

Abstract
A 46-year-old woman presented with right upper abdominal pain and fever. At imaging, enlarged peripancreatic and hilar lymph nodes, as well as hypodense liver lesions, were detected, suggestive of malignant disease. At endoscopy, the mass adjacent to the duodenum was seen as a protruding lesion through the duodenal wall. A biopsy of this lesion, taken through the duodenal wall, showed a histiocytic granulomatous inflammation with necrosis. Serology for Bartonella henselae IgM was highly elevated a few weeks after presentation, consistent with the diagnosis of cat scratch disease. Clinical symptoms subsided spontaneously and, after treatment with azithromycin, the lymphatic masses, liver lesions and duodenal ulceration disappeared completely.
Background
This is the first case report describing ‘cat scratch’ disease with severe radiological abnormalities and a protruding mass in the duodenum. The patient only recalls a dog bite and no known cat scratch, although she does own cats. After the dog bite she did develop a skin lesion, which resembled erythema nodosum according to her general practitioner. Therefore, the dog bite might have been the cause of the infection with Bartonella henselae. This micro-organism caused liver lesions, and pancreatic and duodenal lymphadenitis, with a protruding lesion into the duodenal wall, without any signs of perforation. To the best of our knowledge, no such protruding lesion, as seen at endoscopy in the duodenum, has ever been described.
Clinicians should also bare in mind that B. henselae IgM antibodies may be elevated up to 3 months after the initial infection. Therefore, as in our case, repetitive testing is necessary to obtain the diagnosis. Our patient was successfully treated with azithromycin.
Case presentation
A 46-year-old woman presented with right upper abdominal pain and fever which had lasted a week. When seen at the outpatient clinic she no longer had fever; there was no jaundice, weight loss, incidental night sweats or stomach-related problems. There was no history of a visit to the tropics. She was diagnosed in the past with high cholesterol and used Lipitor for years. Her family history revealed no malignancies. Physical examination showed no abnormalities and no signs of valvular cardiac disease were found. There were no skin defects or peripheral lymphadenopathy at the time of presentation.1
Investigations
Imaging: on ultrasound, large confluent nodules were seen at the area around the pancreas head as well as at the hepatoduodenal ligament, highly suggestive of enlarged lymph nodes. No conspicuous lesion was seen in the pancreatic head. Additional imaging was conducted by means of a CT scan. This confirmed the presence of the enlarged lymph nodes adjacent to the duodenum (figure 1). Furthermore, two hypodense lesions were seen in the liver.2 3 Owing to the severity and the radiological aspect of the liver lesions a differential diagnosis of metastases of an unknown primary tumour, multifocal hepatocellular carcinoma and cholangiocarcinoma was made.
Figure 1.

CT scan showing enlarged lymph nodes adjacent to the duodenum.
An upper endoscopy was performed showing a small protruding lesion in the descending duodenum. When a set of biopsy forceps was introduced to take a sample, it could easily be passed through the duodenal wall into the area where the lymphatic mass was suspected (figure 2). At the time the patient was completely without symptoms and had no signs of perforation; the adjacent mass must have sealed off this area, as was already visible on CT scan, which also showed a lack of free air. Histology of the biopsies taken through the duodenal wall showed no dysplasia but did reveal a histiocytic granulomatous inflammation with necrosis (figures 3 and 4). All tumour markers were negative. A systemic or infectious disease was now more likely. No micro-organisms, such as bacteria, fungi or mycobacteria could be detected in the histology specimens using specific stains including Ziehl-Neelsen and silver staining. Serum interferon-γ release assays (IGRA) and PCR on tissue for tuberculosis, and serological tests for Epstein-Barr virus and Cytomegalovirus were all negative. HIV and Borrelia serology were negative. Serology for B. henselae obtained 6 weeks after the initial presentation showed a positive ELISA IgM: 5.89 and IgG: 3.57 ratio (optical density=OD 450 nm/690 nm; IgM in house ELISA, RIVM the Netherlands).4 In retrospect a serum specimen taken 3 weeks earlier showed an IgM: 2.55. As IgM is typically only found in the first 3 months after infection and a significant rise in IgM titre was seen, infection from this organism was confirmed. PCR testing for B. henselae in an earlier specimen, which contained purulent material, of the duodenal mass was negative for B. henselae DNA. No genotype could be determined.
Figure 2.

Endoscopic image of a protruding lesion in the duodenum. Biopsy forceps could easily pass through the duodenum wall.
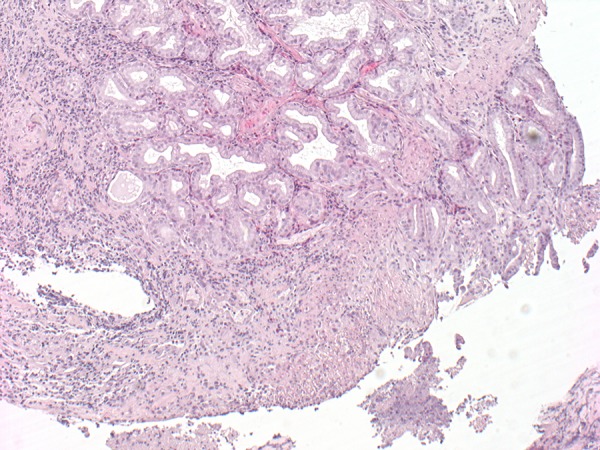
Figure 3.
Duodenal biopsy showing a mucosal defect and histiocytic inflammation.
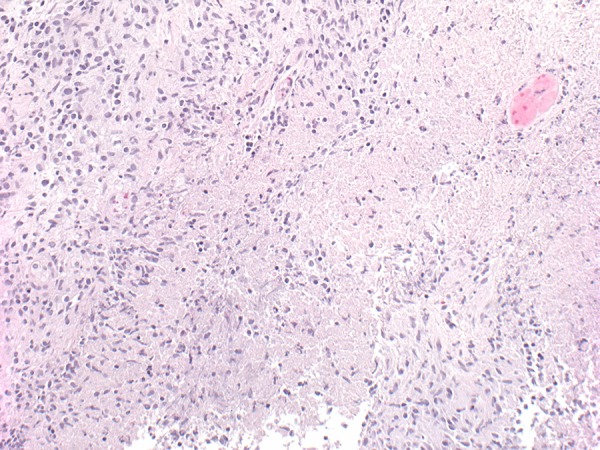
Figure 4.
Submucosal duodenal tissue with palisading histiocytes at the rim of a necrotic area.
Treatment
Owing to the severity of the abnormalities found at endoscopy and radiology images the patient was treated with azithromycin 500 mg 1 day, followed by 4 days with 250 mg once daily, even though she had no further symptoms.
Outcome and follow-up
Four months after the initial presentation a control ultrasound was performed showing a normal aspect of the liver, the enlarged lymph nodes had completely subsided. Also, a repeat upper endoscopy was performed showing a healed duodenal wall. The patient was completely without symptoms and doing well.
On further questioning, the patient mentioned she has two cats, but she did not recall any bites or scratches.5 However, she did recall being bitten by a young dog after which she developed a lesion on her leg, which had the appearance of erythema nodosum, according to her general practitioner, 2 weeks before her symptoms started. Neither the dog nor her cats were tested for B. henselae.
Discussion
This is the first case report describing ‘cat scratch’ disease with a protruding mass in the duodenum in addition to other upper abdominal radiological abnormalities, perhaps caused by a dog bite. In most presentations, lymphadenopathy depends on the site of the primary inoculation. The most common locations are the axillary, epitrochlear, cervical, supraclavicular and submandibular lymph nodes. Our patient experienced a dog bite and no known cat scratch, although she did own two cats. Interestingly, after the dog bite she did develop a skin lesion, which resembled erythema nodosum, on her leg, according to her general practitioner. Therefore the dog bite might well have been the source of the infection with B. henselae causing all her symptoms. The protruding lesion into the duodenal wall was a remarkable endoscopic finding, without any clinical signs of perforation. We were not able to identify existing references describing such protruding lesions. We were fortunate to have consecutive specimens that enabled us to show a serological IgM titre rise, which is more convincing evidence of infection compared with a single specimen. The patient was treated with azithromycin, although spontaneous healing was already suggested by the clinical course.
Patient's perspective.
The patient first experienced anxiety due to the fact that a malignancy was suspected. When the diagnosis of cat scratch disease was made, it was a big relief for herself and her family.
Learning points.
Cat scratch disease can appear as hypodense liver lesions and lymphadenitis protruding into the duodenal wall, mimicking malignant disease; a dog bite (or flea or tick bite) may have caused it in our patient.
Bartonella henselae serology shows a positive dynamic; IgM antibodies may be elevated up to 3 months after the initial infection.
Fortunately, ugly masses can also be due to benign causes.
Footnotes
Contributors: MvI-vL wrote the case report. JP revised the manuscript and added the CT scan picture. HB revised the manuscript and added two histology pictures.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Weinspach S, Tenenbaum T, Schönberger S, et al. Cat scratch disease—heterogeneous in clinical presentation: five unusual cases of an infection caused by Bartonella henselae. Klin Padiatr 2010;222:73–8 [DOI] [PubMed] [Google Scholar]
- 2.Dzelalija B, Petrovec M, Avsic-Zupanc T. Probable atypical cat scratch disease presenting as isolated posterior pancreatic duodenal lymphadenitis and abdominal pain. Clin Infect Dis 2001;33:912–14 [DOI] [PubMed] [Google Scholar]
- 3.Anyfantakis D, Kastanakis M, Papadomichelakis A, et al. Cat-scratch disease presenting as a solitary splenic abscess in an immunocompetent adult: case report and literature review. Infez Med 2013;21:130–3 [PubMed] [Google Scholar]
- 4.Herremans M, Bakker J, Vermeulen M, et al. Evaluation of an in-house cat scratch disease IgM ELISA to detect Bartonella henselae in a routine laboratory setting. Eur J Clin Microbiol Infect Dis 2009;28:147–52 [DOI] [PubMed] [Google Scholar]
- 5.Jeffrey D, Kravetz MD, Daniel G, et al. Cat-associated Zoonoses. Arch Intern Med 2002;162:1945–52 [DOI] [PubMed] [Google Scholar]