

Abstract
The prevalence of Type 2 diabetes (DM2) is rapidly rising, especially among minority and low-income youth. There is an unmet need to engage youth in identifying solutions to reverse this trajectory. Social marketing campaigns and entertainment education are effective forms of health communication for engaging populations in health-promoting behaviors. Critical to curbing the epidemic is moving the diabetes conversation away from individual behavior alone and toward a socio-ecologic perspective using a public health literacy framework. We developed an academic-community partnership to develop, implement, and evaluate a DM2 prevention campaign targeting minority and low-income youth. The Bigger Picture uses hard-hitting, youth-generated “spoken-word” messages around key environmental and social drivers of the DM2 epidemic. Campaign goals included promoting health capacity and civic engagement. This paper focuses on the development and implementation of the campaign, including (a) rationale and theoretical underpinnings; (b) steps in campaign creation; (c) testing the campaign messaging; and (d) campaign dissemination and evaluation planning. A youth-created health communication campaign using a public health literacy framework with targeted, relevant, and compelling messaging appears to be a promising vehicle for reaching at-risk youth to increase knowledge of and attitudes about preventing DM2, change social norms, and motivate participation in health promotion initiatives.
In the U.S., type 2 diabetes (DM2) prevalence is increasing dramatically, especially among minority youth and young adults. With this rise are growing disparities related to race/ethnicity and socioeconomic status (Mayer-Davis et al., 2009). The Centers for Disease Control and Prevention has estimated that the lifetime risk of developing type 2 diabetes for those born in 2000 is highest for Hispanics (53% and 45% for females and males, respectively) followed by Blacks (49% and 40%, respectively), and finally whites (31% and 27%, respectively) (Narayan, Boyle, Thompson, Sorensen, & Williamson, 2003). A recent study of youth ages 12–19 revealed that 23% had pre-diabetes or type 2 diabetes, up from 9% only 8 years prior (May, Kuklina, & Yoon, 2012). Another analysis of the same ages demonstrated 34% of DM2 cases to be previously undiagnosed (Demmer, Zuk, Rosenbaum, & Desvarieux, 2013).
Diabetes interventions focused on individuals may be inadequate to reverse these epidemic trends. While a number of studies test DM2 prevention interventions focused at the individual level (HEALTHY Study Group et al., 2009; Hofsteenge, Chinapaw, Weijs, van Tulder, & Delemarre-van de Waal, 2008; Lindstrom, Absetz, Hemio, Peltomaki, & Peltonen, 2010; Ritenbaugh et al., 2003; Siegrist, Hanssen, Lammel, Haller, & Halle, 2011; Vos, Wit, Pijl, Kruyff, & Houdijk, 2011; Wilmot et al., 2011; Zhang & Cooke, 2012), it is increasingly recognized that such approaches are costly and difficult to scale so as to achieve population impacts. A more comprehensive approach that adopts a socio-ecological perspective and includes a focus on the environment, social conditions, and root causes of diabetes-related health disparities is necessary to reverse this frightening trajectory.
Rationale and Theoretical Underpinnings
Public Health Literacy
Public health literacy is defined as “the degree to which individuals and groups can obtain, process, understand, evaluate, and act upon information needed to make public health decisions that benefit the community” (Freedman et al., 2009). It is a recent construct that takes into account the complex social, ecologic, and systemic forces affecting well-being. It consists of three dimensions – conceptual foundations, critical skills, and civic orientation (Table 1) – and together with individual-level health literacy, can forma more comprehensive model of what being “health literate” means (Freedman et al., 2009).
Table 1.
Dimensions of public health literacy applied to the creation and dissemination of The Bigger Picture campaign.
| Dimensions of Public Health Literacy | Dimensions of The Bigger Picture |
|---|---|
|
Conceptual Foundations Basic knowledge and information needed to understand and take action on public health concerns. |
Information presented in youth poet writing workshops |
| Core public health concepts such as primary prevention, health promotion, and population health | Core concepts of primary prevention of DM2, health promotion to decrease risk |
| Public health constructs (prevalence, risk factors, probability, ORs) and the relationship of each to morbidity and mortality | Social and ethnic disparities in prevalence of DM2, probabilities of disease complications, and risk factors for DM2 |
| Ecologic perspectives and the many pathways through which health is promoted | Influence of the built environment, food and beverage policy, poverty, food insecurity, and advertising practices in addition to individual behavior and genetics on DM2 risk |
|
Critical Skills Skills necessary to obtain, process, evaluate, and act upon information needed to make public health decisions that benefit the community |
Youth poets re-story the information into spoken-word PSA scripts |
| Obtain, evaluate, and utilize public health information from a variety of sources | Poets incorporated statistics, geocoded maps, infographics and fact sheets about DM2 into PSAs |
| Identify public health aspects of personal and community concerns | Poets used knowledge and experience of own communities (e.g. violence, urban planning) in talking about DM2 |
| Communicate information about health conditions and actions not only as a personal concern but also as a problem affecting the larger community | Poets interpreted the link between DM2 and policies about food, education, and health care, and the role of advertising and corporate marketing of food as affecting individuals and the larger community |
| Assess who is naming and framing public health problems and solutions, and describe framing limitations | Poets recognized the cultural, historical, and institutional boundaries on the framing of DM2 risk based on individual behavior, and re-framed it as one based in the built environment, policy, poverty, and marketing |
|
Civic Orientation Ensures that “the public” remains at the center, includes skills and resources necessary to address health concerns through civic engagement. |
Disseminate campaign to those most at risk for DM2 – low-income and minority youth – with the goal of inspiring civic engagement |
| Articulate that the burdens and benefits of society are not fairly distributed | PSAs and school presentations focus on the social determinants of DM2 |
| Evaluate who benefits and who is harmed by public health efforts or lack thereof | PSAs and school presentations demonstrate lack of policy efforts to address root causes of DM2 risk |
| Communicate that public health problems are not inevitable and can be changed through civic action | PSAs and school presentations include messages of getting involved in the community, to take action, including a list of organizational resources |
| Address public health problems through civic action, leadership, and dialogue | School presentations encourage student participation and dialogue, campaign website invites youth to tell their stories about mitigating DM2 risk |
Adapted from Freedman et al. (2009).
Deficits in public health literacy abound. Despite the scientifically accepted construct of social determinants of health, a 2008–2009 national survey revealed that Americans believed health was most affected by individual behaviors and access to health care while social or economic factors were less important, and respondents who were non-White and lower income recognized a stronger role for social determinants (Robert & Booske, 2011). Respondents were also less aware of health disparities by race than by income (Booske, Robert, & Rohan, 2011). Among a group of nationally representative U.S. adults, predisposing values toward personal responsibility and political orientation account for some differences in reactions to messages about health disparities (Gollust & Cappella, 2014). Researchers and clinician soften identify personal responsibility and behavior as the natural starting point for health discourse, assumptions that resonate with values implicit in the “American Dream” (Lundell, Niederdeppe, & Clarke, 2013).
News media propagates these views. For example, responsibility about obesity in the media through 2004 was attributed to personal causes and solutions significantly more than societal attributions (Kim & Willis, 2007). With respect to the burgeoning DM2 epidemic, a study of articles about DM2 in US newspapers in 2005–2006 found that of those proposing a strategy to address diabetes, 58% focused on individual behavior change while only 12% described any upstream, population-based strategies; of those mentioning at least one cause of DM2, 70% mentioned obesity or weight gain, 50% biology, and 40% individual behaviors, while only 12% mentioned socioeconomic or neighborhood factors (Gollust & Lantz, 2009). Responses by a diverse group of American adults to news media narratives describing social causation for DM2 were highly variable, and were strongly associated with political affiliation (Gollust, Lantz, & Ubel, 2009).
In social psychology, attribution theory suggests that people explain the causes of events or a person’s disposition as either internal or external, with the former seen as caused by a person’s characteristics which are in his or her control, and the latter seen as caused by contextual factors which are outside a person’s control (Heider, 1958). Some Americans attribute social conditions to personal flaws while others attribute them to societal factors, and this is strongly associated with support for policies addressing these factors (Iyengar, 1989). For example, adults were more likely to support government spending on research of DM2 after viewing an article on social determinants of DM2 compared to those viewing an article with no causal language (Gollust, Lantz, & Ubel, 2010). People’s attributions of responsibility for health disparities therefore shape support for policy, and more effective messaging to emphasize social determinants of health has potential to influence policy support (Niederdeppe, Bu, Borah, Kindig, & Robert, 2008). Perhaps educating minority youth, who may have the most to gain due to their increased risk for DM2, about social determinants of DM2 is a critical step toward improving public health literacy and policy support related to the DM2 epidemic.
Social Marketing and Entertainment Education
A key first step in any educational campaign is to create appealing messages. Social marketing accomplishes this by applying marketing strategies to increase the acceptability of ideas or practices in a target group and improving their spread through message promoters who resonate with the target audience. Social marketing can help translate scientific knowledge into effective education programs (Lefebvre & Flora, 1988). Similarly, entertainment education is the process of designing and implementing media messages to entertain while increasing an audience’s knowledge about an issue, creating favorable attitudes, and changing behavior (Singhal & Rogers, 1999).
Social marketing campaigns have proven effective in engaging youth around health promotion. One of the most well-studied is the U.S.-based Truth® antismoking campaign, which shifted focus from individual behavior toward a socio-environmental perspective, delivering messages about tobacco industry practices. This campaign changed attitudes, beliefs, and behavior, especially among African-American youth (Cowell et al., 2009; Davis et al., 2009; Farrelly et al., 2002; Farrelly et al., 2005; Farrelly et al., 2009). Supporting the use of a socio-environmental perspective to change behavior, high school students participating in community advocacy activities to counter environmental influences of smoking reported lower rates of regular smoking than students who simply learned about smoking and drug prevention (Winkleby et al., 2004). Shifts in social norms, in part, contributed to success in tobacco control (Klein & Dietz, 2010), and this target may be well-suited for DM2. Youth participation in content creation may also be important – a Photovoice project in which students created Public Service Announcements (PSAs) about socio-ecological contributions to asthma demonstrated increased knowledge among community members and engaged adolescents in education (Gupta et al., 2013).
From a strategic standpoint, there is particular value in focusing on youth because of their vulnerability to advertising (Kunkel et al., 2004), and counter-advertising campaigns have potential to improve awareness (Mello, Studdert, & Brennan, 2006). Since youth are heavy consumers of the internet, including a web-based component is likely critical. Digital media, through user-generated content, enables members of marginalized groups to speak for themselves and to call attention to the environmental conditions that obstruct healthy living. The internet provides an opportunity for direct communication between individuals and large audiences, serving as a potential for communication about health disparities and environmental barriers (Niederdeppe, Bigman, Gonzales, & Gollust, 2013).
We believed that a campaign merging principles of social marketing and entertainment education would be an important avenue toward engaging minority youth, and that a campaign focused on socio-environmental factors contributing to DM2 risk might improve public health literacy among minority and low-income youth and their stakeholders. Our two goals were to: (1) enable minority youth poets to create the campaign messaging while also promoting their own development including the capacity for initiative (Larson 2000, Zeldin 2004) and health literacy (Wharf Higgins 2009), and to (2) enhance engagement of an adolescent audience by virtue of the authenticity of the content and the focus on health and social justice. The aim of this paper is to describe the development and early implementation of The Bigger Picture, a youth-targeted diabetes prevention campaign that uses youth-generated “spoken-word” messages around key environmental and social prevention targets to engage, educate, and activate youth to find solutions to the complex and challenging problem of DM2.
Campaign Creation
Academic-Community Partnership
After the Director (DS) of UCSF’s Center for Vulnerable Populations (CVP) Health Communications Program (http://cvp.ucsf.edu/) heard a youth poet perform about diabetes in her family, collaboration planning began with the Executive Director (JK) of the non-profit Youth Speaks (YS) (http://youthspeaks.org/) to fill a gap in relevant youth-targeted messaging about DM2. YS is committed to youth development through spoken-word performance and literacy promotion in San Francisco, CA, and helped create sister programs in 47 cities across the U.S. The CVP and YS formed a partnership in order to develop, seek grant funding for, and disseminate a DM2 prevention campaign using spoken-word messages written and performed by youth poets to educate and activate their peers around the social and environmental conditions that affect DM2 risk. The synergy between the two groups, with CVP faculty’s public health expertise in diabetes and health communication, and YS bringing over a decade of community and youth engagement and pedagogy, laid a strong partnership foundation.
Campaign Vision
Using a public health literacy framework (Table 1), the focus of the campaign was to re-frame DM2 dialogue from individual behavior change to the social and environmental determinants that increase DM2 risk, particularly in distressed communities that lack both access to health opportunities such as fresh affordable food and safe areas for physical activity, and awareness of the institutional forces that shape consumer choices such as targeted promotion of low-cost sugar-sweetened beverages and junk food. Through a creative convergence between social marketing and entertainment education, youth spoken-word voices became the vehicle for health messaging, with the ultimate goal of engaging the youth poets, low-income and minority youth, and their community stakeholders to increase knowledge of, shift attitudes about, and build capacity to prevent DM2 in their communities.
The initial campaign target audience was low-income and minority youth and young adults living in distressed neighborhoods in the San Francisco Bay Area, the group hardest hit by the growing diabetes epidemic. Potential inroads to this audience included the public school system and community events in target neighborhoods, as well as a web-based platform. By having the messaging created and performed by youth poets, we hoped to maximize the appeal of peer influence and assure fresh and relevant content. We also hoped to contribute to the paucity of available messaging focused on the social determinants of DM2 to counterbalance the predominance of information around individual behavior’s contribution to DM2 risk. From a public health literacy perspective, our goal was to engage more stakeholders in public health efforts aimed at diminishing DM2 risk, and promote greater engagement in addressing community-level determinants of DM2, specifically, and health more broadly.
We collaboratively determined the campaign’s title, The Bigger Picture (TBP), because it encourages the viewer to “take a step back” when looking at the DM2 epidemic and “see” the larger social and environmental forces at play. To date (3 years), the partnership has secured $215,827 (nearly $72,000/year) in grant funding for campaign development, early implementation, and dissemination.
Creation of the Spoken-Word Public Service Announcements by Youth Poets
Previous groups have had success using a collaborative, “learners as interpreters” approach, in which health information is interpreted and retold as prevention messages in participants’ own communities (Handley, Santos, & McClelland, 2009), Similarly, we conducted seven writing workshops – each made up of 5–8 sessions lasting 2 hours each (16–20 hours total) – for over 40 YS poets over the course of 3 years. Poets were invited to participate in TBP by YS staff based on their level of YS experience, participation in performances or workshops, and demonstrating development as a writer and public speaker. Participating YS poets were between the ages of 16 and 24, and the majority self-identified as Latino or Black. Youth poets received a stipend of $100 for their work, consistent with standard YS poet compensation. CVP faculty (DS) and the TBP Project Director (SF) provided workshop content through power point presentations, videos, and fact sheets that displayed DM2 data at the individual and population level in dynamic and appealing ways, such as through geo-coded maps and infographics. The workshops engaged poets through interactive discussions about the growing prevalence of DM2; social and ethnic disparities in prevalence and complications of DM2; and the influence of the built environment, food and beverage policy, poverty, food insecurity and advertising practices on DM2. Workshops were facilitated by an experienced YS poet mentor. The poets had time in each workshop to “re-story” this information into first-person narratives and poems, consistent with dimensions of public health literacy (Table 1). Through an iterative group review process, poems were finalized and, to date, 17 scripts selected (typically 2–3 per workshop) to become video PSAs (2 also in Spanish making 19 total) for posting on the website.
TBP team and poets worked with a professional videographer to create well-produced video PSAs, with the poets themselves often performing as actors. PSA themes have included the association of DM2 risk with the built environment, industry marketing practices targeting minority youth, sedentary behavior, food addiction and stress, food insecurity, poverty, sugary drinks and industry tactics, and racial and socioeconomic disparities. The PSAs can be viewed at www.thebiggerpicture.org/watch/. Example PSA excerpts are displayed in Figure 1.
Figure 1.

Selected campaign public service announcement excerpts and images.
Development of the On-Line Platform
Because digital media provides an opportunity for direct communication between individuals and large audiences with potential to contribute to social movements and to shape public discussion, and because youth are heavy users of social media, the marketing director of YS built an on-line platform for the campaign. We built TBP campaign website (Figure 2, www.thebiggerpicture.org) in English and Spanish to include appealing, clear, and reliable information about diabetes; the video PSAs; links to related resources; and a downloadable toolkit and workbook for educators that could be used in classrooms to build on content expressed in the PSAs. These materials were developed from information provided by CVP and compiled by the YS team into a format congruent with their creative writing pedagogy. The CVP and YS websites also embedded links to promote the campaign website. To increase visibility by social media users and promote the campaign, we created a Facebook page (www.facebook.com/thebiggerpicturecampaign) and a Twitter account (https://twitter.com/BigPicCampaign).
Figure 2.
Screenshot of the campaign website (www.thebiggerpicture.org).
Testing the Campaign Messaging
As PSAs were being finalized and the videos produced, we did preliminary testing to assess appeal while still opportunity to make adjustments, to understand the implementation needs and challenges prior to dissemination to the target audience, and to foster engagement of those who work directly with or are members of the target population. We tested the campaign messaging through surveys both of the youth poets participating in the workshops and of Bay Area health and community stakeholders.
Youth poet surveys: refining campaign direction and understanding engagement
The youth poets who participated in writing workshops largely represented our target audience of minority youth and young adults, and were deeply involved in the translation of data about DM2 into spoken-word stories of the disease’s effect in their own communities, making their perceptions important for gauging whether the campaign was growing in the right direction. To understand their knowledge of DM2, the effect of this information on their intention to make changes in their communities and themselves, and the importance they attribute to this work as compared to other issues, we invited poets from two of the first four writing workshops to complete anonymous paper surveys on both the first and last days of the workshop. The surveys asked about relevance of DM2, whether the poet discussed DM2 with his/her peers, and whether the poet would describe DM2 risk as a medical issue or a social justice issue. They were also asked to rank the contribution of 5 factors to DM2 risk: 1. unhealthy individual behaviors, 2. genetics, 3. food policies, 4. insufficient opportunities for physical activity, and 5. social class. Each question was asked both before and after the workshop so that short-term changes could be assessed. In addition, open-ended post-workshop questions offered poets the opportunity to share what they thought would work best to reach and motivate youth, and what personal changes and social action the poets intended to pursue.
Thirteen of 14 poets completed surveys. At the end of the workshop, 10 poets reported talking with their friends about DM2, up from only 4 poets on the workshop’s first day. On a scale of 1–10 (10 = highest relevance) asking how relevant DM2 was as an issue affecting their peers and themselves, the average response was 5.1 before the workshop (range 1–8) and increased to 7.3 after, with 3 individuals ranking it a 10 (range 3–10). After the workshop, all but one of the respondents identified DM2 as a social justice issue, or as both a medical and social justice issue. Before the workshop, the most commonly ranked top contributor to DM2 risk was unhealthy individual behaviors while the least commonly ranked was insufficient opportunities for physical activity. At the end of the workshop, this rank order remained unchanged.
When answering how TBP could reach youth, the poets most often identified using Youth Speaks events and high school classrooms, developing more workshop curricula, making the information “relatable” to youth, and using the arts to “inform and have the youth critically evaluate how diabetes affects them.” In exploring how the campaign could motivate youth to care, the poets again identified writing workshops, school visits and interactive events to increase knowledge, and “give them tools” to take action and make changes both in personal choices and at a community level.
Reflecting on their own intended personal changes, most focused on individual dietary and physical activity behaviors: “drink more water,” “stop drinking soda,” and “go to more dance classes.” However, some incorporated both changes of their individual behavior as well as community-level activity: “I’m going to be more consciously aware of my environment, what it produces, and therefore what I consume,” and, “Try to perform more pieces that spread awareness about the effects of capitalism… I will support more food justice organizations and events and shop at my local farmers markets.” Finally, reflecting on their own intended social actions, the most common themes involved educating their community. “Talk to more people about diabetes,” “Tell friends to stop drinking soda,” and, “I’m going to start with buying my dad groceries… actual groceries.” Some also discussed continuing with campaign promotion: “Helping to build the school visit program,” and, “Promote The Bigger Picture and sustainable food initiatives.”
These poets had in-depth exposure to and buy-in into the themes of social and environmental contributions to DM2 risk through the workshops, and though most of them still focused on individual behaviors as their intended change, there was clear appreciation for why it was harder for some to change than others. This is perhaps evidence that these poets who were deeply involved with messaging understood that individual behavior is shaped by environment, or perhaps that our American cultural values of and common messaging around the importance of individual behavior may be difficult to shift. This underscores that DM2 is a complex disease dependent upon genetics, individual behavior, and social and environmental constructs.
Youth and community stakeholder surveys: refining messages and fostering engagement
Prior to and during early dissemination, stakeholders not only provided feedback for testing and refining the messages but were also intermediaries serving as early campaign disseminators to the youth with whom they work. We defined a relevant stakeholder group as adults one step removed from our target audience of at-risk youth – health professionals, youth and/or health-related non-profit leaders, high school teachers, and target community members and advocates. Over an 18-month period soon after the initial PSA scripts had been made into videos, campaign representatives (CVP staff, YS staff and poets) participated in regional public health and medical conferences, school nurse meetings and trainings, and community activities, providing brief presentations and live poetry performances to promote the campaign. After these presentations, we invited audience stakeholders to fill out an anonymous paper survey to report their beliefs about the messaging. The survey included 8 Likert-scale questions gauging attitude about the campaign and acceptability of the messaging, a section soliciting which themes they felt would be most compelling to the target audience, and an invitation to receive more information about the campaign.
We collected a convenience sample of 334 stakeholder responses. The overwhelming majority had positive impressions of both the PSA messages and strategies for delivery (Table 2). After seeing the PSAs, nearly all respondents (96%) believed that youth can serve as agents of social change, increasing from only 23% prior to the presentation. The most common priority themes selected by stakeholders were how poverty restricts food choices, the contribution of neighborhood and recreational spaces to diabetes risk, ethnic disparities, and body image issues. The theme least commonly selected was taxing sugar, which is consistent with findings from a recent survey demonstrating less public support for pro-tax arguments than policies that limit taxation (Barry, Niederdeppe, & Gollust, 2013).
Table 2.
Stakeholder survey responses: Perceptions of Health and Community Stakeholders About The Bigger Picture, N = 334 respondents (convenience sample)
| Perception | Proportion |
|---|---|
| PSAs increased my awareness of environmental and social conditions that affect diabetes prevalence | 78% |
| Believe that youth can serve as agents of social change* | |
| Prior to seeing narratives | 23% |
| After seeing narratives | 96% |
| Health communication strategies used in this project are relevant to my organization | 92% |
| I would use the format of youth population-generated video PSAs in my work | 87% |
| Partnership and PSAs make me want to harness youth populations’ voices to promote social change and/or other health initiatives | 93% |
Note. Stakeholders included regional health professionals, leaders from youth- and/or health-related non-profits, high school teachers, and target community members and advocates.
p<.001 for McNemar’s Chi2 test
Campaign Dissemination: plan and evaluation
Public high school assemblies
To begin reaching the target audience, we utilized long-term relationships between YS and UCSF with regional public school districts and invited them to identify their priority schools (based on need and risk) to receive live presentations of the TBP campaign. The identified schools had a mean socioeconomically disadvantaged rate of 66% (i.e. qualify for free or reduced lunches) and a large number of minority students (on average, 33% Asian, 32% Latino, and 20% black), representing low-income and minority youth who are at higher risk of DM2 (public data from California’s Department of Education “School Accountability Report Card” for 2011–12 school year). These visits were provided free of charge to the schools. YS has a long history of pedagogy using large-group school assembly presentations to engage youth around social issues, and we decided to apply this format to campaign content. One YS poet staff with experience leading school visits was assigned to lead each visit.
We developed a script for a 1-hour high school assembly to be presented on a large screen using Power Point to display facts and figures with embedded PSA videos. The script allowed the poet leader space to first engage the student audience in participation through short verbal “icebreakers” - contests between classes and asking questions. The script emerged through an iterative process between CVP staff, YS staff, and poets, providing a balance of information that included a definition of DM2, statistics about the social factors and built environment that contribute to risk, embedded video TBP PSAs, resources for more information, and specific action steps. All information included in the presentation was also available on the campaign’s website. Depending on poet availability, at least one live performance per assembly augmented the video PSAs. On average, each assembly allowed time to view 5–6 PSAs. To evaluate whether we reached our target audience, we asked 3 demographics questions. To gauge campaign effectiveness, we asked 3 questions both at the beginning and end of the assembly to measure short-term change in knowledge and attitude. These questions were finalized through a group iterative process and tested for face validity and interpretability by YS poets. The questions were: 1. a true/false question asking if DM2 is preventable; 2. a multiple choice question (correct answer, “all of the above”) asking the student to identify environmental contributors in addition to individual behavior as affecting DM2 risk; and 3. a 1–5 Likert scale asking, “How much do you care about preventing diabetes?” We used Turning Point software® to insert the questions directly into the assembly presentation. A random sample of participating students utilized 80 handheld audience response systems (commonly called “clickers”) to give real-time responses.
Piloting the high school visits
To test the feasibility and initial acceptability of the high school student assembly, we piloted the presentations in 2 Bay Area public high schools. Six hundred high school students participated in 2 assemblies, with 135 of them responding to all pre/post questions using the audience response system “clickers”. Initially, the embedded demographics questions were at the end of the PowerPoint presentation, but during the first pilot assembly, time ran short and the poet leader was unable to collect that data; therefore, demographics are not shown. However, we observed short-term changes in knowledge of and attitudes about DM2 (Figure 3), with 2 of the 3 measures being statistically significant using McNemar’s Chi2 test – identifying the environment in addition to individual behavior as contributing to DM2 risk, and caring a lot about preventing DM2. Based on anecdotal teacher and student feedback, as well as poet assembly leader experience, the script and PowerPoint slides were modified into their final version. With these revisions, we have disseminated the campaign through assemblies and writing workshops in 13 high schools serving low-income and minority students in the San Francisco Bay Area. The evaluation results of these efforts demonstrated robust improvements across all 3 items and are the topic for an article currently in review (data not shown).
Figure 3.
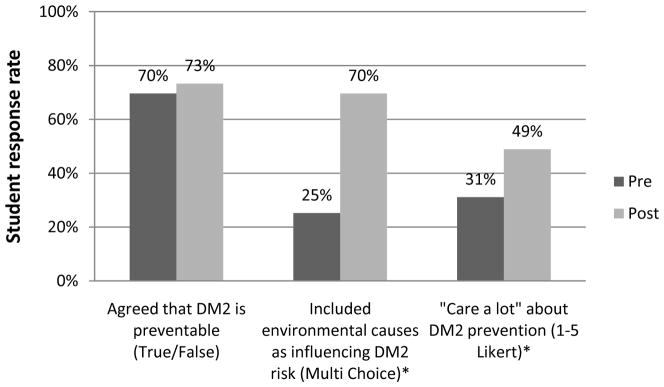
Change in student knowledge and attitude during school assembly pilots (n = 135). *McNemar’s χ2 p values < .001 for the question’s pre-post comparison.
On-line platform
To extend the reach of the targeted high school visits, we complemented the in-person dissemination with social media to promote the campaign website, video PSAs, and downloadable educational materials. One of the YS staff updates the campaign’s Facebook page and Twitter feed, driving traffic, Tweets, and Likes, and both were promoted during the high school presentations. Given that teens are heavy users of social media, we hope this will allow teen-to-teen dissemination of campaign information after initial exposure through high school visits. We planned to use web analytics to assess this reach, focusing on counts of video watches, toolkit and workbook downloads, Facebook likes, and Twitter followers. We are considering expanding TBP to include other social media platforms that are especially popular amongst our target audience.
Additional steps to increase exposure
Achieving exposure –ideally repeated exposure – of a larger target population to the campaign can be difficult and complex, especially if relying solely on an isolated on-line platform. Our initial budget allowed us to begin dissemination of this multi-layered campaign through high school visits and the on-line platform, which made an initial evaluation of reach and efficacy possible. This prompted initial exposure to the PSAs, either on-line or during a school visit, with a hope for subsequent peer-to-peer sharing through classroom discussion or web-based mechanisms. The messages were also disseminated to stakeholders and young people through community events and conferences, furthering the campaigns’ reach. Securing additional funding would allow us to grow these endeavors. In addition, we are working with three local health departments (San Francisco, Alameda, and Sonoma counties in California) through their public health campaigns to reduce sugary drink consumption (e.g. San Francisco’s “Shape Up” campaign, http://shapeupsfcoalition.org/), expanding our potential reach and bringing youth voices into the health discourse. We are also exploring potential partnerships in other regions to engage youth in food policy and education. Finally, through the network of YS-related youth poet organizations, we hope that future funding can be used to support poets in other cities and states to work in their own communities and write their own PSAs, furthering exposure.
Study Limitations
The model that we applied to the development and early implementation of the campaign PSAs and on-line platform is not the only possible model, and campaign developers should also consider other successful models, such as Photovoice (Gupta et al., 2013), student-led literacy school curricula (Pinkleton et al., 2008), and use of behavior theory and mass media (Hennessy et al., 2013). It remains to be determined how best to assess the effectiveness of the PSAs, and whether poetic license in writing the PSAs (e.g. PSA theme, race of actors, style of spoken word) should be influenced by opinions of target audience members. With the use of convenience samples in the evaluation of this formative work, there is potential for social desirability and selection bias; we attempted to minimize the former by keeping survey responses anonymous. Despite the importance of the public health literacy framework, we are not aware of any validated measures to evaluate this novel construct. Finally, it remains unclear how to best target PSAs to audiences, and how to best use the PSAs to promote civic engagement in their own communities around health disparities. Nevertheless, TBP campaign is gaining traction. In addition to county health departments adopting the campaign as part of their own efforts, in November 2013, TBP presented to the Institute of Medicine’s Round Table on Health Literacy, receiving a standing ovation (IOM Board on Population Health and Public Health Practice, 2013).
Conclusion
The present article aimed to demonstrate the application of social marketing and entertainment education strategies to a novel, public health literacy program to reduce DM2 risk. Through a participatory approach, TBP has created a fresh, engaging, and relevant campaign targeting youth hardest hit by the DM2 epidemic. The campaign’s success to date is likely the result of the youth poets’ curiosity, talent, and clear commitment to racial, social, and environmental justice, the talented videographer, and, most importantly, a strong academic-community partnership between two well-established organizations whose strong individual track records enabled them to take a risk, collaborate, and persevere to create an innovative campaign. Although the campaign evaluation is the subject of another article in review, we can report that the campaign effectively resonates with youth poets, minority high school students, and community and youth stakeholders, groups with differing levels of exposure to the campaign but who may serve as good proxies, or ambassadors, for the target population. We conclude that health communication campaigns using youth-generated spoken-word PSAs about the social and environmental determinants of DM2 can contribute to a more comprehensive model of health literacy. The authentic, personalized, creative, relevant, and sometimes hard-hitting messages have potential to engage and activate youth around social determinants of DM2. A major challenge will be how to harness the on-line platform to extend the campaign’s reach. Future research should investigate ways to foster new media to disseminate participatory approaches to address the socio-ecologic determinants of DM2 risk. It is our belief that youth are especially open to messages that increase their public health literacy, and we are optimistic that TBP campaign will engage youth of color to participate in, and even lead, initiatives to reverse the social and environmental drivers of the diabetes epidemic.
Acknowledgments
This research is the result of a close partnership between the University of California San Francisco Center for Vulnerable Populations at San Francisco General Hospital and Trauma Center, and the staff of Youth Speaks, whose wisdom, expertise, and candid feedback made this collaboration possible. The energy, creativity, and deep commitment to racial, social, and environmental justice of the youth poets are at the heart of this campaign, and without them, this campaign would not exist. The authors also thank their main videographer, Jamie DeWolf, for his incredible artistry and passion in creating the PSAs. Sarah Fine is Project Director of The Bigger Picture, and Hodari Davis is Creative Director for The Bigger Picture. The study team thanks their funders, listed below.
Funding
The UCSF Diabetes Family Fund for Innovative Patient Care, Education and Scientific Discovery; National Institute On Minority Health And Health Disparities of the National Institutes of Health (NIH) under Award Number P60MD006902; the NIH’s National Institute of Diabetes and Digestive and Kidney Diseases for The Health Delivery Systems-Center for Diabetes Translational Research (CDTR) P30DK092924; AT&T, Metta Fund, and the Department of Public Health’s Shape Up San Francisco through the San Francisco General Hospital Foundation; The California Diabetes Program; S.D. Bechtel Jr. Foundation; Stephen Bechtel Fund; and The California Endowment. Elizabeth Rogers was supported by the UCSF Division of General Internal Medicine’s NRSA institutional training grant (T32 HP19025). None of the views expressed in The Bigger Picture PSAs are those of the funders.
Contributor Information
ELIZABETH ROGERS, Applied Clinical Research Program, Divisions of Medicine and Pediatrics, University of Minnesota School of Medicine, Minneapolis, Minnesota, and Divisions of General Internal Medicine and Pediatrics, University of California San Francisco, San Francisco, California, USA.
SARAH FINE, University of California San Francisco Center for Vulnerable Populations, San Francisco General Hospital and Trauma Center, San Francisco, California, USA.
MARGARET A. HANDLEY, University of California San Francisco Center for Vulnerable Populations, San Francisco General Hospital and Trauma Center, and Department of Epidemiology and Biostatistics, University of California San Francisco, San Francisco, California, USA
HODARI DAVIS, Youth Speaks, San Francisco, California, USA.
JAMES KASS, Youth Speaks, San Francisco, California, USA.
DEAN SCHILLINGER, Division of General Internal Medicine, and University of California San Francisco Center for Vulnerable Populations, San Francisco General Hospital and Trauma Center, San Francisco, California, USA.
References
- Barry CL, Niederdeppe J, Gollust SE. Taxes on sugar-sweetened beverages: Results from a 2011 national public opinion survey. American Journal of Preventive Medicine. 2013;44(2):158–163. doi: 10.1016/j.amepre.2012.09.065. [DOI] [PubMed] [Google Scholar]
- Booske BC, Robert SA, Rohan AM. Awareness of racial and socioeconomic health disparities in the United States: The national opinion survey on health and health disparities, 2008–2009. Preventing Chronic Disease. 2011;8(4):A73. [PMC free article] [PubMed] [Google Scholar]
- Cowell AJ, Farrelly MC, Chou R, Vallone DM. Assessing the impact of the national ‘truth’ antismoking campaign on beliefs, attitudes, and intent to smoke by race/ethnicity. Ethnicity & Health. 2009;14(1):75–91. doi: 10.1080/13557850802257715. [DOI] [PubMed] [Google Scholar]
- Davis KC, Farrelly MC, Messeri P, Duke J. The impact of national smoking prevention campaigns on tobacco-related beliefs, intentions to smoke and smoking initiation: Results from a longitudinal survey of youth in the United States. International Journal of Environmental Research and Public Health. 2009;6(2):722–740. doi: 10.3390/ijerph6020722. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Demmer RT, Zuk AM, Rosenbaum M, Desvarieux M. Prevalence of diagnosed and undiagnosed type 2 diabetes mellitus among US adolescents: Results from the continuous NHANES, 1999–2010. American Journal of Epidemiology. 2013;178(7):1106–1113. doi: 10.1093/aje/kwt088. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farrelly MC, Davis KC, Haviland ML, Messeri P, Healton CG. Evidence of a dose-response relationship between “truth” antismoking ads and youth smoking prevalence. American Journal of Public Health. 2005;95(3):425–431. doi: 10.2105/AJPH.2004.049692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farrelly MC, Healton CG, Davis KC, Messeri P, Hersey JC, Haviland ML. Getting to the truth: Evaluating national tobacco counter marketing campaigns. American Journal of Public Health. 2002;92(6):901–907. doi: 10.2105/ajph.92.6.901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Farrelly MC, Nonnemaker J, Davis KC, Hussin A. The influence of the national truth campaign on smoking initiation. American Journal of Preventive Medicine. 2009;36(5):379–384. doi: 10.1016/j.amepre.2009.01.019. [DOI] [PubMed] [Google Scholar]
- Freedman DA, Bess KD, Tucker HA, Boyd DL, Tuchman AM, Wallston KA. Public health literacy defined. American Journal of Preventive Medicine. 2009;36(5):446–451. doi: 10.1016/j.amepre.2009.02.001. [DOI] [PubMed] [Google Scholar]
- Gollust SE, Cappella JN. Understanding public resistance to messages about health disparities. Journal of Health Communication. 2014 doi: 10.1080/10810730.2013.821561. [DOI] [PubMed] [Google Scholar]
- Gollust SE, Lantz PM. Communicating population health: Print news media coverage of type 2 diabetes. Social Science & Medicine (1982) 2009;69(7):1091–1098. doi: 10.1016/j.socscimed.2009.07.009. [DOI] [PubMed] [Google Scholar]
- Gollust SE, Lantz PM, Ubel PA. The polarizing effect of news media messages about the social determinants of health. American Journal of Public Health. 2009;99(12):2160–2167. doi: 10.2105/AJPH.2009.161414. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gollust SE, Lantz PM, Ubel PA. Images of illness: How causal claims and racial associations influence public preferences toward diabetes research spending. Journal of Health Politics, Policy and Law. 2010;35(6):921–959. doi: 10.1215/03616878-2010-034. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gupta RS, Lau CH, Warren CM, Lelchuk A, Alencar A, Springston EE, Holl JL. The impact of student-directed videos on community asthma knowledge. Journal of Community Health. 2013;38(3):463–470. doi: 10.1007/s10900-012-9630-4. [DOI] [PubMed] [Google Scholar]
- Handley MA, Santos MG, McClelland J. Reports from the field: Engaging learners as interpreters for developing health messages -- designing the ‘familias sin plomo’ English as a second language curriculum project. Global Health Promotion. 2009;16(3):53–58. doi: 10.1177/1757975909339773. [DOI] [PubMed] [Google Scholar]
- HEALTHY Study Group. Hirst K, Baranowski T, DeBar L, Foster GD, Kaufman F, Yin Z. HEALTHY study rationale, design and methods: Moderating risk of type 2 diabetes in multi-ethnic middle school students. International Journal of Obesity (2005) 2009;33(Suppl 4):S4–20. doi: 10.1038/ijo.2009.112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heider F. The psychology of interpersonal relations. New York: Wiley; 1958. [Google Scholar]
- Hennessy M, Romer D, Valois RF, Vanable P, Carey MP, Stanton B, Salazar LF. Safer sex media messages and adolescent sexual behavior: 3-year follow-up results from project iMPPACS. American Journal of Public Health. 2013;103(1):134–140. doi: 10.2105/AJPH.2012.300856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hofsteenge GH, Chinapaw MJ, Weijs PJ, van Tulder MW, Delemarre-van de Waal HA. Go4 it; study design of a randomised controlled trial and economic evaluation of a multidisciplinary group intervention for obese adolescents for prevention of diabetes mellitus type 2. BMC Public Health. 2008;8 doi: 10.1186/1471-2458-8-410. 410-2458-8-410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- IOM Board on Population Health and Public Health Practice. Implications of health literacy for public health: A workshop. Paper presented at the Beckman Center; Irvine, CA. 2013. Retrieved from http://www.iom.edu/Activities/PublicHealth/HealthLiteracy/2013-NOV-21.aspx. [Google Scholar]
- Iyengar S. How citizens think about national issues: A matter of responsibility. American Journal of Political Science. 1989;33(4):878–900. [Google Scholar]
- Kim SH, Willis LA. Talking about obesity: News framing of who is responsible for causing and fixing the problem. Journal of Health Communication. 2007;12(4):359–376. doi: 10.1080/10810730701326051. 779409223 [pii] [DOI] [PubMed] [Google Scholar]
- Klein JD, Dietz W. Childhood obesity: The new tobacco. Health Affairs; Health Aff. 2010;29(3):388–392. doi: 10.1377/hlthaff.2009.0736. [DOI] [PubMed] [Google Scholar]
- Kunkel D, Wilcox BL, Cantor J, Palmer E, Linn S, Dowrick P. Report of the APA task force on advertising and children. Washington, D.C: American Psychological Association; 2004. [Google Scholar]
- Lefebvre RC, Flora JA. Social marketing and public health intervention. Health Education & Behavior. 1988;15(3):299–315. doi: 10.1177/109019818801500305. [DOI] [PubMed] [Google Scholar]
- Lindstrom J, Absetz P, Hemio K, Peltomaki P, Peltonen M. Reducing the risk of type 2 diabetes with nutrition and physical activity - efficacy and implementation of lifestyle interventions in Finland. Public Health Nutrition. 2010;13(6A):993–999. doi: 10.1017/S1368980010000960. [DOI] [PubMed] [Google Scholar]
- Lundell H, Niederdeppe J, Clarke C. Public views about health causation, attributions of responsibility, and inequality. Journal of Health Communication. 2013;18(9):1116–1130. doi: 10.1080/10810730.2013.768724. [DOI] [PubMed] [Google Scholar]
- May AL, Kuklina EV, Yoon PW. Prevalence of cardiovascular disease risk factors among US adolescents, 1999–2008. Pediatrics. 2012;129(6):1035–1041. doi: 10.1542/peds.2011-1082. [DOI] [PubMed] [Google Scholar]
- Mayer-Davis EJ, Bell RA, Dabelea D, D’Agostino R, Jr, Imperatore G, Lawrence JM for Diabetes in Youth Study Group SEARCH. The many faces of diabetes in American youth: Type 1 and type 2 diabetes in five race and ethnic populations: The SEARCH for diabetes in youth study. Diabetes Care. 2009;32(Suppl 2):S99–101. doi: 10.2337/dc09-S201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mello MM, Studdert DM, Brennan TA. Obesity — the new frontier of public health law. The New England Journal of Medicine. 2006;354(24):2601–2610. doi: 10.1056/NEJMhpr060227. [DOI] [PubMed] [Google Scholar]
- Narayan KM, Boyle JP, Thompson TJ, Sorensen SW, Williamson DF. Lifetime risk for diabetes mellitus in the United States. JAMA: The Journal of the American Medical Association. 2003;290(14):1884–1890. doi: 10.1001/jama.290.14.1884. [DOI] [PubMed] [Google Scholar]
- Niederdeppe J, Bigman CA, Gonzales AL, Gollust SE. Communication about health disparities in the mass media. Journal of Communication. 2013;63(1):8–30. doi: 10.1111/jcom.12003. [DOI] [Google Scholar]
- Niederdeppe J, Bu QL, Borah P, Kindig DA, Robert SA. Message design strategies to raise public awareness of social determinants of health and population health disparities. The Milbank Quarterly. 2008;86(3):481–513. doi: 10.1111/j.1468-0009.2008.00530.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pinkleton BE, Austin EW, Cohen M, Chen YC, Fitzgerald E. Effects of a peer-led media literacy curriculum on adolescents’ knowledge and attitudes toward sexual behavior and media portrayals of sex. Health Communication. 2008;23(5):462–472. doi: 10.1080/10410230802342135. [DOI] [PubMed] [Google Scholar]
- Ritenbaugh C, Teufel-Shone NI, Aickin MG, Joe JR, Poirier S, Dillingham DC, Cockerham D. A lifestyle intervention improves plasma insulin levels among Native American high school youth. Preventive Medicine. 2003;36(3):309–319. doi: 10.1016/s0091-7435(02)00015-4. [DOI] [PubMed] [Google Scholar]
- Robert SA, Booske BC. US opinions on health determinants and social policy as health policy. American Journal of Public Health. 2011;101(9):1655–1663. doi: 10.2105/AJPH.2011.300217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Siegrist M, Hanssen H, Lammel C, Haller B, Halle M. A cluster randomised school-based lifestyle intervention programme for the prevention of childhood obesity and related early cardiovascular disease (JuvenTUM 3) BMC Public Health. 2011;11 doi: 10.1186/1471-2458-11-258. 258-2458-11-258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Singhal A, Rogers EM. Entertainment-education: A communication strategy for social change. Mahwah, N.J: L. Erlbaum Associates; 1999. [Google Scholar]
- Vos RC, Wit JM, Pijl H, Kruyff CC, Houdijk EC. The effect of family-based multidisciplinary cognitive behavioral treatment in children with obesity: Study protocol for a randomized controlled trial. Trials. 2011;12 doi: 10.1186/1745-6215-12-110. 110-6215-12-110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilmot EG, Davies MJ, Edwardson CL, Gorely T, Khunti K, Nimmo M, Biddle SJ. Rationale and study design for a randomised controlled trial to reduce sedentary time in adults at risk of type 2 diabetes mellitus: Project STAND (Sedentary Time ANd Diabetes) BMC Public Health. 2011;11 doi: 10.1186/1471-2458-11-908. 908-2458-11-908. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Winkleby MA, Feighery E, Dunn M, Kole S, Ahn D, Killen JD. Effects of an advocacy intervention to reduce smoking among teenagers. Archives of Pediatrics & Adolescent Medicine. 2004;158(3):269–275. doi: 10.1001/archpedi.158.3.269. [DOI] [PubMed] [Google Scholar]
- Zhang Y, Cooke R. Using a combined motivational and volitional intervention to promote exercise and healthy dietary behaviour among undergraduates. Diabetes Research and Clinical Practice. 2012;95(2):215–223. doi: 10.1016/j.diabres.2011.10.006. [DOI] [PubMed] [Google Scholar]