

Abstract
This study examined the relationship between self-reported drinking identity (SRDI), defined as how closely individuals believe drinking is a crucial aspect of their identity (Conner, Warren, Close, & Sparks, 1999), and alcohol use by considering drink-refusal self-efficacy (DRSE) as a potential mediator. Based on previous findings, we expected that SRDI would be negatively associated with DRSE and positively associated with drinking, and that DRSE would be negatively linked with drinking. Further, we expected that DRSE would mediate the association between SRDI and drinking. Participants included 1069 undergraduate students (M age = 22.93 years, SD = 6.29, 76.25% female) from a large southern university who completed computer-based study materials. Gender was associated with SRDI, each of the DRSE subscales, and drinking, indicating that males report greater SRDI, lower DRSE, and increased alcohol consumption. Consistent with expectations, SRDI was negatively linked with DRSE and positively linked with drinking. DRSE subscales were negatively associated with drinking. Further, four measurement models for latent variables were tested for SRDI and each of the three DRSE subscales. Results showed that the emotional relief and social subscales of DRSE mediated the association between SRDI and drinking, however this mediating relationship did not emerge for the opportunistic subscale. Implications of these results are discussed.
Keywords: identity, self-efficacy, alcohol, drinking
College drinking
Despite efforts in intervention and prevention of drinking among undergraduate students, college drinking remains problematic (Johnston, O'Malley, Bachman, & Schulenberg, 2012). Research demonstrates that undergraduate students drink heavily and as a consequence experience a range of alcohol-related problems ranging from poor class attendance to hangovers, trouble with the law, eating disorders, injury, depression, sexual assault, risky sexual behavior, and even death (Abbey et al., 2003; Dunn et al., 2002; Geisner, Larimer, & Neighbors, 2004; Hingson et al., 2005; Hingson, 2010; Kaysen et al., 2006; Koss & Gaines, 1993; Larimer et al., 1999; Wechsler et al., 1994; Wechsler et al., 2000). Prevalence estimates indicate that 80% of college students drink occasionally, 67% drink at least once per month, and 40% frequently drink several alcoholic beverages on a given occasion (Johnston, O'Malley, Bachman, & Schulenberg, 2006). Compared to 38% of non-college young adults, almost 44% of undergraduates report heavy episodic drinking (consuming five or more drinks in a row during the previous two weeks; SAMHSA, 2008). NIAAA (2007) reports that examine morbidity and mortality trends related to college alcohol use suggest that almost 20% of undergraduates meet DSM-IV criteria for alcohol dependence or abuse, and less than 5% seek alcohol treatment or counseling. Effort continues to be dedicated to the identification of psychological factors and mechanisms that interventions might effectively target (e.g., Malloy, Goldman, & Kington, 2002; Nelson, Toomey, Lenk, Erickson, & Winters, 2010). Additional research is needed to understand how to further translate scientific knowledge to a reduction in alcohol behaviors and consequent harm (Hingson, 2010).
Drinking identity
Reducing potential for harm associated with drinking requires better elucidated understanding of antecedents or precursors to using alcohol. The theory of planned behavior (TPB; Ajzen, 1991) is one theory related to behavior antecedents such as college drinking (Collins & Carey, 2007; Conner, Warren, Close, & Sparks, 1999; Huchting, Lac, & LaBrie, 2008). The TPB proposes that subjective norms, attitudes, and perceived behavioral control conjointly influence intentions, which in turn influence behavior (Ajzen, 1991). Recent work indicates that predictive validity of intent and behavior improves with the addition of the self-identity concept (e.g., Charng, Piliavin, & Callero, 1988; Fekadu & Kraft, 2001; Pierro et al., 2003; Smith et al., 2007). Self-identity has been described as the salient part of the self which is related to a behavior (Conner & Armitage, 1998). Individuals are motivated to maintain consistent self-views (Lalwani & Shavitt, 2009; Steele, 1988), and engaging in identity-relevant behavior may facilitate maintenance of consistency in the broader self-concept. As such, self-identity may be a useful predictor of behavior.
Drinking identity seems to be a central precursor to risky alcohol behavior. Drinking identity can be conceptualized as the extent to which a person perceives alcohol consumption to be a defining or central part of his/her identity (Conner et al., 1999). Furthermore, and consistent with broader work on self-identity's role in behavior, alcohol identity has been associated with college drinking (Casey & Dollinger, 2007; Dollinger, Rhodes, & Corcoran, 1993; Dollinger, 1996). Research on drinking identity has utilized implicit and explicit measures for identity. Implicit measures (e.g., the implicit association test; IAT; Greenwald, McGhee, & Schwartz, 1998) have found that drinking identity more reliably and consistently predicts drinking outcomes relative to other alcohol-related implicit associations (Foster, Neighbors, & Young, under review; Gray, Laplante, Bannon, Ambady, & Shaffer, 2011; Lindgren, Foster, Westgate, & Neighbors, 2013; Lindgren et al., 2013). Consistent with this, explicit alcohol identity, also termed self-reported drinking identity (SRDI), has demonstrated significant links with increased alcohol use (e.g., Foster, Yeung, & Prokhorov, under review; Reed et al., 2007). Importantly, increased alcohol consumption is in turn linked to the experience of more alcohol-related problems (e.g., Lindgren et al., 2013). Implicit and explicit measures for drinking identity converge in terms of conclusions that drinking identity is significantly linked with increases in alcohol use. Greater consideration of drinking identity would be consistent with a recent reformulation of the theory of planned behavior (see Fekadu & Kraft, 2001) that demonstrated that including measures of identification with a behavior increases the predictability of that behavior. Moreover, evaluation of factors that might potentially influence the relationship between drinking identity and alcohol use is of great importance, particularly as they relate to initiation and encouragement of continued behavior change.
Drink-refusal self-efficacy
Beliefs with respect to self-efficacy and behavior change are recognized as the foundation of human agency (Bandura, 1982; 2000). Broadly, self-efficacy is conceptualized as self-perceived competence related to beliefs that one can cope with situations (Bandura, 2000). In particular, drink refusal self-efficacy (DRSE) relates to one's belief that he or she is able to resist, refuse, or turn down alcohol, and DRSE is a useful predictor of drinking (e.g., Baldwin, Oei, & Young, 1993; Morawska & Oei, 2005; Oei & Morawska, 2004; Skutle, 1999; Solomon & Annis, 1990). Behavioral scientists concerned with risky alcohol practices among college students have explored drink refusal self-efficacy (DRSE; e.g., Cho, 2006; Young, Oei, & Crook, 1991), which conceptually refers to an individual's self-perceived ability to resist alcohol. DRSE includes three dimensions: 1) drinking directed towards affect regulation or emotional relief (e.g., when stressed or anxious); 2) drinking involving social settings (e.g., in a social setting such as a party); and 3) drinking when an opportunity arises (e.g., being offered or given a drink; Lee & Oei, 1993; Young et al., 1991). Each of the three DRSE factors assesses a similar construct in different situations (Young, Hasking, Oei, & Loveday, 2007).
Early research suggests that college students low in social and opportunistic DRSE drink more relative to those high in these aspects (Young et al., 1991). Furthermore, general DRSE contributes unique variance to the prediction of drinking among undergraduates when positive and negative alcohol expectancies, which are known to predict drinking, are controlled (Oei & Jardim, 2007; Young, Conner, Ricciardelli, & Saunders, 2006). Recent work further shows that DRSE is a reliable proximal predictor of risky alcohol use, mediating effects of alcohol expectancies, and impulsivity (Gullo, Dawe, Kambouropoulos, Stalger, & Jackson, 2010). Among college students, DRSE is inversely related to intentions to drink and consumption levels (Baldwin, Oei, & Young, 1993; Collins, Witkiewitz, & Larimer, 2011). Research indicates that DRSE mediates the relationship between alcohol expectancies and consumption (e.g., Gullo, Dawe, Kambouropoulos, Staiger, & Jackson, 2010; Morawska & Oei, 2005), is associated with drinking in non-clinical samples (e.g., Young, Hasking, Oei, & Loveday, 2007), and is linked with abstinence following treatment (Maisto, Connors, & Zywiak, 2000). Research further shows that DRSE moderates the effect of protective behavioral strategies (PBS) on drinking such that individuals low in PBS and DRSE are at increased risk for drinking (Ehret, Ghaidarov, & Labrie, 2013) relative to those high in either. Further, DRSE is shown to mediate the relationship between alcohol expectancies and problems (Connor et al., 2011) and moderate the effect of alcohol expectancies on drinking (Oei & Jardim, 2007). Importantly, DRSE has consistently been associated with decreased drinking (e.g., Connor, George, Gullo, Kelly, & Young, 2011; Foster, Neighbors, & Young, under review; Oei & Jardim, 2007). Thus, the inclusion of DRSE into alcohol-related harm reduction efforts among college students is highly encouraged (Cho, 2006; Collins et al., 2011).
Mediators of the association between drinking identity and drinking have not been previously examined. We propose that self-efficacy is likely to mediate this association. To some extent, drinking identity may be viewed as a global association between the self and alcohol. This likely increases the salience of alcohol cues in the environment as well as availability of alcohol in considering from a range of possible behaviors. For a person who is higher in drinking identity, alcohol is an important part of the self-concept whereas for a person who is lower in drinking identity, alcohol is not integrated in the self-definition. To the extent that these deductions are correct, we would expect that it would be much easier for a person low in drinking identity to refuse alcohol across a variety of situations whereas it would be more difficult for a person who is higher in drinking identity. Thus, we considered DRSE as a mediator in the relationship between SRDI and drinking. Based on previous literature, we expected that SRDI would be negatively associated with DRSE and positively associated with drinking. We further expected that DRSE would be negatively associated with drinking. Moreover, we expected that DRSE would mediate the association between SRDI and drinking.
Method
Participants and procedure
The current research included 1067 college students (76.25% female) from a large southern university who completed computer-based study material as part of a larger intervention. Data for the present study came from the baseline assessment of the larger longitudinal trial. Participants were recruited via flyers and in-class recruitment and received extra credit in exchange for participation. Participants' mean age was 22.93 years (SD = 6.29). The sample consisted of the following races: 34% Caucasian, 19% Black/African American, 20.6% Asian/Pacific Islander, 6% Multi-Ethnic, 0.4% Native American/American Indian, and 20% Other. Additionally, 30% of participants reported as Hispanic/Latino.
Measures
Demographics
Participants reported demographic information including year in school, race, ethnicity, gender, and age.
Alcohol use
Alcohol consumption was measured using the Daily Drinking Questionnaire (Collins et al., 1985; Kivlahan et al., 1990), which measures the number of standard alcoholic beverages consumed on each day of the week (Monday-Sunday) within the previous three months. Scores represent the average number of alcoholic beverages consumed over the course of each week during the past month. Relative to other alcohol use indices (e.g., binge drinking frequency, estimated blood alcohol levels), weekly drinking is a reliable index of problems among college students (Borsari, Neal, Collins, & Carey, 2001).
Drinking identity
Self-reported drinking identity (SRDI) was evaluated using a five-item scale adapted from the Smoker Self-Concept Scale developed by Shadel and Mermelstein (1996). The SRDI scale assesses the degree to which individuals believe alcohol consumption is integrated with their own self-concept using a scale ranging from 1= Strongly disagree to 7 = Strongly agree (Shadel & Mermelstein, 1996). A sample item is “drinking is a part of ‘who I am’”. A higher mean score indicates a stronger belief that drinking plays a part in the individual's life and personality, and others' perceptions of the role of alcohol in his or her life (Lindgren, Neighbors et al., 2013). The scale was reliable and positively associated with alcohol consumption, alcohol cravings, and alcohol-related problems among college students Lindgren, Neighbors et al., 2013).
Drink refusal self-efficacy
The Drink Refusal Self-Efficacy (DRSE) questionnaire, a 19-item scale, was used to assess self-efficacy related to resisting drinking (Young, Hasking, Oei, & Loveday, 2007). The measure has three subscales including social pressure refusal self-efficacy, opportunistic refusal self-efficacy, and emotional relief refusal self-efficacy. Participants were provided a list of situations in which individuals may find themselves drinking and were asked to rate their ability to resist or refuse drinking on a six-point Likert scale ranging from 1 = “I am very sure I could NOT resist drinking” to 6 = “I am very sure I could resist drinking”. Sample items are “when someone offers me a drink” (social pressure), “when I am on the way home from school” (opportunistic), and “when I am angry” (emotional relief). A higher mean score in the subscale indicates a higher level of self-efficacy in refusing drinking. The scale was validated among adolescents in Australia with a stable three-factor structure and satisfactory Cronbach's alphas (Young, Hasking, Oei, & Loveday, 2007). The three subscales were also negatively associated with both frequency and volume of alcohol consumption per week (Young, Hasking, Oei, & Loveday, 2007).
Analytic plan
Descriptive statistics including means, standard deviations, and distribution statistics were computed for major variables. Pearson correlation analysis was conducted to examine the associations among variables. These analyses were conducted by SPSS 19.0. Structural Equation Modeling (SEM) was used to evaluate the fitness of the hypothesized models in explaining the associations among SRDI, DRSE and drinking. It was conducted with AMOS 20.0 (IBM, 2011). Before conducting SEM, we estimated the goodness-of-fit of the measurement models by confirmatory factor analysis (CFA). For the measurement models of SRDI and DRSE, scale items were used as the indicators of the latent variable. For standardized factor loadings, we used .70 as a criterion to ensure construct validity (Hulland, 1999). Due to the fact that each latent variable was composed of items from within the same measure, covariances for errors were expected. Error covariances were added according to the modification indices that significantly improve the measurement model fit (Kline, 2005; MacCallum & Austin, 2000).
The hypothesized mediation model was evaluated through examination of model fit and standardized path loadings (see Figure 1; Kline, 2005; MacCallum & Austin, 2000). In the structural model, number of drinks per week was used as the dependent variable. In the hypothesized models, mediation was tested through an analysis of direct and indirect effects or path coefficients, among the latent and observed variables (MacKinnon, 2008). To ensure the stability of the path coefficient estimates, the analysis for mediation model was also supplemented with 2000 Bollen-Stine bootstrap replications. Significance of indirect effect was examined by the 95% confidence intervals (CI) after bootstrapping. Confidence intervals were computed through the 2000 estimates of the indirect effect bootstrap samples. The highest and lowest 2.5% of the indirect effect estimates determined the confidence intervals. An indirect effect was considered statistically significant if the 95% CI did not include zero.
Figure 1.
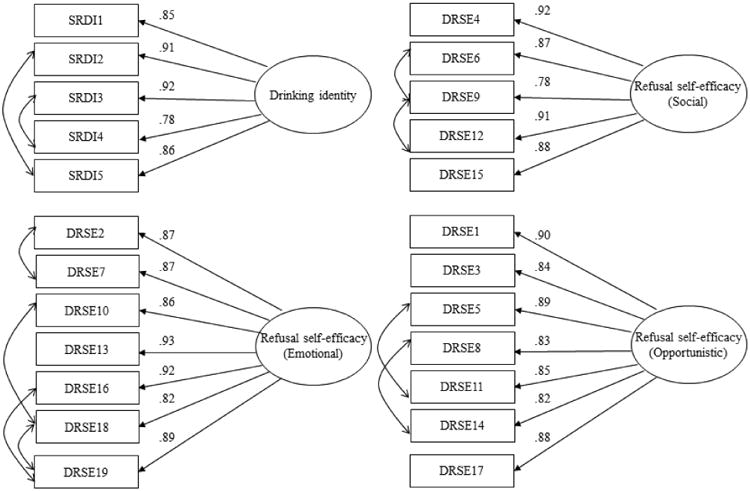
Latent variable measurement models for SRDI and DRSE. All factor loadings significant at p < .001.
Model goodness-of-fit was evaluated using several indices. Favorable fit indices included a chi-square value with a non-significant p-value, a Root Mean Square Error of Approximation (RMSEA) with values ≤0.08, and a Comparative Fit index (CFI), a Normed Fit Index (NFI), and Tucker-Lewis Index (TLI) with values ≥0.95 (Hu & Bentler, 1999; Kelloway, 1998; Steiger, 1990). Due to the relatively large sample (N = 1067) and the fact that chi-square was sensitive to sample size (Hoe, 2008), we did not use the statistical significance of chi-square value as the primary index to evaluate the goodness-of-fit of the overall model.
Results
Descriptive statistics and correlations among major variables
Descriptive statistics of major variables, Cronbach's alphas of the measures, and inter-correlations among major variables are presented in Table 1. All measures demonstrated good internal consistency with alpha coefficients ranging from .94 to .96. Gender was significantly associated with SRDI (r = .13, p <.01), emotional relief DRSE (r = .-12, p <.01), social DRSE (r = -.10, p <.01), and opportunistic DRSE (r = -16, p <.01). Gender was also significantly associated with number of drinks consumed per week (r = .12, p <.01), indicating that males had higher levels of SRDI, lower levels of DRSE, and consumed more drinks per week. Results showed that SRDI was negatively associated with DRSE. Findings further revealed that SRDI was positively associated with number of drinks consumed per week (r = .37, p <.01), such that a higher level of SRDI was associated with increased number of drinks per week. Emotional relief, social, and opportunistic subscales of DRSE were negatively associated with number of drinks per week (r = -.27, -.40, and -.16 respectively, p <.01), such that higher levels of emotional relief, social, and opportunistic DRSE were associated with decreased number of drinks per week. Thus, our first and second hypotheses were supported.
Table 1. Means, Standard Deviations, and Correlations among Variables.
| 1. | 2. | 3. | 4. | 5. | |
|---|---|---|---|---|---|
| 1. SRDI | -- | ||||
| 2. Emotional DRSE | -.29** | -- | |||
| 3. Social DRSE | -.31** | .66** | -- | ||
| 4. Opportunistic DRSE | -.29** | .80** | .53** | -- | |
| 5. Number of drinks per week | .37** | -.27** | -.40** | .-16** | -- |
| 6. Gender | .13** | -.12** | -.10** | -.16** | .12** |
| Mean | 0.46 | 5.30 | 4.53 | 5.61 | 3.87 |
| Standard Deviation | 1.03 | 1.15 | 1.49 | 0.93 | 6.40 |
| Cronbach's alpha | .94 | .96 | .94 | .95 | NA |
Note. N=1067.
p < .01,
p < .05.
Gender: Male (1), Female (0).
Latent variable measurement models
Four measurement models for latent variables were individually constructed and tested (see Figure 1) for use in the structural equation model. The latent variables for SRDI, emotional relief DRSE, social DRSE, and opportunistic DRSE were respectively constructed by 5, 7, 5, and 7 items in the measurement scales. With the inclusion of two covariances for errors, the measurement model for SRDI had a satisfactory fit (χ2 (3) =9.75, p = 021, CFI = .988; NFI = .998; TLI = .995; RMSEA =.047). With the inclusion of four covariances for errors, the measurement model for emotional relief DRSE had a satisfactory fit (χ2 (10) = 69.86, p < .001, CFI = .993; NFI = .992; TLI = .985; RMSEA =.076). With the inclusion of two covariances for errors, the measurement model for social DRSE had a satisfactory fit (χ2 (3) = 9.36, p = .025, CFI = .999; NFI = .998; TLI = .996; RMSEA =.045). With the inclusion of two covariances for errors, the measurement model for opportunistic DRSE had a satisfactory fit (χ2 (12) = 50.26, p <001, CFI = .994; NFI = .993; TLI = .990; RMSEA =.056). For all four latent variables, all indicators had significant factor loadings with values greater than .70 (see Figure 1), showing that the indicators were sufficiently associated with the latent variable.
Mediation Models
SEM was conducted to examine the fitness of the proposed model which hypothesized that DRSE mediated the relationship between SRDI and drinking. Each of the three subscales of DRSE was examined as mediator in three separate mediation models. To account for potential influence of gender on the constructs of interests (including SRDI, DRSE, and drinking), gender was included in the model as it was significantly associated with SRDI, DRSE, and drinking.
Using emotional relief DRSE as the mediator, Model 1 (Figure 2) showed a satisfactory fit in predicting number of drinks per week (χ2 (67) =226.79, p < 001, CFI = .988; NFI = .983; TLI = .983; RMSEA =.048). The standardized path coefficients supported the negative association between SRDI and emotional relief DRSE (β = -29, p <001), and the negative association between emotional relief DRSE and drinking (β = -.18, p <.001). Results from bootstrapping supported the presence of a partial mediation effect, as both the indirect effect from SRDI to drinking via emotional relief DRSE (β = 0.05, p = .001; 95% CI= 0.03, 0.08) and the direct effect from SRDI to drinking (β = 0.33, p = .001; 95% CI = 0.24, 0.41) were greater than zero in the 95% confidence intervals. Therefore, a partial mediation effect of emotional relief DRSE between SRDI and drinking was supported.
Figure 2.
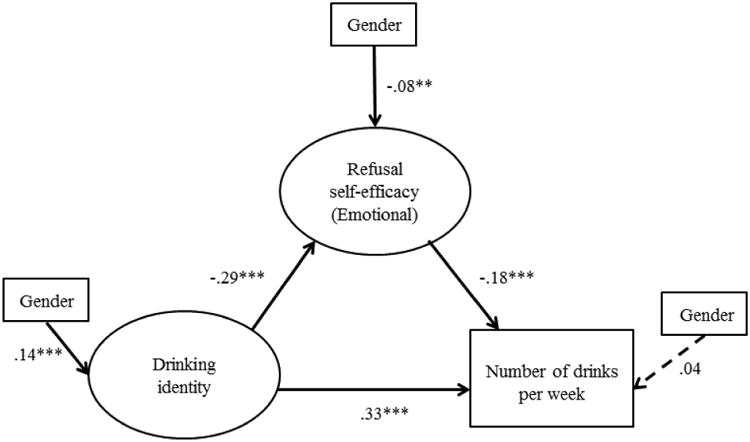
Partial mediation model for the relationships among SRDI, emotional DRSE, and drinking. Standardized path coefficients are presented. Broken lines represent non-significant paths.
Note. Gender was included as a covariate with significant bivariate correlations with SRDI, emotional DRSE and drinking. *p <.05; ** p <.01, *** p <.001.
Using social DRSE as the mediator, Model 2 (Figure 3) showed a satisfactory fit in predicting number of drinks per week (χ2 (46) = 121.82, p < .001, CFI = .992; NFI = .987; TLI = .989; RMSEA =.040). The standardized path coefficients supported the negative association between SRDI and social DRSE (β = -32, p <001), and the negative association between social DRSE and drinking (β = -31, p <001). Results from bootstrapping supported the presence of a partial mediation effect, as both the indirect effect from SRDI to drinking via social DRSE (β = 0.10, p = .001; 95% CI= 0.08, 0.13) and the direct effect from SRDI to drinking (β = 0.28, p =.001; 95% CI = 0.22, 0.33) were greater than zero in the 95% confidence intervals. Therefore, a partial mediation effect of social DRSE between SRDI and drinking was supported.
Figure 3.
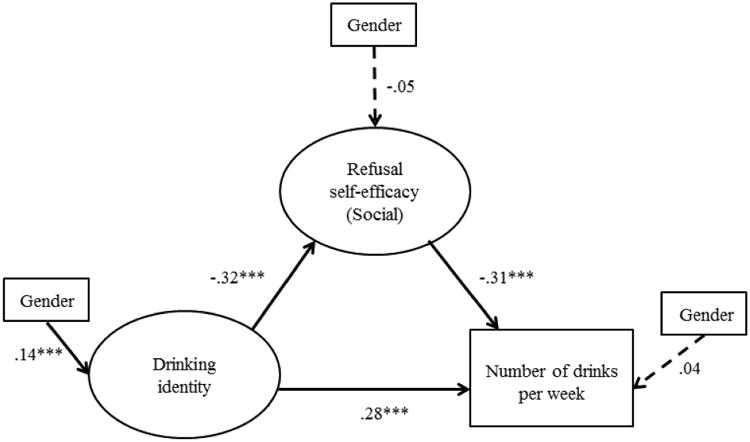
Partial mediation model for the relationships among SRDI, social DRSE, and drinking. Standardized path coefficients are presented. Broken lines represent non-significant paths.
Note. Gender was included as a covariate with significant bivariate correlations with SRDI, emotional DRSE, and drinking. *p <.05; ** p <.01, *** p <.001.
Using opportunistic DRSE as the mediator, Model 3 (Figure 4) showed a satisfactory fit in predicting number of drinks per week (χ2 (69) = 228.30, p <.001, CFI = .986; NFI = .980; TLI = .982; RMSEA =.047). The standardized path coefficients supported the negative association between SRDI and opportunistic DRSE (β = -.28, p <001), but not the negative association between opportunistic DRSE and drinking (β = -.05, p =13). Results from bootstrapping did not support the presence of any mediation effect, as the indirect effect from SRDI to drinking via opportunistic DRSE included zero in the 95% confidence intervals (β = 0.01, p = .001; 95% CI= -.01, 0.04). No mediation effect of opportunistic DRSE between SRDI and drinking was supported.
Figure 4.
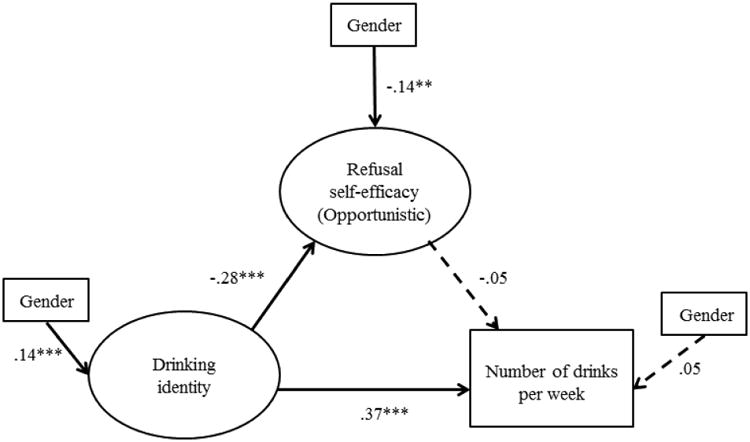
Structural equation model for the relationships among SRDI, opportunistic DRSE, and drinking. Standardized path coefficients are presented. Broken lines represent non-significant paths.
Note. Gender was included as a covariate with significant bivariate correlations with SRDI, emotional DRSE, and drinking. *p <.05; ** p <.01, *** p <.001.
Discussion
The present research bridges a gap in the literature by considering DRSE as a mediator of the relationship between SRDI and drinking, and further elucidates how the intersection between DRSE and SRDI impacts alcohol use. This study examined the relationship between SRDI and drinking by considering DRSE as a potential mediator. Our findings largely supported our expectations. Not included in initial hypotheses but incorporated into analyses was gender, which was found to significantly associate with all major variables in the study (SRDI, DRSE, and drinking). Gender differences in drinking have been demonstrated in college samples, and higher prevalence of binge drinking and related problems have been shown among males relative to females (e.g., Foster & Neighbors, 2013; Grant et al., 2004; Seo & Li, 2009; Slutske, 2005; Wells et al., 2010). Our findings are consistent with the literature in that males reported increased number of alcoholic beverages consumed per week. Additionally, results showed that males self-identified more strongly with drinking relative to females. It is possible that increased SRDI among males might be linked with the perspective of alcohol being more of a male domain (male centered or dominated) than female (Perkins, 1992). Gender theorists suggest that particular aspects of the male gender role (e.g., masculine norms, gender role stress, or attitudes that heavy drinking is a symbol of masculinity) may be associated with alcohol behavior (Capraro, 2000; Courtenay, 2000, Lemle & Mishkind, 1989; Mahalik et al., 2003; McCreary, Newcomb, & Sadave, 1999). Our findings further indicated that males reported lower DRSE relative to females, findings not inconsistent with previous work which often include gender in prediction models as a covariate due to its consistent correlation with DRSE (e.g., Ehret, Ghaidarov, & LaBrie, 2013). Generally, our findings with respect to gender differences support the need to take gender and other individuals' risk factors that contribute to elevated intoxication and negative consequences into consideration.
Consistent with expectations based on previous research (Foster et al., under review), we found that SRDI and DRSE were negatively associated. SRDI was almost equally associated with each of the three DRSE subscales, suggesting that regardless of context or situation, drinking identity may influence one's assessment of how able one is to resist drinking to the same extent. Also consistent with what was predicted, we found positive associations between drinking identity and alcohol consumption, findings which support the literature (Foster, Neighbors, & Young, under review; Foster, Yeung, & Prokhorov, under review; Gray, Laplante, Bannon, Ambady, & Shaffer, 2011; Lindgren, Foster, Westgate, & Neighbors, 2013). Moreover, and in line with predictions, DRSE was negatively linked with drinking, results which replicate previous work (Collins et al., 2011). Our results provide additional support for the evaluation of factors that might potentially influence relationships between drinking identity and alcohol use. Thoughtful and strategic tailoring of intervention strategies to target these concepts would be worthwhile.
As was expected, SEM and bootstrapping demonstrated mediating effects for social and emotional DRSE between SRDI and drinking. This is consistent with the notion that individuals who view alcohol as a large part of self-image engage in increased drinking due, in part, to decreases in social or emotional DRSE. Stated differently, these findings suggest that individuals who strongly self-identify with alcohol may drink or not drink primarily to the extent to which he or she believes that they are able to resist or refuse alcohol. Moreover, this is particularly true for situations when individuals might drink to alleviate stress (emotional relief) or in settings such as a party (social pressure). Implications are that modifying social or emotional DRSE might be an important step in reducing or breaking the link between SRDI and problematic alcohol use.
The lack of support for opportunistic DRSE (e.g., consuming alcohol when an occasion for drinking arises such as being offered a drink) as a mediator was contrary to expectations. This difference may stem from the description of opportunistic DRSE relating to belief in one's ability to refuse alcohol when a drinking opportunity arises. Findings indicate that opportunistic DRSE is a weaker predictor of drinking relative to social or emotional DRSE, which may suggest that alcohol consumption (or resisting consumption) among undergraduate students might be more a function of strategies and skills that overlap with resisting social pressure or regulating negative affect, rather than when an opportunity arises. It is well documented that social forces are among the most commonly cited reasons that college students list for drinking (e.g., Litt, Lewis, Stahlbrandt, Firth, & Neighbors, 2012), and that regulating negative affect also plays a large role in alcohol behaviors among young adults (e.g., Neighbors, Larimer, Geisner, & Knee, 2004). Thus, it stands to reason that beliefs in one's refusal skills with respect to drinking might be more closely related to social and affective aspects among college students relative to opportunistic DRSE.
Overall, these findings may have important clinical implications as they support the perspective that modifying DRSE clinically (e.g., increasing a person's belief that they can resist alcohol) may break or reduce the link between SRDI and problem drinking. This perspective has been a focus for psychotherapy outcome research (e.g., Witkiewitz, Donovan, & Hartzler, 2012) and evidence from behavioral interventions for alcohol dependence suggest that some of the variance in intervention efficacy might be attributed to individual differences in DRSE. Additionally, recent work evaluating whether DRSE training coupled with a cognitive behavioral intervention was effective in reducing drinking indicate that changes in DRSE mediate the relationship between the intervention and drinking outcomes (Witkiewitz et al., 2012), and this is consistent with previous work (e.g., Komro et al., 2001). An important next step, and one noted by Witkiewitz and colleagues (2012) is to conduct an experimentally designed study of DRSE as the agent of change. For example, a study utilizing randomization of participants to either receive DRSE training or not would allow for manipulation of DRSE and evaluation of resulting changes in drinking. Further, improving SRDI (e.g., reducing a person's self-identification with alcohol) may indirectly reduce problem drinking behaviors. This perspective is consistent with literature which suggests that computer-based practice programs that involve learning a new contingency related to drinking can reduce cognitive biases such as identification or association with drinking (e.g., reductions in SRDI; Clerkin & Teachman, 2010; Wiers et al., 2011). Furthermore, findings indicate that attempting to alter specifically opportunistic DRSE may have less clinical utility when intervening with clients high in SRDI.
Limitations and future directions
The strengths of this research must be considered in light of its limitations. Using cross-sectional samples has limitations related to causal inferences following mediation tests. Relationships between the variables and constructs of interest were not longitudinally measured, and thus, causality of the relationships cannot be elucidated. Moreover, changes that may occur among the constructs over time cannot be evaluated. Additional research is needed to examine longitudinal relationships between SRDI, DRSE, and alcohol consumption. Relatedly, mediation models ideally should evaluate predictors assessed at an initial time point followed by mediators assessed at a subsequent time point, and outcomes at a third time point (Kenny, Kashy, & Bolger, 1998; Nock, 2007), which is a limitation of the present research study as temporal precedence was not established. This research represents a logical starting point for a critical examination of temporal precedence and predictive validity of the models. Replications of this work are needed in longitudinal samples to mitigate causal ambiguity.
Highlights.
We evaluated drinking identity as a moderator of drinking
Drinking identity and drink-refusal self-efficacy interacted to predict drinking
Four measurement models for latent variables were tested
Acknowledgments
Role of Funding Sources: This research was not supported by any grant.
Footnotes
Contributors: Dawn Foster designed the study, wrote the protocol, conducted literature searches, provided summaries of previous research studies, and drafted the intro, method, and discussion sections. Nelson Yeung conducted the statistical analysis and wrote the results section. Clayton Neighbors contributed by assisting with conceptualizing theoretical bases and providing feedback to the manuscript. All authors contributed to and have approved the final manuscript.
Conflict of Interest: All authors declare that they have no conflicts of interest.
References
- Abbey A, Buck PO, Zawacki T, Saenz C. Alcohol's effects on perceptions of a potential date rape. Journal of Studies on Alcohol. 2003;64(5):669–677. doi: 10.15288/jsa.2003.64.669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ajzen I. The theory of planned behavior. Organizational Behavior and Human Decision Processes. 1991;50:179–211. [Google Scholar]
- Baldwin AR, Oei TP, Young R. To drink or not to drink: The differential role of alcohol expectancies and drinking refusal self-efficacy in quantity and frequency of alcohol consumption. Cognitive Therapy and Research. 1993;17(6):511–530. [Google Scholar]
- Bandura A. Self-efficacy mechanisms in human agency. American Psychologist. 1982;37:122–147. [Google Scholar]
- Bandura A. Health promotion from the perspective of social cognitive theory. In: Norman P, Abraham C, Conner M, editors. Understanding and changing health behaviour: From health beliefs to self-regulation. Amsterdam Netherlands: Harwood Academic Publishers; 2000. p. 299-339. [Google Scholar]
- Borsari B, Neal DJ, Collins SE, Carey KB. Differential utility of three indexes of risky drinking for predicting alcohol problems in college students. Psychology of Addictive Behaviors. 2001;15:321–324. doi: 10.1037//0893-164x.15.4.321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Capraro RL. Why college men drink: Alcohol, adventure, and the paradox of masculinity. Journal of American College Health. 2000;48(6):307–315. doi: 10.1080/07448480009596272. [DOI] [PubMed] [Google Scholar]
- Casey PF, Dollinger SJ. College students' alcohol-related problems: An autophotograpic approach. Journal of Alcohol and Drug Education. 2007;51(2):8–25. [Google Scholar]
- Charng H, Piliavin JA, Callero PL. Role identity and reasoned action in the prediction of repeated behavior. Social Psychology Quarterly. 1988;51(4):303–317. [Google Scholar]
- Cho H. Readiness to change, norms, and self-efficacy among heavy-drinking college students. Journal of Studies on Alcohol. 2006;67(1):131–138. doi: 10.15288/jsa.2006.67.131. [DOI] [PubMed] [Google Scholar]
- Clerkin EM, Teachman BA. Training implicit social anxiety associations: An experimental intervention. Journal of Anxiety Disorders. 2010;24:300–308. doi: 10.1016/j.janxdis.2010.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins SE, Carey KB. The theory of planned behavior as a model of heavy episodic drinking among college students. Psychology of Addictive Behaviors. 2007;21(4):498–507. doi: 10.1037/0893-164X.21.4.498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Collins R, Parks GA, Marlatt G. Social determinants of alcohol consumption: The effects of social interaction and model status on the self-administration of alcohol. Journal of Consulting and Clinical Psychology. 1985;53:189–200. doi: 10.1037//0022-006x.53.2.189. [DOI] [PubMed] [Google Scholar]
- Collins SE, Witkiewitz K, Larimer ME. The Theory of Planned Behavior as a predictor of growth in risky college drinking. Journal of Studies on Alcohol and Drugs. 2011;72(2):322–332. doi: 10.15288/jsad.2011.72.322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conner M, Armitage CJ. Extending the theory of planned behaviour: A review and avenues for further research. Journal of Applied Social Psychology. 1998;28:1430–1464. [Google Scholar]
- Conner M, Warren R, Close S, Sparks P. Alcohol consumption and the theory of planned behaviour: An examination of the cognitive mediation of past behaviour. Journal of Applied Social Psychology. 1999;29:1675–1703. [Google Scholar]
- Connor JP, George SM, Gullo MJ, Kelly AB, Young RD. A prospective study of alcohol expectancies and self-efficacy as predictors of young adolescent alcohol misuse. Alcohol and Alcoholism. 2011;46(2):161–169. doi: 10.1093/alcalc/agr004. [DOI] [PubMed] [Google Scholar]
- Courtenay WH. Constructions of masculinity and their influence on men's well-being: A theory of gender and health. Social Science & Medicine. 2000;50(10):1385–1401. doi: 10.1016/s0277-9536(99)00390-1. [DOI] [PubMed] [Google Scholar]
- Dollinger SJ. Autophotographic identities of young adults: With special reference to alcohol, athletics, achievement, religion, and work. Journal of Personality Assessment. 1996;67(2):384–398. doi: 10.1207/s15327752jpa6702_12. [DOI] [PubMed] [Google Scholar]
- Dollinger SJ, Rhodes KA, Corcoran KJ. Photographically portrayed identities, alcohol expectancies, and excessive drinking. Journal of Personality Assessment. 1993;60(3):522–531. doi: 10.1207/s15327752jpa6003_9. [DOI] [PubMed] [Google Scholar]
- Dunn EC, Larimer ME, Neighbors C. Alcohol and drug-related negative consequences in college students with bulimia nervosa and binge eating disorder. International Journal of Eating Disorders. 2002;32(2):171–178. doi: 10.1002/eat.10075. [DOI] [PubMed] [Google Scholar]
- Ehret PJ, Ghaidarov TM, Labrie JW. Can you say no? Examining the relationship between drinking refusal self-efficacy and protective behavioral strategy use on alcohol outcomes. Addictive Behaviors. 2013;38(4):1898–1904. doi: 10.1016/j.addbeh.2012.12.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fekadu Z, Kraft P. Self-identity in planned behavior perspective: Past behavior and its moderating effects on self-identity–intention relations. Social Behavior and Personality. 2001;29(7):671–685. [Google Scholar]
- Fekadu Z, Kraft P. Expanding the theory of planned behaviour: The role of social norms and group identification. Journal of Health Psychology. 2002;7(1):33–43. doi: 10.1177/1359105302007001650. [DOI] [PubMed] [Google Scholar]
- Foster DW, Neighbors C. Self-consciousness as a moderator of the effect of social drinking motives on alcohol use. Addictive Behaviors. 2013;38(4):1996–2002. doi: 10.1016/j.addbeh.2013.01.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Geisner IM, Larimer ME, Neighbors C. The relationship among alcohol use, related problems, and symptoms of psychological distress: Gender as a moderator in a college sample. Addictive Behaviors. 2004;29:843–848. doi: 10.1016/j.addbeh.2004.02.024. [DOI] [PubMed] [Google Scholar]
- Grant BF, Dawson DA, Stinson FS, Chou S, Dufour MC, Pickering RP. The 12-month prevalence and trends in DSM-IV alcohol abuse and dependence: United States, 1991-1992 and 2001-2002. Drug and Alcohol Dependence. 2004;74(3):223–234. doi: 10.1016/j.drugalcdep.2004.02.004. [DOI] [PubMed] [Google Scholar]
- Gray HM, LaPlante DA, Bannon BL, Ambady N, Shaffer HJ. Development and validation of the alcohol identity implicit associations test (AI-IAT) Addictive Behaviors. 2011;36(9):919–926. doi: 10.1016/j.addbeh.2011.05.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Greenwald AG, McGhee DE, Schwartz JLK. Measuring individual differences in implicit cognition: The implicit association test. Journal of Personality and Social Psychology. 1998;74:1464–1480. doi: 10.1037//0022-3514.74.6.1464. [DOI] [PubMed] [Google Scholar]
- Gullo MJ, Dawe S, Kambouropoulos N, Staiger PK, Jackson CJ. Alcohol expectancies and drinking refusal self-efficacy mediate the association of impulsivity with alcohol misuse. Alcoholism: Clinical and Experimental Research. 2010;34:1386–1399. doi: 10.1111/j.1530-0277.2010.01222.x. [DOI] [PubMed] [Google Scholar]
- Hingson RW. Magnitude and prevention of college drinking and related problems. Alcohol Research & Health. 2010;33(1):45–54. [PMC free article] [PubMed] [Google Scholar]
- Hingson R, Heeren T, Winter M, Wechsler H. Magnitude of alcohol-related mortality and morbidity among U.S. college students ages 18-24: Changes from 1998 to 2001. Annual Review of Public Health. 2005;26:259–279. doi: 10.1146/annurev.publhealth.26.021304.144652. [DOI] [PubMed] [Google Scholar]
- Hoe SL. Issues and procedures in adopting structural equation modeling technique. Journal of Applied Quantative Methods. 2008;3:76–83. [Google Scholar]
- Hu LT, Bentler PM. Cut-off criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. [Google Scholar]
- Huchting K, Lac A, LaBrie JW. An application of the theory of planned behavior to sorority alcohol consumption. Addictive Behaviors. 2008;33(4):538–551. doi: 10.1016/j.addbeh.2007.11.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hulland J. Use of partial least squares (PLS) in strategic management research: A review of four recent studies. Strategic Management Journal. 1999;20:195–204. [Google Scholar]
- Johnston LD, O'Malley PM, Bachman JG, Schulenberg JE. Monitoring the future national survey results on drug use, 1975-2005 Volume II: College students and adults ages 19-45. Bethesda, MD: National Institute on Drug Abuse; 2006. NIH Publication No. 06-5884. [Google Scholar]
- Johnston LD, O'Malley PM, Bachman JG, Schulenberg JE. Monitoring the future national results on adolescent drug use: Overview of key findings, 2011. Bethesda, MD: National Institute on Drug Abuse; 2012. NIH Publication No. 12-5882. [Google Scholar]
- Kaysen D, Neighbors C, Martell J, Fossos N, Larimer ME. Incapacitated rape and alcohol use: A prospective analysis. Addictive Behaviors. 2006;31(10):1820–1832. doi: 10.1016/j.addbeh.2005.12.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kelloway EK. Assessing model fit. In: Kelloway EK, editor. Using LISREL for Structural Equation Modeling: A Researcher's Guide. Sage Publication, Inc.; Thousand Oaks, California: 1998. [Google Scholar]
- Kenny DA, Kashy DA, Bolger N. Data analysis in social psychology. In: Gilbert DT, Fiske ST, Lindzey G, editors. The handbook of social psychology. 4th. New York, NY: McGraw-Hill; 1998. pp. 233–265. [Google Scholar]
- Kivlahan DR, Marlatt GA, Fromme K, Coppel DB, Williams E. Secondary prevention with college drinkers: Evaluation of an alcohol skills training program. Journal of Consulting and Clinical Psychology. 1990;58:805–810. doi: 10.1037//0022-006x.58.6.805. [DOI] [PubMed] [Google Scholar]
- Kline RB. Principles and practice of structural equation modeling. 2nd. New York, NY: Guilford Press; 2005. [Google Scholar]
- Komro KA, Perry CL, Williams CL, Stigler MH, Farbakhsh K, Veblen-Mortenson S. How did Project Northland reduce alcohol use among adolescents? Analysis of mediating variables. Health Education Research. 2001;16:59–70. doi: 10.1093/her/16.1.59. [DOI] [PubMed] [Google Scholar]
- Koss MP, Gaines JA. The prediction of sexual aggression by alcohol use, athletic participation, and fraternity affiliation. Journal of Interpersonal Violence. 1993;8:94–108. [Google Scholar]
- Lalwani AK, Shavitt S. The “me” I claim to be: Cultural self-construal elicits self-presentational goal pursuit. Journal of Personality and Social Psychology. 2009;97(1):88–102. doi: 10.1037/a0014100. [DOI] [PubMed] [Google Scholar]
- Larimer ME, Lydum AR, Anderson BK, Turner AP. Male and female recipients of unwanted sexual contact in a college student sample: Prevalence rates, alcohol use, and depression symptoms. Sex Roles. 1999;40(3-4):295–308. [Google Scholar]
- Lee NK, Oei TS. The importance of alcohol expectancies and drinking refusal self-efficacy in the quantity and frequency of alcohol consumption. Journal of Substance Abuse. 1993;5(4):379–390. doi: 10.1016/0899-3289(93)90006-w. [DOI] [PubMed] [Google Scholar]
- Lemle R, Mishkind ME. Alcohol and masculinity. Journal of Substance Abuse Treatment. 1989;6(4):213–222. doi: 10.1016/0740-5472(89)90045-7. [DOI] [PubMed] [Google Scholar]
- Lindgren KP, Foster DW, Westgate EC, Neighbors C. Implicit drinking identity: Drinker + me associations predict college student drinking consistently. Addictive Behaviors. 2013;38(5):2163–2166. doi: 10.1016/j.addbeh.2013.01.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindgren KP, Neighbors C, Teachman BA, Wiers RW, Westgate E, Greenwald AG. I drink therefore I am: Validating alcohol-related implicit association tests. Psychology of Addictive Behaviors. 2013;27:1–13. doi: 10.1037/a0027640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Litt DM, Lewis MA, Stahlbrandt H, Firth P, Neighbors C. Social comparison as a moderator of the association between perceived norms and alcohol use and negative consequences among college students. Journal of Studies on Alcohol and Drugs. 2012;73(6):961–967. doi: 10.15288/jsad.2012.73.961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MacCallum RC, Austin JT. Applications of structural equation modeling in psychological research. Annual Review of Psychology. 2000;51:201–226. doi: 10.1146/annurev.psych.51.1.201. [DOI] [PubMed] [Google Scholar]
- MacKinnon DP. Introduction to structural mediation analysis. New York, NY: Lawrence Erlbaum; 2008. [Google Scholar]
- Mahalik JR, Good GE, Englar-Carlson M. Masculinity scripts, presenting concerns, and help seeking: Implications for practice and training. Professional Psychology: Research and Practice. 2003;34(2):123–131. [Google Scholar]
- Maisto SA, Connors GJ, Zywiak WH. Alcohol treatment changes in coping skills, self-efficacy, and levels of alcohol use and related problems 1 year following treatment initiation. Psychology of Addictive Behaviors. 2000;14:257–66. doi: 10.1037//0893-164x.14.3.257. [DOI] [PubMed] [Google Scholar]
- Malloy EA, Goldman M, Kington R. A call to action: Changing the culture of drinking at US colleges. National Institute on Alcohol Abuse and Alcoholism: Task Force of the National Advisory Council on Alcohol Abuse and Alcoholism; Washington, DC: 2002. [Google Scholar]
- McCreary DR, Newcomb MD, Sadave S. The male role, alcohol use, and alcohol problems. Journal of Counseling Psychology. 1999;46(1):109–124. [Google Scholar]
- Morawska AA, Oei TS. Binge drinking in university students: A test of the cognitive model. Addictive Behaviors. 2005;30(2):203–218. doi: 10.1016/j.addbeh.2004.05.011. [DOI] [PubMed] [Google Scholar]
- Neighbors C, Larimer ME, Geisner I, Knee C. Feeling controlled and drinking motives among college students: Contingent self-esteem as a mediator. Self and Identity. 2004;3(3):207–224. [Google Scholar]
- Nelson TF, Toomey TL, Lenk KM, Erickson DJ, Winters KC. Implementation of NIAAA college drinking task force recommendations: How are colleges doing 6 years later? Alcoholism: Clinical and Experimental Research. 2010;34(10):1687–1693. doi: 10.1111/j.1530-0277.2010.01268.x. [DOI] [PubMed] [Google Scholar]
- NIAAA. What colleges need to know now: An update on college drinking research. Bethesda, MD: National Institutes of Health, DHHS; 2007. NIH Publication No. 07-5010. [Google Scholar]
- Nock MK. Conceptual and design essentials for evaluating mechanisms of change. Alcoholism: Clinical and Experimental Research. 2007;31:4S–12S. doi: 10.1111/j.1530-0277.2007.00488.x. 3. [DOI] [PubMed] [Google Scholar]
- Oei TS, Jardim C. Alcohol expectancies, drinking refusal self-efficacy and drinking behaviour in Asian and Australian students. Drug and Alcohol Dependence. 2007;87(2-3):281–287. doi: 10.1016/j.drugalcdep.2006.08.019. [DOI] [PubMed] [Google Scholar]
- Oei TS, Morawska AA. A cognitive model of binge drinking: The influence of alcohol expectancies and drinking refusal self-efficacy. Addictive Behaviors. 2004;29:159–179. doi: 10.1016/s0306-4603(03)00076-5. [DOI] [PubMed] [Google Scholar]
- Perkins H. Gender patterns in consequences of collegiate alcohol abuse: A 10-yr study of trends in an undergraduate population. Journal of Studies on Alcohol. 1992;53(5):458–462. doi: 10.15288/jsa.1992.53.458. [DOI] [PubMed] [Google Scholar]
- Pierro A, Mannetti L, Livi S. Self-identity and the theory of planned behavior in the prediction of health behavior and leisure activity. Self and Identity. 2003;2(1):47–60. [Google Scholar]
- Reed MB, Wang R, Shillington AM, Clapp JD, Lange JE. The relationship between alcohol use and cigarette smoking in a sample of undergraduate college students. Addict Behaviors. 2007;32(3):449–464. doi: 10.1016/j.addbeh.2006.05.016. [DOI] [PubMed] [Google Scholar]
- SAMHSA. Screening on campus: Effective and available. U.S Department of Health and Human Services, Substance Abuse & Mental Health Services Administration; 2008. Retrieved from website: http://www.samhsa.gov/samhsa_news/volumexvi_2/article7.htm. [Google Scholar]
- Seo D, Li K. Effects of college climate on students' binge drinking: Hierarchical generalized linear model. Annals of Behavioral Medicine. 2009;38(3):262–268. doi: 10.1007/s12160-009-9150-3. [DOI] [PubMed] [Google Scholar]
- Shadel WG, Mermelstein R. Individual differences in self-concept among smokers attempting to quit: Validation and predictive utility of measures of the smoker self-concept and abstainer self-concept. Annals of Behavioral Medicine. 1996;18(3):151–156. doi: 10.1007/BF02883391. [DOI] [PubMed] [Google Scholar]
- Skutle A. The relationship among self-efficacy expectancies, severity of alcohol abuse, and psychological benefits from drinking. Addictive Behaviors. 1999;24:87–98. doi: 10.1016/s0306-4603(98)00007-0. [DOI] [PubMed] [Google Scholar]
- Slutske WS. Alcohol use disorders among US college students and their non-college-attending peers. Archives of General Psychiatry. 2005;62(3):321–327. doi: 10.1001/archpsyc.62.3.321. [DOI] [PubMed] [Google Scholar]
- Smith JR, Terry DJ, Manstead ASR, Louis WR, Kotterman D, Wolfs J. Interaction effects in the theory of planned behavior: The interplay of self-identity and past behavior. Journal of Applied Social Psychology. 2007;37(11):2726–2750. [Google Scholar]
- Solomon KE, Annis HM. Outcome and efficacy expectancy in the prediction of post-treatment drinking behavior. British Journal of Addiction. 1990;85:659–665. doi: 10.1111/j.1360-0443.1990.tb03528.x. [DOI] [PubMed] [Google Scholar]
- Steele CM. The psychology of self-affirmation: Sustaining the integrity of the self. In: Berkowitz L, editor. Advances in experimental social psychology. Vol. 21. San Diego, CA: Academic Press; 1988. pp. 261–302. [Google Scholar]
- Steiger JH. Structural model evaluation and modification: An interval estimation approach. Multivariate Behavorial Research. 1990;25:173–180. doi: 10.1207/s15327906mbr2502_4. [DOI] [PubMed] [Google Scholar]
- Wechsler H, Davenport A, Dowdall G, Moeykens B. Health and behavioral consequences of binge drinking in college: A national survey of students at 140 campuses. Journal of the American Medical Association. 1994;272(21):1672–1677. [PubMed] [Google Scholar]
- Wechsler H, Kuo M, Lee H, Dowdall GW. Environmental correlates of underage alcohol use and related problems of college students. American Journal of Preventive Medicine. 2000;19:24–29. doi: 10.1016/s0749-3797(00)00163-x. [DOI] [PubMed] [Google Scholar]
- Wiers RW, Eberl C, Rinck M, Becker ES, Lindenmeyer J. Retraining automatic action tendencies changes alcoholic patients' approach bias for alcohol and improves treatment outcome. Psychological Science. 2011;22:490–497. doi: 10.1177/0956797611400615. [DOI] [PubMed] [Google Scholar]
- Wells BE, Kelly BC, Golub SA, Grov C, Parsons JT. Patterns of alcohol consumption and sexual behavior among young adults in nightclubs. The American Journal of Drug and Alcohol Abuse. 2010;36(1):39–45. doi: 10.3109/00952990903544836. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Witkiewitz K, Donovan DM, Hartzler B. Drink refusal training as part of a combined behavioral intervention: Effectiveness and mechanisms of change. Journal Of Consulting And Clinical Psychology. 2012;80(3):440–449. doi: 10.1037/a0026996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Young RD, Connor JP, Ricciardelli LA, Saunders JB. The role of alcohol expectancy and drinking refusal self-efficacy beliefs in University student drinking. Alcohol and Alcoholism. 2006;41(1):70–75. doi: 10.1093/alcalc/agh237. [DOI] [PubMed] [Google Scholar]
- Young RM, Hasking PA, Oei TP, Loveday W. Validation of the Drinking Refusal Self-Efficacy Questionnaire—Revised in an adolescent sample (DRSEQ-RA) Addictive Behaviors. 2007;32:862–868. doi: 10.1016/j.addbeh.2006.07.001. [DOI] [PubMed] [Google Scholar]
- Young RM, Oei TPS. Drinking expectancy profile: Test manual. Behaviour Research and Therapy Centre, University of Queensland; Australia: 1996. [Google Scholar]
- Young RD, Oei TP, Crook GM. Differences in the perception of alcoholic versus non-alcoholic beverage advertisements. Psychologia: An International Journal of Psychology in the Orient. 1991;34(4):241–247. [Google Scholar]