

Abstract
Background: Patients admitted in coronary care units face various stressors. Ambiguity of future life conditions and unawareness of caring methods intensifies the patients’ anxiety and stress. This study was conducted to assess the effects of whole body massage on anxiety and vital signs of patients with acute coronary disorders.
Methods: A randomized controlled trial was conducted on 120 patients. Patients were randomly allocated into two groups. The intervention group received a session of whole body massage and the control group received routine care. The levels of State, Trait and overall anxiety and vital signs were assessed in both groups before and after intervention. Independent sample t-test, paired t-test, Chi-square and Fischer exact tests were used for data analysis.
Results: The baseline overall mean score of anxiety was 79.43±29.34 in the intervention group and was decreased to 50.38±20.35 after massage therapy (p=0.001). However, no significant changes were occurred in the overall mean anxiety in the control group during the study. The baseline diastolic blood pressure was 77.05±8.12 mmHg and was decreased to 72.18±9.19 mmHg after the intervention (p=0.004). Also, significant decreases were occurred in heart rate and respiration rate of intervention group after massage therapy (p=0.001). However, no significant changes were occurred in vital signs of the control group during the study.
Conclusion: The results suggest that whole body massage was effective in reducing anxiety and stabilizing vital signs of patients with acute coronary disorders.
Keywords: Massage therapy, Anxiety, Vital signs, Acute coronary disorder
Introduction
Patients admitted in coronary care units (CCU) face various worrying stressors (1). Almost 50% of patients having acute coronary syndrome (ACS) experience stress symptoms (2) in a way that one of the nursing diagnoses for these patients is anxiety (3). Moreover, ambiguity of future life conditions and unawareness of caring methods intensifies the patients’ stress.
Anxiety affects the function of all parts of the body, and in patients with acute myocardial infarction (AMI) it has more negative effects (4). Anxiety affecting nervous system, endocrine glands and immune system causes dysrhythmias, myocardial ischemia, heart failure, delirium, and delay in recovery of injuries and infections. Moreover, it increases the length of hospital stay and pain intensity and decreases the quality of life and sleep and finally may leads to death (5-7).
Factors such as pain, uncertainty, fear of death and long term disability are the reasons of worry and anxiety in hospitalized patients (8). It has also been reported that the patients in intensive care units and patients undergone heart surgery are very anxious (9).
Different methods have been applied to reduce anxiety and its consequences. Therapeutic touch and massage are of the oldest anxiolytic methods (10). Using massage therapy for accelerating wound healing has been recorded in old civilizations and is one of the most common treatments in the United States (11). Bray et al., reported that massage is advantageous for relaxation and pain reduction. However, it is recommended that more researches should be done about how to reduce anxiety in patients of critical and cardiac care units (12).
A recent study has reported that massage therapy reduces the pain and myofascial tension in patients with fibromyalgia and improves their mobility, physical functioning and quality of sleep (13). Another study has reported that back massage significantly reduced anxiety in patients with congestive heart failure. However this study did not use a control group (5). Several studies have also reported that massage therapy reduced anxiety of patients with scapulocostal syndrome (14), stroke (15), hand pain (16) and constipation (17). It has also been shown that massage therapy reduces pain and anxiety and improves sleep quality of patients undergone cardiovascular surgeries (18, 19, 9). However, these studies suffer some limitations such as small sample size and totally relying on patient-reported outcomes (18, 19). Studies have also reported that although massage may reduce chronic pain, it affects anxiety very briefly (13, 10). A recent study has also showed that massage therapy have no effect on anxiety in patients with breast cancer (20). Because of these inconsistencies, local application and short length of massage in some of previous studies, and lack of studies in patients with AMI and ACS, and because the heart rate and blood pressure can quickly be affected by anxiety, the present study aimed to investigate the effect of whole body massage on anxiety and vital signs of patients admitted in CCU wards of Kashan University of Medical Sciences (KAUMS) after acute coronary syndrome or acute myocardial infarction.
Methods
The study design
A randomized controlled trial was conducted with the permission of Kashan University of Medical Sciences. The study was done in two CCU wards of ShahidBeheshti hospital of Kashan, Iran.
The participants invited to the study after daily reviewing of the patients’ files of CCU wards and consulting with their physicians.
Sample Size
After a pilot study on 10 experimental and 10 control patients, and on the basis of the following formula the estimated number of samples for each group was estimated to be 52 patients (α= 0.05, 1-β=0.80, µ1-µ2= 4.84 and ). However 60 patients were selected for each group to compensate the possible attritions.
A convenience sample of the patients admitted in CCU (after ACS and AMI) was randomly allocated into 2 groups using a random number table(Fig. 1).
Fig. 1 .
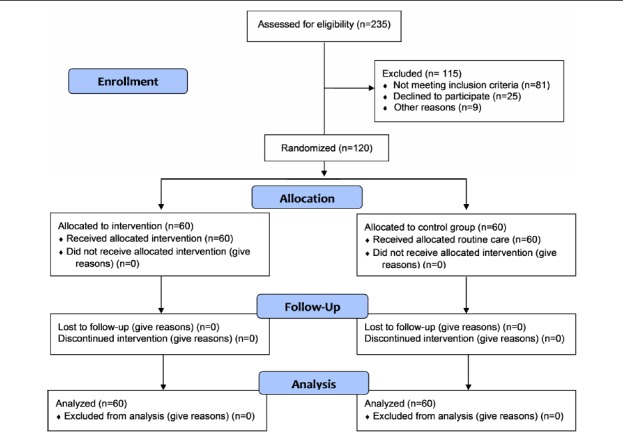
The trial Flow Diagram
Inclusion criteria
The criteria for inclusion were: male patients hospitalized in CCU, having a medical diagnosis of ACS or AMI, being literate, being conscious, a long of stay more than two days, and willing to participate in the study. Also not having the following conditions were selected as additional criteria, including: receiving warfarin, a cardiac arrest in the past 72 hours, severe dyspnea, fever, a cardiac pacemaker, a pulse rate less than 60/min, a history of second degree burn in more than 25% of the body surface, a known diabetes with autonomic neuropathy, a known mental disorder and infectious disease or hepatitis and jaundice, an amputated limb, a known adrenal gland and skin disorder, a diagnosed deep vein thrombosis, a dialysis fistula and a history of bone fracture in the past 2 months and a history of receiving massage therapy.
Exclusion criteria
The criteria for exclusion were: loss of consciousness, hemodynamic instability during the massage therapy session and refusing to complete the massage therapy session or decline to answer the study questionnaire.
Instruments
The data collection tool included two parts. The first part consisted of questions about demographic data (patient’s age, marital status, and job, number of children, education level, the patient’s medical diagnosis (AMI/ACS), and history of massage therapy. These data was gathered by interview and using patient’s file. There was a sheet for recording the patient’s vital signs (systolic and diastolic blood pressure, heart rate, and respiration rate) in two occasions. Blood pressures were measured from the left arm, using a mercury sphygmomanometer, after resting for 15 minutes lying on back. Instead of pulse rate, the patients’ heart rate was monitored on the patients monitor. Oral temperature was measured using an oral thermometer for 5 minutes. Respiration rate was also measured for one minute without patient’s notice. Vital signs were measured 30 minutes before and 15 minutes after the massage therapy (while the patients were resting). During massage therapy, the patients’ heart rhythm was also being monitored.
The Spielberger's State-Trait Anxiety Inventory (STAI) was used as the second part of the data collection tool and was answered by the patient. The STAI has two parts for measuring State and Trait anxiety. Each part has 20 items on a four-choice Likert scale. The state anxiety scale evaluate how respondents feel right now and is scored from ‘not at all’ to ‘very much’ (not at all=4, somewhat=3, moderately=2, and very much=1). In this part items number 3,4,6,7,9,12,13,14,17 and 18 were scored reversely.
The trait anxiety scale evaluate how respondents feel generally and is scored from ‘almost never’ to ‘almost always’ (almost never=4, sometimes=3, most of the time=2, and almost always=1). In this part items number 2,4,5,8,9,12,15,17,18 and 20 were scored reversely. The scores achieved from each parts of anxiety inventory varied from 20 to 80.
Mahram in 1994 has translated the STAI in Farsi and evaluated its reliability and validity. He has got reliability of 0.94 by Cronbach’s Alpha. For validity of the test the comparison of mean of anxiety of the standard community in all age ranges in two levels of 5% and 1% have been achieved. The Farsi inventory has been repeatedly used and evaluated among various groups and its validity and reliability have been measured (21, 22).
Intervention method
In the intervention group, massage therapy was done on the third day of hospitalization (when the acute phase of the disease is usually passed) after the physician’s permission and after the patient signed the informed consent form. All massage therapy sessions was done in a private room or after dropping the curtains around the patient.
For each participant in the intervention group, one session of massage therapy (for about 60 minutes) was done. For massage facilitation almond oil was used to massage back, shoulder deltoid muscles, front part of legs, arms, forearms, back of thighs, palms and fingers, metatarsus, front part of thighs, back of feet and toes, belly and chest, auxiliaries and neck muscles of the patient. Massage techniques used included static massage, surface tension techniques, stretching massage, superficial lymph unload, transverse friction techniques, and myofascial releasing techniques. (23)Immediately before and 30 minutes after the massage therapy, the anxiety level of the patient was measured. All the patients were examined and massaged in the evening shifts. All the massage therapy sessions was conducted by another researcher who had a special certificate in massage therapy or an assistant who has been trained and supervised by this researcher.
No intervention was done for the control group and they just received the routine care. The participants in this group also signed the informed consent form and their personal data and vital signs and anxiety was assessed first (as mentioned before) and after 105 minutes.
Ethical considerations
This study was approved by the Research Council and the Research Ethics Committee of Kashan University of Medical Sciences. The researchers also obtained permission from the hospital authorities. All of the subjects informed about being free to participate in the research, non-disclosure of personal information and were offered the written informed consent form to be signed before entering the study. The researchers were mindful of the need to pay close attention to ethical considerations and to the welfare of research participants.
Data analysis
Data analysis was performed usig SPSS 11.5 software. We used independent sample t-test for the comparisons between the mean scores of the two groups and paired t-test for within group comparisons. Chi-square and Fischer exact tests were also used for the comparisons between qualitative data. A P-value of less than 0.05 was considered to be significant.
Results
The mean age of the total cases was 57.60 (SD=14.48) years. Totally, 89.16% of the patients were married, 68.33% were employed and the others were retired or unemployed. The education of most of patients (58.33%) was at the level of primary school and the rest was at the level of secondary school or higher education. None of the patients had a history of massage therapy and the majority of the intervention group was completely or highly satisfied of massage therapy (Table 1).
Table 1 . Personal characteristics of the patients .
| Variables | Groups | p | ||
| Massage N(%) | Control N(%) | |||
| Age (Mean±SD) | 59.31±12.42 | 55.88±16.20 | 0.483 | |
| Medical diagnosis | ACS | 42 (70) | 47 (78.3) | 0. 404 |
| AMI | 18 (30) | 13 (21.7) | ||
| Level of education | Elementary | 36 (60) | 34 (56.7) | 0.711 |
| Secondary or higher | 24 (40) | 26 (43.3) | ||
| Marital status | Married | 54 (90) | 53 (88.3) | 0.768 |
| Single or widowed | 6 (10) | 7 (11.7) | ||
| Job | Employed | 42 (70) | 40 (66.7) | 0.694 |
| Retired/ unemployed | 18 (30) | 20 (33.3) | ||
| Previous hospitalization | Yes | 43 (71.7) | 39 (65) | 0.432 |
| No | 17 (28.3) | 21 (35) | ||
| Satisfaction of massage therapy | Completely | 39 (65) | --------- | |
| High | 18 (30) | |||
| Moderate | 3 (5) | |||
Before the massage therapy, the anxiety level and vital signs was investigated that there was no significant difference between the two groups (p>0.05) (Table 2 and 3). However, a significant decrease was observed in the state, trait and overall anxiety after the massage therapy session (p=0.001) (Table 2). There was also a decrease in level of all vital signs after the massage therapy session that was statistically significant for diastolic blood pressure, heart rate, and respiration rate (p<0.05) (Table 3).
Table 2 . Mean scores of state, trait and overall anxiety of the three groups before and after the intervention .
| Variable | Group | t-Test results | |||
| Massage | Control | 95% CI* | |||
|
State anxiety (Mean±SD) |
Before the intervention | 39.41±15.25 | 36.71±8.75 | -1.79 , 7.19 |
P= 0.237 T= 2.00 |
| After the intervention | 24.30±9.56 | 37.43±13.79 | -17.42 , -8.84 |
P= 0.001 T= -6.06 |
|
| P (paired t test) | 0.001 | 0.576 | - | ||
|
Trait anxiety (Mean±SD) |
Before the intervention |
40.01±14.92 | 35.31±10.98 | -0.03 , 9.43 |
P= 0.051 T= 1.96 |
| After the intervention | 26.08±11.08 | 35.33±11.60 | -13.35, -5.14 |
P= 0.001 T= -4.46 |
|
| P (paired t test) | 0.001 | 0.968 | - | ||
|
Overall anxiety (Mean±SD) |
Before the intervention |
79.43±29.34 | 72.03±18.72 | -1.49 , 16.29 |
P=0.102 T= 1.647 |
|
After the intervention |
50.38±20.35 | 72.76±21.80 | -30.00 ,-14.75 |
P=0.001 T= -5.813 |
|
| P (paired t test) | 0.001 | 0.613 | - | ||
CI= Confidence Interval of the Difference
Table 3 . Mean scores of state, trait and overall anxiety of the three groups before and after the intervention .
| Variable | Group | t-Test results | |||
| Massage | Control | 95% CI* | |||
| Systolic BP* (Mean±SD) | Before the intervention | 123.40±13.88 | 119.70±14.84 | -1.49 , 8.89 | P= 0.161 |
| T= 1.410 | |||||
| After the intervention | 120.51±14.50 | 123.83±17.18 | -9.06 , 2.43 | P= 0.25 | |
| T= -1.142 | |||||
| P (paired t test) | 0.242 | 0.147 | - | ||
| Diastolic BP* (Mean±SD) | Before the intervention | 77.05±8.12 | 75.36±9.82 | -1.57 , 4.94 | P= 0.30 |
| T= 1.022 | |||||
| After the intervention | 72.18±9.19 | 77.78±12.04 | -9.47 , -1.72 | P= 0.005 | |
| T= -2.862 | |||||
| P (paired t test) | 0.004 | 0.212 | - | ||
| Heart rate** (Mean±SD) | Before the intervention | 77.13±13.47 | 78.13±13.82 | -5.93 , 3.93 | P=0.68 |
| T= -0.401 | |||||
| After the intervention | 70.28±11.95 | 78.06±13.60 | -12.41 , -3.15 | P= 0.001 | |
| T= -3.329 | |||||
| P (paired t test) | 0.001 | 0.903 | - | ||
| Respiration rate** | Before the intervention | 19.53±4.40 | 18.51±4.69 | -0.63 , 2.66 | P=0. 0.22 |
| T= 1.223 | |||||
| After the intervention | 17.13±2.49 | 18.60±4.79 | -2.84 , -0.08 | P= 0.038 | |
| T= -2.103 | |||||
| P (paired t test) | 0.001 | 0.133 | |||
CI= Confidence Interval of the Difference, *Measures as mm hg, **per minutes
Discussion
The findings of this study showed that whole body massage reduces anxiety in patients admitted in CCU. This finding is consistent with the study published by Abolhasani who studied the effects of sensuous stimulation and back massage on anxiety in patients hospitalized in a coronary care unit (1). Massage seems to relax the muscles (14) and decreases nor-epinephrine (24) that consequently will result in reduced anxiety.
Our results showed that massage therapy reduces trait anxiety in patients admitted to CCU. Few studies have examined the effect of massage on trait anxiety. In a recent report it has reported that massage therapy after heart surgery may be pleasant but is not effective on trait anxiety (25). Another study has also reported that therapeutic touch did not significantly affect the trait anxiety of women undergoing cardiac catheterization (26). This result is inconsistent with our findings and may be attributed to short-term and local intervention. However, it seems that using whole body massage with a long duration was effective in achieving different results in the present study. The findings of this study showed that massage therapy reduces the overall anxiety score in patients admitted in CCU. Two other studies have also reported the same findings when they studied the effects of massage therapy on anxiety and tension of cardiac surgery (18) and stroke patients (15). Though, the difference between anxiety of intervention and control groups was not significant in the study conducted by Jouzi et al. (15). Previous studies have also shown that massage can relax muscles, produce calmness, reduces pain, fatigue and drowsiness and eventually leads to reduction of anxiety. In the present study, the difference between pre and post intervention mean scores of state, trait and overall anxiety and the difference between the mean scores of overall anxiety of the two groups were observed to be significant. These findings confirm the effect of massage therapy on the state, trait and overall anxiety in patients with coronary disorders.
Results of the present study showed that massage therapy have beneficial effects on vital signs of patients hospitalized in CCU by balancing systolic and diastolic blood pressures, heart rate and respiration rate. Some investigators found no significant effects of massage therapy on psychological responses (27, 28). However, findings of the present study are consistent with the studies conducted by Haji Hoseini et al., (29)Degirmen et al., (30)Lindgren et al., (31)and Shaban et al. (32). Illness and the threat of illness are usually accompanied by anxiety and stress. These emotional changes usually affect the patient’s physiological parameters such as vital signs (33). It has been shown that physiologic manifestations of anxiety are triggered by the sympathetic nervous system. It seems that massage may decrease the level of anxiety, which then would lower the levels of blood pressure, heart rate and respiratory rate (34,35). Additionally, it was hypothesized that massage changes the gradient pressure between the tissues and vessels that consequently facilitates the movement of liquids between tissues and vessels and vice versa. This process finally adjusts physiological parameters such as blood pressure (23). On the other hand, massage may distract the patient and consequently would reduce his anxiety (20). Then, it would finally decrease the blood pressure and heart rate. Also massage may induce a sense of comfort and relaxation and then endorphins may be secreted (35), vessels would be dilated, the blood flow increases within the superficial vessels of body (36) and blood pressure will be reduced. The reduction of heart rate after the massage may also be related to the anxiolytic and parasympatomimetic effects of massage (14, 31).
The observed alterations in the vital signs and anxiety level values can be important and advantageous for patients with AMI and ACS because these changes would reduce the myocardial oxygen demand. It can be recommended that massage therapy be used to balance the vital signs of patients admitted in CCU.
Conclusion
Based on the findings of the present study, massage therapy was effective in reducing anxiety, blood pressure, heart rate and respiration rate in male patients with ACS and AMI. Therefore we suggest that massage therapy be used as a complementary method to reduce the CCU patients’ anxiety and stabilize their vital signs.
Individual characteristics of the persons who performed the massage and wearing a white gown by the nurse may have affected the patients' anxiety levels. However, these factors were beyond the control of the researchers. In the present study the massage therapy was only performed in one session. We also did not consider the severity of myocardial infarction (MI) and angiography report. We also did not ask the patient about the exact reason of anxiety and measured the post massage anxiety and vital signs one time shortly after the massage therapy session. However, further research can be suggested with daily repeating of massage therapy, evaluation of anxiety and vital signs at more times after the massage therapy sessions, considering the exact reason of anxiety and also with considering the MI and angiography report. Then, the exact reason of anxiety and duration of the effects of massage therapy can be determined.
Acknowledgments
The researchers would like to express their gratitude to the directors and personnel of CCUs of ShahidBeheshti Hospital of the Kashan University of medical sciences. Also this study was supported by Kashan University of medical sciences with the project number of 9077. The registration number of this study is IRCT201112048296N1.
Cite this article as: Adib-Hajbaghery M, Abasi A, Rajabi-Beheshtabad R. Whole body massage for reducing anxiety and stabilizing vital signs of patients in cardiac care unit. Med J Islam Repub Iran 2014 (17 June). Vol. 28:47.
References
- 1.Abolhasani S. Effects of sensuous stimulation on anxiety in the patients hospitalized in coronary care unit. Sci J Kurdistan Univ Med Sci. 2007;12:44–52. [Google Scholar]
- 2.Huffman JC, Smith FA, Blais MA, Januzzi JL, Fricchione GL. Anxiety, independent of depressive symptoms, is associated with in-hospital cardiac complications after acute myocardial infarction. J Psychosom Res. 2008;65:557–563. doi: 10.1016/j.jpsychores.2008.08.001. [DOI] [PubMed] [Google Scholar]
- 3.McKinley S, Fien M, Riegel B, Meischke H, Aburuz ME, Lennie TA, Moser DK. Complications after acute coronary syndrome are reduced by perceived control of cardiac illness. J Adv Nurs. 2012;68:2320–30. doi: 10.1111/j.1365-2648.2011.05933.x. [DOI] [PubMed] [Google Scholar]
- 4.Arora D, Anand M, Katyal VK, Anand V. Anxiety and well-being among acute coronary syndrome patients: overtime. J Indian Acad Appl Psychol. 2010;36:79–88. [Google Scholar]
- 5.Chen W, Liu G, Yeh S, Chiang M, Fu M, Hsieh Y. Effect of back massage intervention on anxiety, comfort, and physiologic responses in patients with congestive heart failure. J Alterna Complement Med. 2013;19:464–70. doi: 10.1089/acm.2011.0873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Abu Ruz ME, Lennie TA, Moser DK. Effects of β-blockers and anxiety on complication rates after acute myocardial infarction. Am J Crit Care. 2011;20:67–73. doi: 10.4037/ajcc2010216. [DOI] [PubMed] [Google Scholar]
- 7.Pedersen SS, Van Domburg RT, Larsen ML. The effect of low social support on short-term prognosis in patients following a first myocardial infarction. Scand J Psychol. 2004;45:313–318. doi: 10.1111/j.1467-9450.2004.00410.x. [DOI] [PubMed] [Google Scholar]
- 8.Dogar IA, Khawaja IS, Azeem MW, Awan H, Ayub A, Iqbal J, Thuras P. Prevalence and Risk Factors for Depression and Anxiety in Hospitalized Cardiac Patients in Pakistan. Psychiatry (Edgmont) 2008;5:38–41. [PMC free article] [PubMed] [Google Scholar]
- 9.AdibHajbaghery M, Moradi T, Mohseni R. Effects of a Multimodal Preparation Package on Vital Signs of Patients Waiting for Coronary Angiography. Nurs Midwifery Stud. 2014;3:E17518. doi: 10.17795/nmsjournal17518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Sherman KJ, Cherkin DC, Kahn J, Erro J, Hrbek A, Deyo RA. et al. A survey of training and practice patterns of massage therapists in two US states. BMC complement altern med. 2005;14:13. doi: 10.1186/1472-6882-5-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: United States, 2007. National Health Statistics Reports. 2008;12:1–23. [PubMed] [Google Scholar]
- 12.Bray K, Hill K, Robson W, Leaver G, Walker N, O'Leary M. et al. British Association of Critical Care Nurses Position statement on the use of restraint in adult critical care units. Nurs Crit Care. 2004;9:199–212. doi: 10.1111/j.1362-1017.2004.00074.x. [DOI] [PubMed] [Google Scholar]
- 13.Castro-Sanchez AM, Mataran-Penarrocha GA, Granero-Molina J, Aguilera-Manrique G, Quesada-Rubio JM, Moreno-Lorenzo C. Benefits of massage-myofascial release therapy on pain, anxiety, quality of sleep, depression, and quality of life in patients with fibromyalgia. Evid-Based Complement Altern Med. 2011;2011:561753. doi: 10.1155/2011/561753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Buttagat V, Eungpinichpong W, Chatchawan U, Kharmwan S. The immediate effects of traditional Thai massage on heart rate variability and stress related parameters in patients with back painassociated with myofascial trigger points. Journal of Bodyw Mov Ther. 2011;15:15–23. doi: 10.1016/j.jbmt.2009.06.005. [DOI] [PubMed] [Google Scholar]
- 15.Jouzi M. Assessment of the effect of massage therapy on stroke patients. Med Sci J Islamic Azad Univ, Tehran Med Branch. 2009;19:256–261. [Google Scholar]
- 16.Field T, Diego M, Delgado J, Garcia D, Funk CG. Hand pain is reduced by massage therapy. Complement Ther Clin Pract. 2011;17:226–229. doi: 10.1016/j.ctcp.2011.02.006. [DOI] [PubMed] [Google Scholar]
- 17.Sinclair M. The use of abdominal massage to treat chronic constipation. J Bodyw Mov Ther. 2011;15:436–445. doi: 10.1016/j.jbmt.2010.07.007. [DOI] [PubMed] [Google Scholar]
- 18.Cutshall SM, Wentworth LJ, Engen D, Sundt TM, Kelly RF, Bauer B. A Effect of massage therapy on pain, anxiety, and tension in cardiac surgical patients: a pilot study. Complement Ther Clin Pract. 2010;16:92–95. doi: 10.1016/j.ctcp.2009.10.006. [DOI] [PubMed] [Google Scholar]
- 19.Nerbass FB, Feltrim MIZ, Souza SAd, Ykeda DS, Lorenzi-Filho G. Effects of massage therapy on sleep quality after coronary artery bypass graft surgery. Clinics. 2010;65:1105–1110. doi: 10.1590/S1807-59322010001100008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Billhult A, Lindholm C, Gunnarsson R, Stener-Victorin E. The effect of massage on cellular immunity, endocrine and psychological factors in women with breast cancer- A randomized controlled clinical trial. Auton Neurosci. 2008;140:88–95. doi: 10.1016/j.autneu.2008.03.006. [DOI] [PubMed] [Google Scholar]
- 21.Dehghan-nayeri N, Adib-Hajbaghery M. Effects of progressive relaxation on anxiety and quality of life in female students: A non-randomized controlled trial. Complement Ther Med. 2011;19:194–200. doi: 10.1016/j.ctim.2011.06.002. [DOI] [PubMed] [Google Scholar]
- 22. Mahram B. Standardization of Spielberger’s test anxiety inventory in Mashhad. Allameh Tabatabaei University, Tehran. 1994.
- 23. Shiri M. Massage therapy (2nded.). Tehran: Aeeizh. 2010.
- 24. Braun MB, Simonson S. Introduction to Massage Therapy (3rded.). Philadelphia: LWW. 2014.
- 25.Baxter GD, Albert NM. Massage therapy after heart surgery: possibly pleasant, but not effective. Focus Altern Complement Ther. 2011;16(1):76–77. [Google Scholar]
- 26.Zolfaghari M, Eybpoosh S, Hazrati M. Effects of therapeutic touch on anxiety, vital signs, and cardiac dysrhythmia in a sample of Iranian women undergoing cardiac catheterization: a quasi-experimental study. J Holistic Nurs. 2012;30(4):225–234. doi: 10.1177/0898010112453325. [DOI] [PubMed] [Google Scholar]
- 27.Cowen VS, Burkett L, Bredimus J, Evans DR, Lamey S, Neuhauser T. et al. A comparative study of Thai massage and Swedish massage relative to physiological and psychological measures. J Bodywork Movement Ther. 2006;10:266–75. [Google Scholar]
- 28.Combron JA, Dexheimer J, Coe P. Changes in blood pressure after various forms of therapeutic massage: A preliminary study. J Altern Complement Med. 2006;12:65–70. doi: 10.1089/acm.2006.12.65. [DOI] [PubMed] [Google Scholar]
- 29.Haji Hoseini F, Avazeh A, Elahi N, Shariati A, Sori H. The effect of massage on comatos patients' vital signs, hospitalized in intensive care units. J Arak Univ Med Sci. 2006;3:1–10. [Google Scholar]
- 30.Degirmen N, Ozerdogan N, Sayiner D, Kosgeroglu N, Ayranci U. Effectiveness of foot and hand massage in post cesarean pain control in a group of Turkish pregnant women. Appl Nurs Res. 2010;23:153–158. doi: 10.1016/j.apnr.2008.08.001. [DOI] [PubMed] [Google Scholar]
- 31.Lindgren L, Rundgren S, Winsö O, Lehtipalo S, Wiklund U, Karlsson M. et al. Physiological responses to touch massage in healthy volunteers. Auton neurosci. 2010;158:105–110. doi: 10.1016/j.autneu.2010.06.011. [DOI] [PubMed] [Google Scholar]
- 32.Shaban M, Haji Amiry P, Mehran A, Kahrary S. Evaluation of immediate effect of foot massage on patient’s vital signs in a general intensive care unit. Hayat. 2004;10:71–80. [Google Scholar]
- 33. Smeltzer S, Bare BG, Hinkle JL, Cheever KH. Brunner and Suddarth's Textbook of Medical-Surgical Nursing. Philadelphia: Lippincott Williams & Wilkins. 2010.
- 34.Çinar Ş, Eser I, Khorshid L. The effects of back massage on the vital signs and anxiety level of elderly staying in a rest home. Hacettepe Univ Faculty of Health Sci Nurs J. 2009;16:14–21. [Google Scholar]
- 35. Tamparo CD, Lewis MA. Diseases of the Human Body (Diseases of the Human Body (5thed.). Philadelphia: F.A. Davis Co. 2011.
- 36. Eungpinichpong W. Therapeutic Thai Massage. Bangkok: Chonromdek Publishing House. 2008.