PORTAL USE ON MEMBER LOYALTY
A 2012 Kaiser Permanente study examined the association between patient portal use—in which secure e-mail with physicians is a key functionality—and membership retention (Turley et al., 2012). Among a retrospective cohort of more than 394 000 Kaiser Permanente Northwest members, researchers examined differences in voluntary (unrelated to loss of employer-provided health insurance benefits) membership retention rates between those who did and did not use the patient portal, using propensity score matching to control for bias. Independent variables used to develop propensity scores included age, gender, length of membership in years, membership type (ie, subscriber, spouse/partner, or dependent), illness burden, and the presence of diabetes and hypertension. Approximately 142 000 members who used the patient portal and an equivalent number of members who did not use it were matched one-to-one by their propensity scores, and differences in retention rates were evaluated. Logistic regression modeling assessed the relative effect of variables on retention.
Results
Retention rates were 96.9% for patient portal users (95% confidence interval [CI], 96.8%-97.0%) and 90.5% for nonusers (95% CI, 90.4%-90.6%; P < .0001). In logistic regression analysis, portal users were 2.6 times more likely to remain members of Kaiser Permanente than were nonusers (95% CI, 2.5-2.7). Differences in retention rates varied with membership tenure. For members with less than 1 year of membership, the retention rate among those who used the portal was 10 percentage points higher than among those who did not use the portal; at 1 to 3 years of membership, the difference in retention rates was 8 percentage points. For members with at least 3 but less than 10 years of membership, the difference in retention rates between patient portal users and nonusers was 3 percentage points. Finally, for members with 10 or more years of membership, the difference in retention rates was less than 2 percentage points.
Interpretation
Members who used the patient portal were more likely to remain members of Kaiser Permanente than were those who did not use the portal—and the effect of portal use on member retention decreased as the length of membership increased. The mechanisms by which patient portal use is associated with higher member retention are unknown, but evidence exists as to consumer preferences for online access to their health information and to e-mailing providers (Fricton & Davies, 2008; Patel et al., 2012; Wen et al., 2010). More than 70% of patients want to use electronic communication with health care providers, and provider-patient electronic communication enables greater patient engagement, leading to improved outcomes and efficiency (Dentzer, 2013; Schickedanz et al., 2013; Seidman & Eytan, 2008; Tagalicod, 2013).
EFFECT OF SECURE E-MAIL WITH PATIENTS ON PHYSICIAN WORKLOADS
We examined the volume of secure patient-physician e-mail and provider response rates and times for patient-initiated e-mail in 7 Kaiser Permanente regions from January through June 2012. We defined a secure e-mail as a single electronic message between patient and provider sent through the patient portal and a secure e-mail thread as including initial and subsequent e-mail messages between provider and patient. Secure e-mail encounters include both threads and individual e-mail messages.
We included 3176 PCPs: physicians, nurse practitioners, and physician assistants in family practice, internal medicine, pediatrics, and obstetrics/gynecology. Their patient panels included an average of 1476 individuals. We excluded PCPs with fewer than 500 patients. Some PCPs responded directly to patient-initiated e-mail; others used a triage model in which registered nurses and medical assistants on their teams responded to e-mail within their scopes of practice. We did not distinguish between these models; unless otherwise specified, “PCP teams” refers to both physicians responding to e-mail and teams—physicians, registered nurses, and medical assistants—doing the same.
We used Pearson correlation coefficient to examine correlations between message volumes and response times. We analyzed response times by physicians only and by PCP teams. For these analyses alone, we excluded physicians who handled a daily average of less than 1 or more than 16 (>2 standard deviations above the mean) secure e-mails with patients and PCP teams that handled a daily average of less than 1 or more than 10 secure e-mails with patients. All data on e-mail volumes and provider response rates and times were obtained from data extracts from the KP HealthConnect Clarity database.
Results
Between January and June 2012, patients and PCP teams collectively initiated 3.6 million secure e-mail encounters. Patients initiated 1.4 million (39%) e-mail encounters; an earlier study demonstrated that the content of patient messages was clinically relevant and required a provider clinical assessment or decision in 63% of instances (Serrato et al., 2007). Primary care provider teams initiated the balance of 2.2 million encounters (61%). Each messaging encounter contained an average of 2.0 secure messages; however, some encounters included only an initial message. Of all messaging encounters, 2.1 million included at least 1 response; these threads contained an average of 2.7 messages. In addition, Kaiser Permanente sent 2.4 million system-generated secure e-mails, such as test results and reminders about appointments or needed care.
Primary care provider teams received a daily average of 4.8 secure e-mails from patients and sent an average of 5.6 e-mail messages. We ranked PCP teams by the daily volume of secure e-mail received from patients. The top quartile consisted of 1024 (32%) PCP teams that received and sent a daily average of 9.0 and 8.5 messages, respectively. A very small group of 17 “super users” (0.5% of all PCP teams) received and sent a daily average of 13.1 and 17.3 messages, respectively; in contrast, 572 PCP teams (18%) had a daily average of zero secure e-mails to and from patients. The Figure depicts the pattern of e-mail use across PCPs in 1 representative region.
Figure.
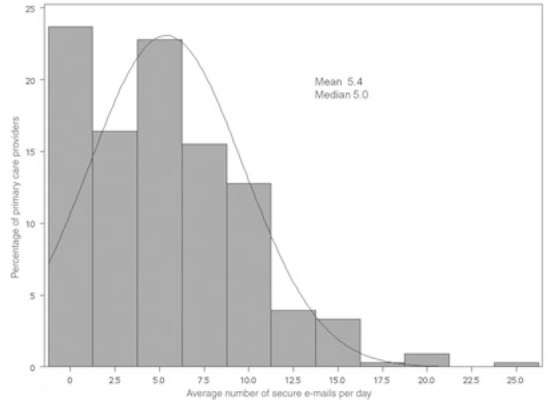
Frequency of secure e-mail with patients among Kaiser Permanente Colorado primary care providers.
Secure e-mail volumes varied slightly by specialty. Primary care provider teams in internal medicine and family practice received a higher daily average volume of e-mail from patients (6.2 and 5.5 messages, respectively) than they sent (3.8 and 3.4, respectively). In contrast, the daily average volume of messages sent by PCPs in pediatrics (1.4) and obstetrics/gynecology (2.8) was higher than the daily average volume of messages they received (1.2 and 2.4, respectively).
Of approximately 1.4 million patient-initiated secure e-mail encounters, PCP teams responded to 1.1 million (77.2%) within 2 business days. Patients received a first response in an average of 5.3 business hours, and providers sent a daily average of 2.7 responses to patient-initiated secure e-mail. Among PCP teams, the average time to first response to patient-initiated e-mail was negatively correlated with total 6-month e-mail volumes (Pearson r = −0.09, P = .0001). Among physicians only, the average response time to secure e-mail was not correlated with total 6-month e-mail volumes with patients (Pearson r = −0.04, P = .24).
Interpretation
The average volume of secure e-mail received from patients was approximately 5 per day. Physician e-mail volumes were not correlated to their response times; 1 interpretation is that fast physician response times do not encourage more messages from patients. Given that physicians spend an average of 2.5 to 3.5 minutes responding to a single secure e-mail from a patient, the average daily impact of secure e-mailing with patients on physician workloads is estimated at 15 minutes (Zhou et al., 2010). However, some secure e-mails with patients may replace phone calls, rendering this estimate generous. The few reports that exist of the effect of secure e-mail with patients on physician workloads largely confirm that impacts are neutral (Crotty et al., 2013; Keplinger et al., 2013). Physician fears about being overwhelmed with workload increases are not realized (Kittler et al., 2004), although we distinguish here between the workload associated with managing the EHR messaging in-basket tasks (results, refills, cosigns, telephone messages, etc) and the workload specific to exchanging secure e-mail with patients. Of course, even the addition of 15 minutes to an already burdened practice may feel overwhelming, and physicians with very high secure e-mail use with patients experience proportionately greater workload impacts and may be the source of a perception among physicians that patient e-mail disproportionately increases in-basket workload.
One report concludes that physicians experience longer workdays when they use secure e-mail with patients and suggests implementing team-based care to ameliorate this effect (Bishop et al., 2013). When our analysis included physicians and other providers on the team, response times to secure e-mail were negatively correlated with e-mail volumes. One possible explanation is that, as the number of e-mails increased, teams developed workflows to increase their efficiency at responding. Finally, although secure e-mails require some physician time, it is unclear whether secure e-mailing with patients replaces some office visits.
EFFECT OF SECURE E-MAIL USE ON UTILIZATION OF HEALTH CARE SERVICES
Observational studies from Kaiser Permanente exploring the association between patient portal use and utilization of health care services show mixed results.
An early assessment
In 2007, Kaiser Permanente Northwest data from some of the first members registered for the patient portal and 2 types of cohort designs assessed relationships between secure e-mailing and utilization of primary care office visits and telephone contacts (Zhou et al., 2007). A retrospective pre-post cohort design assessed the impact on utilization before and after portal registration among 4700 members who were registered portal users for longer than 13 months and had used at least 1 feature. A matched-cohort design controlled for age, gender, selected chronic conditions, and PCP while assessing differences in utilization before and after registration for 3200 members and an equal number of matched controls.
Results
In the pre-post cohort, the annual adult primary care office visit rates decreased by 0.23 (9.7%) visits per member (P < .001). In the matched cohorts, annual adult primary care office visit rates for portal users decreased by 0.25 (P < .001; 10.3%); the corresponding decrease for matched controls was 0.07 (P < .003; 3.6%). The 0.18 (6.7%) difference was statistically significant (P < .003).
Overall telephone contact rates in the region increased by 24% during the retrospective observation period, so the analysis of portal use and telephone contacts was restricted to the matched cohorts. Annual documented telephone contact rates for portal users increased by 0.32 (16.2%) contacts per member (P < .001); the corresponding rate for matched controls increased by 0.52 (P < .001; 29.9%). The 0.30 (13.7%) difference was statistically significant (P < .01).
Interpretation
Although the study did not examine specific portal uses, corroborating evidence suggested that secure e-mailing replaced some office visits and telephone encounters. For example, among portal-registered members who were surveyed, 25% and 44%, respectively, indicated that e-mailing or calling the office for advice was their chosen alternative to scheduling a visit (Zhou et al., 2007). Differential changes in utilization—either greater decreases in primary care office visit rates or constrained increases in telephone contacts—among members who used the patient portal suggested that secure e-mailing did, in fact, replace other modalities of care.
A more recent study
However, a 2012 study using matching methods documents the opposite relationship: use of the patient portal was associated with more use of clinical services, including hospital stays (Palen et al., 2012). More than 44 000 portal-using members in Kaiser Permanente Colorado were matched to an equivalent number of nonusing members using propensity score methods. Independent variables in the matching model included age, gender, race/ethnicity, number of chronic illness, and number of baseline office visits. Utilization rates for office visits, telephone encounters, after-hours clinic visits, emergency department (ED) encounters, and hospitalization were compared before and after the date of portal registration (or, in the case of controls, the median date of each member's length of enrollment) between members who did and did not use the patient portal. General estimating equation modeling was also used to compare visit rate ratios over time across matched cohorts and subgroups on the basis of age and 4 disease categories.
Results
When comparing the use of clinical services before and after the index date with that of nonusers, significant increases occurred among portal users in annual per-member rates of office visits (0.7; 95% CI, 0.6-0.7; P < .001) and telephone encounters per year (0.3; 95% CI, 0.2-0.3; P < .001). For portal users, significant increases also occurred in per 1000-member rates of after-hours clinic visits (18.7 per 1000 members per year; 95% CI, 12.8-24.3; P < .001), ED encounters (11.2 per 1000 members per year; 95% CI, 2.6-19.7; P = .01), and hospitalizations (19.9 per 1000 members per year; 95% CI, 14.6-25.3; P < .001). Comparable increases occurred across age categories. General estimating equation modeling revealed similar results. When compared with their preportal access use, the rate ratio for portal users was 1.16 (95% CI, 1.15-1.18; P < .001) for office visits, 1.08 (95% CI, 1.07-1.09; P < .001) for telephone encounters, 1.13 (95% CI, 1.08-1.18; P < .001) for after-hours clinic visits, 1.07 (95% CI, 1.02-1.11; P < .001) for ED visits, and 1.38 (95% CI, 1.30-1.47; P < .001) for hospitalizations. In contrast, nonusers had rate ratios of 1.00 or less for utilization before and after the index date for office visits, ED encounters, and hospitalizations. All differences in rate ratios between portal users and nonusers were statistically significant at P ≤ .01).
Interpretation
The reasons underlying the association of online access to care and increased use of in-person services are unclear. Members may have activated their portal access in anticipation of health needs. Members who are already more likely to use services may selectively sign up for portal access and use it to gain even more frequent access, instead of viewing it as a substitute for in-person contact with the health care system.
DIRECTIONS FOR FUTURE INQUIRY
The 2 studies exploring relationships between the use of the patient portal and other forms of health care utilization provide conflicting results. However, they share a common characteristic that is not representative of the current use of secure e-mail between providers and patients at Kaiser Permanente. Both studies assessed associations between health care utilization and the first 12 months of patient portal use. Although both excluded a 1- or 2-month interval centered on the portal registration date to minimize the effect of a known spike in office visits around the time of registration, both studies compared baseline and postregistration utilization rates among new portal users.
In contrast, secure patient-physician e-mail is a sustained, growing, and evolving care modality. In 2005, the first year for which data were collected for both utilization studies, the region with the highest use of the patient portal had registered just 6% of members. Current registration rates for adults range from 32% to 65% across regions; the current national rate is 52%. A new approach is required to understand associations between secure patient-physician e-mail and utilization of other health care services in a population with widespread and mature use of secure e-mail; designs focusing on new patient portal registrants in this more saturated environment may introduce bias. In addition, we need to examine relationships between patient portal access, secure e-mail use, utilization of clinical services, and type of health plan product purchased.
Consequently, new investigations are in process at Kaiser Permanente. They include instrumental variable analyses to account for bias arising from patient factors and examine associations between the use of secure e-mail and health care services utilization for specific clinical conditions and care processes. For instance, ongoing investigations examine associations between patient-physician secure e-mail and office visit use among members with a subset of low-acuity conditions, between secure e-mail and primary care office visits following referral to specialty care, and between secure e-mail and office visits following hospital discharge. These investigations aim to help unravel what appear to be increasingly complex associations between secure patient-physician e-mail and the use of other health care services.
CONCLUSION
Kaiser Permanente has documented benefits of secure patient-physician e-mail in terms of quality of care and member retention. Data suggest that the average impact on physician workloads is manageable, although some physicians may experience more acute challenges because of very high secure e-mail volumes, primary care practices that have not been optimized to support secure e-mail with patients, or EHR limitations that are not directly related to secure e-mail with patients. Future research is needed to isolate the effect of secure e-mailing on physician workloads. Unresolved questions remain about associations between the use of secure patient-physician e-mail and utilization of other types of health care services. Ongoing investigations seek to shed light in this area.
Footnotes
All authors declare no financial conflicts of interest.
REFERENCES
- Bishop T. F., Press M. J., Mendelsohn J. L., Casalino L. P. (2013). Electronic communication improves access, but barriers to its widespread adoption remain. Health Affairs, 32(8), 1361–1367 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Medicare & Medicaid Services. (2012). Stage 2 overview tipsheet. Retrieved from http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2Overview_Tipsheet.pdf
- Crotty B. H., Mostaghimi A., Landon B. E. (2013). Preparing residents for future practice: report of a curriculum for electronic patient-doctor communication. Postgraduate Medical Journal, 89(1056), 554–559 [DOI] [PubMed] [Google Scholar]
- Dentzer S. (2013). Rx for the ‘blockbuster drug' of patient engagement. Health Affairs, 32(2), 202. [DOI] [PubMed] [Google Scholar]
- Duru O. K., Schmittdiel J. A., Dyer W. T., Parker M. M., Uratsu C. S., Chan J., Karter A. J. (2010). Mail-order pharmacy use and adherence to diabetes-related medications. The American Journal of Managed Care, 16(1), 33–40 [PMC free article] [PubMed] [Google Scholar]
- Fricton J. R., Davies D. (2008). Personal health records to improve health information exchange and patient safety. In: Henriksen K., Battles J. B., Keyes M. A., Grady M. L. (Eds.), Advances in patient safety: New directions and alternative approaches. Vol. 4. Technology and medication safety. Rockville, MD: Agency for Healthcare Research and Quality; [PubMed] [Google Scholar]
- Keplinger L. E., Koopman R. J., Mehr D. R., Kruse R. L., Wakefield D. S., Wakefield B. J., Canfield S. M. (2013). Patient portal implementation: resident and attending physician attitudes. Family Medicine, 45(5), 335–340 [PMC free article] [PubMed] [Google Scholar]
- Kittler A. F., Carlson G. L., Harris C., Lippincott M., Pizziferri L., Volk L. A., Bates D. W. (2004). Primary care physician attitudes towards using a secure web-based portal designed to facilitate electronic communication with patients. Informatics in Primary Care, 12(3), 129–138 [DOI] [PubMed] [Google Scholar]
- Palen T. E., Ross C., Powers J. D., Xu S. (2012). Association of online patient access to clinicians and medical records with use of clinical services. JAMA, 308(19), 2012–2019 [DOI] [PubMed] [Google Scholar]
- Patel V. N., Dhopeshwarkar R. V., Edwards A., Barron Y., Sparenborg J., Kaushal R. (2012). Consumer support for health information exchange and personal health records: a regional health information organization survey. Journal of Medical Systems, 36(3), 1043–1052 [DOI] [PubMed] [Google Scholar]
- Sarkar U., Lyles C. R., Parker M. M., Allen J., Nguyen R., Moffet H. H., Karter A. J. (2014). Use of the refill function through an online patient portal is associated with improved adherence to statins in an integrated health system. Medical Care, 52(3):194–201 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schickedanz A., Huang D., Lopez A., Cheung E., Lyles C. R., Bodenheimer T., Sarkar U. (2013). Access, interest, and attitudes toward electronic communication for health care among patients in the medical safety net. Journal of General Internal Medicine, 28(7), 914–920 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seidman J., Eytan T. (2008). Helping patients plug in: lessons in the adoption of online consumer tools. Oakland, CA: California Healthcare Foundation [Google Scholar]
- Serrato C. A., Retecki S., Schmidt D. E. (2007). MyChart—a new mode of care delivery: 2005 personal health link research report. The Permanente Journal, 11(2), 14–20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tagalicod R. (2013). Stage 2: engaging patients in their health care. Retrieved from http://www.cms.gov/eHealth/ListServ_Stage2_EngagingPatients.html
- Turley M., Garrido T., Lowenthal A., Zhou Y. Y. (2012). Association between personal health record enrollment and patient loyalty. The American Journal of Managed Care, 18(7), e248–e253 [PubMed] [Google Scholar]
- Wen K. Y., Kreps G., Zhu F., Miller S. (2010). Consumers' perceptions about and use of the internet for personal health records and health information exchange: analysis of the 2007 Health Information National Trends Survey. Journal of Medical Internet Research, 12(4), e73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhou Y. Y., Garrido T., Chin H. L., Wiesenthal A. M., Liang L. L. (2007). Patient access to an electronic health record with secure messaging: impact on primary care utilization. American Journal of Managed Care, 13(7), 418–424 [PubMed] [Google Scholar]
- Zhou Y. Y., Kanter M. H., Wang J. J., Garrido T. (2010). Improved quality at Kaiser Permanente through e-mail between physicians and patients. Health Affairs, 29(7), 1370–1375 [DOI] [PubMed] [Google Scholar]