

Abstract
We report a case of an 86-year-old female patient who presented with a septic, right ureteric obstruction, caused by a symptomatic Bochdalek hernia. The patient was initially managed with percutaneous nephrostomy and final treatment was achieved by placement of an external-internal nephroureteral double pigtail.
Background
We describe a case of right-sided Bochdalek hernia complicated with ureteric obstruction, treated by means of percutaneous nephrostomy and double-J-stent placement. We think it is an interesting case presenting an alternative minimal invasive treatment method for elderly patients not suitable for surgery.
Case presentation
An 86-year-old female patient presented to the emergency department with severe right flank pain and dehydration.
Initial laboratory workup revealed an elevated white cell count at 11.5×109/L (normal 4.00–11.0×109/L) and elevated creatinine levels counting 220 µmol/L with an estimated glomerular filtration rate of 25 mL/min. The urinalysis was pathological and urine culture was positive for Escherichia coli.
Ultrasound assessment showed right-sided hydronephrosis without evidence of the obstructing cause. Non-contrast CT was performed, which confirmed right kidney acalculous hydronephrosis, in combination with a right posterior paravertebral Bochdalek hernia and large right pleural effusion. On closer examination, there was the impression of right ureter incarceration and dilation with kinking inside the hernia. No evidence of ureter dilation was noted distally (figure 1A, B).
Figure 1.

CT of the abdomen in axial slices (A) and coronal reconstruction (B) demonstrated a small right-sided posterior paravertebral Bochdalek hernia containing a loop of a dilated right ureter (arrow) resulting in mild hydronephrosis of the associated kidney Severe scoliosis of the upper lumbar spine was also noticed as well as a large right pleural effusion (not seen on these images).
The patient received medical treatment with antibiotics, analgesics and hydration and was discharged in good clinical condition 4 days later.
The patient was readmitted 48 h later with right flank pain.
Cystoscopy for double pigtail placement in the right ureter was unsuccessful, owing to the extended length of the right ureter, which was retracted inside the hernia. During the following 3 days, the patient became septic, so percutaneous nephrostomy was performed. Urine full of pus was drained, while nephrostomography confirmed the diagnosis of a cranially retracted right renal pelvis and ureter, with subsequent obstruction, prior to a major kinking inside the paravertebral hernia (figure 2). The ureter was opacified without dilation in his retroperitoneal course until the cysto-ureteral junction. The patient was discharged 3 days later and had an uneventful recovery. After 1 month, nephrostomy was successfully exchanged for an eight French nephrostomy catheter with a double pigtail ureteral extension of 26 cm length between the two pigtails (Boston Sc., Natick, Massachusetts, USA; figure 3A). The external catheter has been kept closed and internal urine drainage has been functioning without problems for a follow-up period of 3 months. After insertion of the J-stent catheter, a mild straightening of the proximal ureter was noticed on a plain abdominal film (figure 3B).
Figure 2.

Percutaneous nephrostomography confirmed the diagnosis of a cranially retracted right renal pelvis and ureter, with subsequent obstruction, owing to a major kinking inside the paravertebral hernia.
Figure 3.
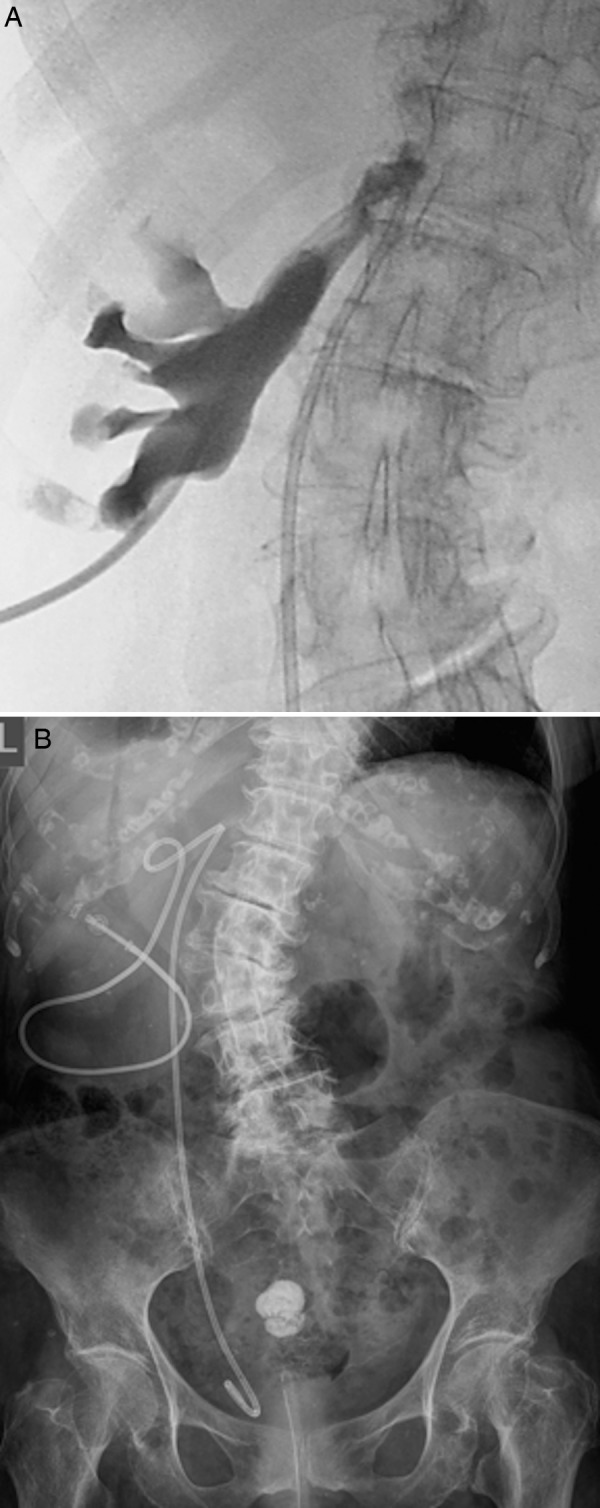
Nephrostomy was exchanged for a nephrostomy catheter with a double pigtail ureteral extension of 26 cm length between the two pigtails (A). Mild straightening of the proximal ureter was noticed on a plain abdominal film (B). A small calcified uterus fibroma was also noticed.
Discussion
Bochdalek hernias result from a developmental failure of postero-lateral diaphragmatic foramina to fuse properly.1 They are the most common type of congenital diaphragmatic hernia, accounting for 95% of cases.2 In adults, most Bochdalek hernias are rare, usually asymptomatic, and therefore their detection is incidental.2–4 Their estimated prevalence ranges from 0.17% to 12.7% according to more recent studies with the use of MDCT and multiplanar reconstruction.2 5 Rarely, incarceration of the ureter in a BH with subsequent obstructive uropathy is possible and has been reported.6–8
Congenital diaphragmatic hernia was first described by Vincent Alexander Bochdalek in 1848.9 It results from the incomplete closure between the lumbar and costal part of the left or right diaphragm during fetal development.1 Symptomatic presentation of Bochdalek hernias in adulthood is usually rare and therefore their detection is incidental.2–4 Most commonly, symptoms are caused by a left-sided hernia in about 90% of all cases.10 Presenting symptomatology depends on the incarcerated anatomic structure, including the kidneys, stomach, bowel, liver, spleen or omentum, and may vary greatly, including chest pain, dyspnoea, nausea, vomiting or severe flank pain.11 12 Entrapment of the renal pelvis and proximal ureter is extremely rare with only four cases reported in the literature.7 8 11 13 Of these, one was asymptomatic and was discovered incidentally,13 one presented with right upper quadrant pain,7 another presented with a 12-month history of intermittent flank pain8 and one presented with severe flank pain and a background of 12 months intermittent flank pain.11 Our patient was otherwise asymptomatic until she presented with acute right flank pain, acute on chronic renal failure and leukocytosis. To date, there have been no reports for a BH associated with ureteral obstruction and complicated with severe septic pyelonephritis.
Plain films and ultrasound examination can be of limited diagnostic help in such cases. A non-contrast CT scan is the modality of choice in order to demonstrate anatomic detail and associations of neighbouring structures and to also exclude calcified stones in the course of a dilated ureter. In this case, findings of BH with entrapment of the ureter, which maintains a normal calibre peripherally, can lead to the diagnosis.10 14
Treatment can be definitive by means of surgical or laparoscopic hernia repair, but diaphragmatic surgery is not without complications, and elderly patients in particular gain only a minimal benefit as the risk of further herniation over their remaining lifetime is low. Under this scope, surgery should be the last option for elderly and/or debilitated patients; however, it should be suggested for younger patients with long life expectancy.12 15
Rigid cystoscopy with placement of a double pigtail ureteral catheter is perhaps the less invasive treatment method.7 11 We attempted this approach but failed due to the lengthy distance between the cysto-ureteral junction and the renal pelvis. In fact, the pigtail remained beneath the hernia level and had to be retrieved. Our patient was subsequently managed with placement of a percutaneous nephrostomy, which decompressed the septic right urinary system, confirmed the diagnosis and allowed us to proceed with a second step internal drainage placement after the patient recovered. Placement of a closed external and internally draining double pigtail catheter allows us an easy exchange procedure at 6-month intervals avoiding new unpleasant cystoscopies for the patient. Additionally, since placement of the flexible 8 Fr catheter, a mild correction of the ureter course has been noted.
Learning points.
From this case one can learn how diagnostic imaging can lead us to the correct assessment of the underlying pathology.
One can also learn how to use this minimal invasive option for elderly patients who are not suitable for surgery.
Percutaneous nephrostomy combined with nephro-ureteric catheter placement offers an alternative palliative treatment method.
Footnotes
Contributors: AH practised all interventional procedures; AK wrote the manuscript; DG was the doctor responsible for the patient; CM edited the manuscript.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Sandstrom CK, Stern EJ. Diaphragmatic hernias: a spectrum of radiographic appearances. Curr Probl Diagn Radiol 2011;40:95–115 [DOI] [PubMed] [Google Scholar]
- 2.Temizöz O, Gençhellaç H, Yekeler E, et al. Prevalence and MDCT characteristics of asymptomatic Bochdalek hernia in adult population. Diagn Interv Radiol 2010;16:52–5 [DOI] [PubMed] [Google Scholar]
- 3.Rout S, Foo FJ, Hayden JD, et al. Right-sided Bochdalek hernia obstructing in an adult: case report and review of the literature. Hernia 2007;11:359–62 [DOI] [PubMed] [Google Scholar]
- 4.Agrafiotis AC, Kotzampassakis N, Boudaka W. Complicated right-sided Bochdalek hernia in an adult. Acta Chir Belg 2011;111:171–3 [DOI] [PubMed] [Google Scholar]
- 5.Mullins ME, Stein J, Saini SS, et al. Prevalence of incidental Bochdalek's hernia in a large adult population. AJR Am J Roentgenol 2001;177:363–6 [DOI] [PubMed] [Google Scholar]
- 6.Osman N, Venugopal S, Doyle G, et al. Bochdalek's hernia causing functional upper ureteric obstruction. Br J Med Surg Urology 2012;5:90–2 [Google Scholar]
- 7.Song YS, Hassani C, Nardi PM. Bochdalek hernia with obstructive uropathy. Urology 2011;77:1338. [DOI] [PubMed] [Google Scholar]
- 8.Paterson IS, Lupton EW. Pelviureteric junction obstruction secondary to renal pelvic incarceration in a congenital diaphragmatic hernia. Br J Urol 1989;64:548–9 [DOI] [PubMed] [Google Scholar]
- 9.Haller JA, Jr. Professor Bochdalek and his hernia: then and now. Prog Pediatr Surg 1986;20:252–5 [DOI] [PubMed] [Google Scholar]
- 10.Wilbur AC, Gorodetsky A, Hibbeln JF. Imaging findings of adult Bochdalek hernias. Clin Imaging 1994;18:224–9 [DOI] [PubMed] [Google Scholar]
- 11.Balakrishnan V, Neerhut G. Right sided Bochdalek hernia causing ureteric obstruction. BJU Int http://www.bjui.co.uk/ContentFullItem.aspx?id=769&SectionType=1&title=Right-sided-Bochdalek-hernia-causing-ureteric-obstruction [Google Scholar]
- 12.Brown SR, Horton JD, Trivette E, et al. Bochdalek hernia in the adult: demographics, presentation, and surgical management. Hernia 2011;15:23–30 [DOI] [PubMed] [Google Scholar]
- 13.Chawla K, Mond DJ. Progressive Bochdalek hernia with unusual ureteral herniation. Comput Med Imaging Graph 1994;18:53–8 [DOI] [PubMed] [Google Scholar]
- 14.Shin MS, Mulligan SA, Baxley WA, et al. Bochdalek hernia of diaphragm in the adult. Diagnosis by computed tomography. Chest 1987;92:1098–101 [DOI] [PubMed] [Google Scholar]
- 15.Palanivelu C, Rangarajan M, Rajapandian S, et al. Laparoscopic repair of adult diaphragmatic hernias and eventration with primary sutured closure and prosthetic reinforcement: a retrospective study. Surg Endosc 2009;23:978–85 [DOI] [PubMed] [Google Scholar]