

Abstract
Background: There is substantial lack of knowledge about the role of socioeconomic status (SES) indicators on life expectancy (LE) within-cities, especially within mega-cities. We aimed to investigate the disparities of LE within city districts of Tehran, Iran, and specify how SES inequalities play role on LE.
Methods: The death and population data for 2010 by different age, gender, and residency district were obtained from the main cemetery of Tehran and statistical centre of Iran, respectively. Age-specific mortality rates and consequently LE were calculated for all 22 districts by different genders. Finally, based on the results of first Tehran's Urban Health Equity Assessment and Response Tool (Urban HEART) project in 2008, the influence of social classes (SCs), total costs, and education indicators were analyzed on LE at birth (e0).
Results: The e0 for total males and females in Tehran were calculated as 74.6 and 78.4 years for 2010, respectively. The maximum LE of 80 years was observed in females of northern part with higher SES, and the minimum e0 of 72.7 years observed in males of southern part with lower SES. The e0 gender gap among districts was 5.5 years for females and 3.7 years for males. The highest and lowest mean of e0 observed in SC1 (highest class) and SC5 (lowest class), were 77.6 and 76.0 years, respectively. The lowest mean of e0 observed in the first group of total costs indicator and was 76.2 years. In addition, the lowest observed mean of e0 was in the first category of education indicator (illiterate) and was 76.0 years.
Conclusion: Results indicate substantial disparities in LE within city districts. This confirms that SES disparities within-cities would have direct influences on LE.
Keywords: Disparities, Education level, Expenditure, Inequality, Iran, Life expectancy, Longevity, Social class, Socioeconomic situation (SES), Tehran, Urban HEART, Within-city health metrics
Introduction
According to world health report 2000, disability-adjusted life expectancy (LE) at birth in Iran for 1999 was 60.5 years, and Iran had a rank of 96 among 191 member states of World Health Organization (WHO) (1). This was upgraded, moreover, to 71.56 years in 2003 (2), and in the most recent report, life expectancy at birth increased to 73 years in 2009 (3).
Generally, there are considerable credible literatures that report influence of socioeconomic measures on LE (4-8). In brief, little association has been reported between LE and gross national product (GNP) among rich countries of the world (4). However, a potent relationship between socioeconomic status (SES) of the households and children mortality rates, exist within the country in which mortality rates increase gradually in households with lower SES (4, 9). In addition, education level has an inverse relation with mortality rates. For example, mortality rates have been reported to be less in well educated people of every parts of the world either developing or developed countries (9-13), where indicates the LE gap within educational groups is still rising to the extent that educational differentials may depict 30% of changes in LE (12). Nevertheless, albeit there is large body of literature in global- and national-scale on the influence of SES disparities on LE, considerable lack of knowledge exist on how SES factors play role on LE within-cities, especially within mega-cities.
In this study, the authors aimed a) to investigate the disparities of LE within 22 city-districts of Tehran, Iran, and b) to analyze the influence of SES disparities on LE within city-districts.
Methods
Study area
Tehran, the capital of Iran, is the largest and most populated city of the country. The population at the time of study was about 8.2 million people (14). The city has a large area of about 613 km2, and divided administratively into 22 districts (15). The structure of the city is diverse in which socioeconomic situation of northern households are higher than southern parts.
LE calculations
In this analytic-descriptive study, we used census method to estimate LE within city districts. The main cemetery of Tehran, Behesht-e-Zahra which provides necessary service for family of deceased people is officially under subsidiary of Tehran Municipality where all death data are recorded. Thus, the number of deaths in 2010 obtained from this cemetery was based on age, gender, and residency district (16). The population data were also derived from the statistical centre of Iran by the same catagories (14). Age-specific mortality rates, thereafter, were calculated for all 22 districts of Tehran by different genders. Based on the age-specific mortality rates, the estimated LE for all Tehran's districts through various gender and age groups, were at birth or <1 year-old, 1-4, 5-9,…, 75-79, and >80 years-old. To estimate life tables we used MORTPAK 4 software—The United Nations Software Package for Mortality Measurements—with 17 different applications, using "COPMAR" and "MATCH" applications to estimate the LE (17). After determining the LE for all 22 districts, we plotted the results using geographic information system (GIS) to visualize the distribution of LE over the city districts.
Socioeconomic measures
In order to determine the influence of socioeconomic measures on LE within city districts, results of the first Tehran's Urban Health Equity Assessment and Response Tool (Urban HEART-1) project in 2008 were extracted (18). Briefly, the Tehran's Urban HEART project evaluated 42 indicators in six principal policy domains including “Physical and Infra-structure,” “Human and Social Development,” “Economic,” “Governance,” “Health” and “Nutrition” to quantify socioeconomic inequalities in a large population-based survey within Tehran megacity. In the current study, three indicators, namely “Socioeconomic Status (SES)” according to job, “Total Costs” (non-food), and “Education” were extracted and analyzed to explore the relationship with LE (18).
Social classes were determined according to the household head’s occupation, and are summarized into six social classes (SCs).
Total Costs was a single quantitative variable, derived from a series of detailed questions regarding every aspect of household expenditures reported by the family head, which were finally categorized into five quintiles that represent 20 percent of total data for each category.
Education was categorized into five groups including “Illiterate,” “Primary,” “High-school and Diploma,” “Bachelor of Science (BSc) and under” and “Master of Science (MSc) and Higher.”
Statistical analyses
Kolmogorov-Smirnov test was used to test the normality of LE. Descriptive statistics were applied to SES, total costs, and education indicators. Levene's test was used to investigate the homogeneity (equality) of variances between sub-groups. Since the variances among the sub-groups were not equal, hence non-parametric tests were used. Moreover Kruskal-Wallis test was used to test differences between sub-groups and post-hoc test used for pairwise multiple comparisons between sub-groups.
Results
LE
The LE for total males and females in Tehran were calculated as 74.6 and 78.4 years for 2010, respectively (p< 0.001). The maximum LE of 80 years was observed in females of northern part (1, 4, and 5 districts) with higher socioeconomic status, and the minimum LE of 72.7 years observed in males of southern part (district 9) with lower socioeconomic status, and with a gap of 7.3 years (Fig. 1). The maximum and minimum observed LE for males in districts of northern (district 1) and southern part (district 9), were 78.2 and 72.7 years, respectively. The maximum LE for females estimated as 80 years in districts of northern part (districts of 1, 4, and 5), while the minimum was 76.3 years in district 9 in southern part. The LE gender gap among districts was 5.5 years for females and 3.7 for males. Regardless of gender difference, the maximum and minimum LEs observed in districts of northern (district 1) and southern part (district 9), were 79.1 and 74.5, respectively.
Fig. 1 .
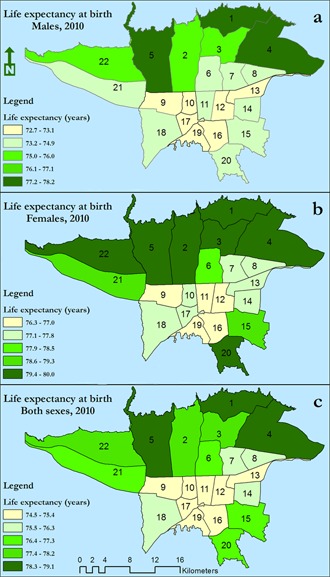
Estimated distribution of life expectancy at birth for a) males, b) females and c) both genders in 22 districts of Tehran, Iran, 2010.
Table 1 shows LE at birth in all 22 districts of Tehran in both genders. Also, Tables 2 and 3 show LE of aforementioned age groups by different genders in all 22 districts of Tehran. Moreover,Fig. 1 illustrates the geographic distribution of LE in all 22 districts of Tehran megacity by various genders. Descriptive statistics of SES, education, and total costs indicators, also, are shown in Table 4.
Table 1 . Life expectancy at birth within Tehran megacity by different districts, genders and geographic location .
| District | Males | Females |
Both genders |
Geographical location |
| 1 | 78.2 | 80.0 | 79.1 | North |
| 2 | 75.9 | 79.6 | 77.7 | North |
| 3 | 75.9 | 79.5 | 77.7 | North |
| 4 | 78.0 | 80.0 | 79.0 | North |
| 5 | 77.8 | 80.0 | 78.9 | North |
| 6 | 74.7 | 78.4 | 76.5 | South |
| 7 | 74.2 | 77.7 | 75.9 | South |
| 8 | 74.0 | 77.3 | 75.6 | West |
| 9 | 72.7 | 76.3 | 74.5 | South |
| 10 | 73.1 | 77.1 | 75.1 | South |
| 11 | 73.7 | 77.0 | 75.3 | South |
| 12 | 72.8 | 76.7 | 74.7 | South |
| 13 | 73.1 | 77.7 | 75.4 | West |
| 14 | 74.3 | 77.6 | 75.9 | West |
| 15 | 74.7 | 78.6 | 76.6 | South |
| 16 | 72.9 | 76.4 | 74.6 | South |
| 17 | 72.8 | 77.2 | 75.0 | South |
| 18 | 74.0 | 77.5 | 75.7 | South |
| 19 | 73.0 | 76.8 | 74.9 | South |
| 20 | 74.0 | 79.9 | 76.9 | South |
| 21 | 74.0 | 79.1 | 76.5 | East |
| 22 | 75.6 | 79.7 | 77.6 | East |
| Total | 74.6 | 78.4 | 76.5 | - |
Table 2 . Life expectancy of males in Tehran megacity by different districts and age-groups in 2010 .
| Age group / District | 1_4 | 5_9 | 10_14 | 15_19 | 20_24 | 25_29 | 30_34 | 35_39 | 40_44 | 45_49 | 50_54 | 55_59 | 60_64 | 65_69 | 70_74 | 75_79 | 80< |
| 1 | 77.54 | 73.55 | 68.57 | 63.59 | 58.64 | 53.70 | 48.76 | 43.82 | 38.89 | 34.00 | 29.22 | 24.65 | 20.38 | 16.41 | 12.77 | 9.64 | 7.11 |
| 2 | 75.58 | 71.62 | 66.65 | 61.69 | 56.77 | 51.89 | 47.00 | 42.10 | 37.23 | 32.40 | 27.72 | 23.29 | 19.17 | 15.37 | 11.92 | 8.99 | 6.65 |
| 3 | 75.58 | 71.62 | 66.65 | 61.69 | 56.77 | 51.89 | 47.00 | 42.10 | 37.23 | 32.40 | 27.72 | 23.29 | 19.17 | 15.37 | 11.92 | 8.99 | 6.65 |
| 4 | 77.37 | 73.38 | 68.39 | 63.41 | 58.47 | 53.54 | 48.60 | 43.67 | 38.74 | 33.86 | 29.08 | 24.52 | 20.27 | 16.31 | 12.69 | 9.58 | 7.07 |
| 5 | 77.19 | 73.21 | 68.22 | 63.24 | 58.30 | 53.37 | 48.44 | 43.51 | 38.59 | 33.71 | 28.94 | 24.40 | 20.15 | 16.21 | 12.61 | 9.51 | 7.02 |
| 6 | 74.61 | 70.67 | 65.71 | 60.76 | 55.88 | 51.02 | 46.16 | 41.30 | 36.45 | 31.67 | 27.04 | 22.67 | 18.63 | 14.92 | 11.55 | 8.70 | 6.44 |
| 7 | 74.21 | 70.29 | 65.33 | 60.39 | 55.52 | 50.68 | 45.83 | 40.98 | 36.14 | 31.38 | 26.77 | 22.43 | 18.42 | 14.74 | 11.41 | 8.60 | 6.36 |
| 8 | 74.06 | 70.14 | 65.19 | 60.25 | 55.38 | 50.54 | 45.70 | 40.85 | 36.02 | 31.27 | 26.67 | 22.34 | 18.34 | 14.67 | 11.36 | 8.55 | 6.33 |
| 9 | 73.06 | 69.18 | 64.25 | 59.33 | 54.49 | 49.69 | 44.88 | 40.07 | 35.29 | 30.58 | 26.04 | 21.78 | 17.86 | 14.26 | 11.03 | 8.30 | 6.15 |
| 10 | 73.37 | 69.47 | 64.53 | 59.61 | 54.75 | 49.95 | 45.13 | 40.31 | 35.51 | 30.78 | 26.22 | 21.95 | 18.00 | 14.38 | 11.12 | 8.37 | 6.21 |
| 11 | 73.83 | 69.91 | 64.97 | 60.03 | 55.17 | 50.34 | 45.51 | 40.67 | 35.85 | 31.10 | 26.52 | 22.21 | 18.23 | 14.57 | 11.28 | 8.49 | 6.29 |
| 12 | 73.14 | 69.25 | 64.32 | 59.40 | 54.55 | 49.76 | 44.95 | 40.13 | 35.34 | 30.63 | 26.08 | 21.82 | 17.89 | 14.29 | 11.05 | 8.32 | 6.17 |
| 13 | 73.37 | 69.47 | 64.53 | 59.61 | 54.75 | 49.95 | 45.13 | 40.31 | 35.51 | 30.78 | 26.22 | 21.95 | 18.00 | 14.38 | 11.12 | 8.37 | 6.21 |
| 14 | 74.29 | 70.36 | 65.41 | 60.47 | 55.59 | 50.75 | 45.89 | 41.04 | 36.20 | 31.44 | 26.82 | 22.48 | 18.47 | 14.78 | 11.44 | 8.62 | 6.38 |
| 15 | 74.61 | 70.67 | 65.71 | 60.76 | 55.88 | 51.02 | 46.16 | 41.30 | 36.45 | 31.67 | 27.04 | 22.67 | 18.63 | 14.92 | 11.55 | 8.70 | 6.44 |
| 16 | 73.21 | 69.33 | 64.39 | 59.47 | 54.62 | 49.82 | 45.01 | 40.19 | 35.40 | 30.68 | 26.13 | 21.86 | 17.93 | 14.32 | 11.07 | 8.34 | 6.18 |
| 17 | 73.14 | 69.25 | 64.32 | 59.40 | 54.55 | 49.76 | 44.95 | 40.13 | 35.34 | 30.63 | 26.08 | 21.82 | 17.89 | 14.29 | 11.05 | 8.32 | 6.17 |
| 18 | 74.06 | 70.14 | 65.19 | 60.25 | 55.38 | 50.54 | 45.70 | 40.85 | 36.02 | 31.27 | 26.67 | 22.34 | 18.34 | 14.67 | 11.36 | 8.55 | 6.33 |
| 19 | 73.29 | 69.40 | 64.46 | 59.54 | 54.69 | 49.88 | 45.07 | 40.25 | 35.45 | 30.73 | 26.18 | 21.90 | 17.96 | 14.35 | 11.10 | 8.36 | 6.19 |
| 20 | 74.06 | 70.14 | 65.19 | 60.25 | 55.38 | 50.54 | 45.70 | 40.85 | 36.02 | 31.27 | 26.67 | 22.34 | 18.34 | 14.67 | 11.36 | 8.55 | 6.33 |
| 21 | 74.06 | 70.14 | 65.19 | 60.25 | 55.38 | 50.54 | 45.70 | 40.85 | 36.02 | 31.27 | 26.67 | 22.34 | 18.34 | 14.67 | 11.36 | 8.55 | 6.33 |
| 22 | 75.33 | 71.38 | 66.41 | 61.45 | 56.55 | 51.67 | 46.78 | 41.90 | 37.03 | 32.21 | 27.54 | 23.13 | 19.03 | 15.26 | 11.83 | 8.91 | 6.59 |
| Total | 74.53 | 70.59 | 65.63 | 60.69 | 55.80 | 50.95 | 46.09 | 41.23 | 36.39 | 31.61 | 26.98 | 22.62 | 18.59 | 14.88 | 11.53 | 8.68 | 6.43 |
Table 3 . Life expectancy of females in Tehran megacity by different districts and age-groups in 2010 .
| Age group / District | 1_4 | 5_9 | 10_14 | 15_19 | 20_24 | 25_29 | 30_34 | 35_39 | 40_44 | 45_49 | 50_54 | 55_59 | 60_64 | 65_69 | 70_74 | 75_79 | 80< |
| 1 | 79.57 | 75.60 | 70.62 | 65.63 | 60.66 | 55.69 | 50.73 | 45.78 | 40.86 | 35.97 | 31.18 | 26.49 | 21.90 | 17.50 | 13.42 | 9.87 | 6.98 |
| 2 | 79.23 | 75.27 | 70.29 | 65.31 | 60.34 | 55.38 | 50.42 | 45.48 | 40.56 | 35.69 | 30.91 | 26.24 | 21.67 | 17.30 | 13.26 | 9.76 | 6.91 |
| 3 | 79.15 | 75.19 | 70.21 | 65.23 | 60.26 | 55.30 | 50.35 | 45.41 | 40.49 | 35.62 | 30.85 | 26.18 | 21.62 | 17.25 | 13.22 | 9.73 | 6.89 |
| 4 | 79.57 | 75.60 | 70.62 | 65.63 | 60.66 | 55.69 | 50.73 | 45.78 | 40.86 | 35.97 | 31.18 | 26.49 | 21.90 | 17.50 | 13.42 | 9.87 | 6.98 |
| 5 | 79.57 | 75.60 | 70.62 | 65.63 | 60.66 | 55.69 | 50.73 | 45.78 | 40.86 | 35.97 | 31.18 | 26.49 | 21.90 | 17.50 | 13.42 | 9.87 | 6.98 |
| 6 | 78.26 | 74.32 | 69.35 | 64.38 | 59.42 | 54.48 | 49.54 | 44.62 | 39.73 | 34.89 | 30.16 | 25.54 | 21.04 | 16.75 | 12.82 | 9.43 | 6.70 |
| 7 | 77.70 | 73.78 | 68.82 | 63.85 | 58.90 | 53.97 | 49.05 | 44.14 | 39.27 | 34.46 | 29.75 | 25.16 | 20.70 | 16.46 | 12.58 | 9.26 | 6.59 |
| 8 | 77.38 | 73.48 | 68.52 | 63.56 | 58.61 | 53.69 | 48.77 | 43.88 | 39.02 | 34.21 | 29.52 | 24.95 | 20.51 | 16.30 | 12.45 | 9.17 | 6.53 |
| 9 | 76.61 | 72.74 | 67.80 | 62.84 | 57.92 | 53.01 | 48.12 | 43.24 | 38.41 | 33.64 | 28.98 | 24.46 | 20.07 | 15.92 | 12.15 | 8.95 | 6.39 |
| 10 | 77.23 | 73.33 | 68.38 | 63.41 | 58.47 | 53.55 | 48.64 | 43.75 | 38.89 | 34.10 | 29.41 | 24.85 | 20.42 | 16.22 | 12.39 | 9.12 | 6.50 |
| 11 | 77.15 | 73.26 | 68.30 | 63.34 | 58.40 | 53.48 | 48.57 | 43.68 | 38.83 | 34.04 | 29.35 | 24.80 | 20.38 | 16.18 | 12.36 | 9.10 | 6.48 |
| 12 | 76.92 | 73.04 | 68.08 | 63.13 | 58.19 | 53.28 | 48.38 | 43.49 | 38.65 | 33.86 | 29.19 | 24.65 | 20.24 | 16.07 | 12.27 | 9.03 | 6.44 |
| 13 | 77.70 | 73.78 | 68.82 | 63.85 | 58.90 | 53.97 | 49.05 | 44.14 | 39.27 | 34.46 | 29.75 | 25.16 | 20.70 | 16.46 | 12.58 | 9.26 | 6.59 |
| 14 | 77.62 | 73.71 | 68.74 | 63.78 | 58.83 | 53.90 | 48.98 | 44.07 | 39.21 | 34.39 | 29.69 | 25.11 | 20.65 | 16.42 | 12.55 | 9.24 | 6.57 |
| 15 | 78.42 | 74.48 | 69.50 | 64.53 | 59.57 | 54.62 | 49.68 | 44.76 | 39.86 | 35.02 | 30.28 | 25.65 | 21.14 | 16.84 | 12.89 | 9.48 | 6.73 |
| 16 | 76.69 | 72.82 | 67.87 | 62.91 | 57.98 | 53.08 | 48.18 | 43.30 | 38.47 | 33.69 | 29.03 | 24.50 | 20.11 | 15.96 | 12.18 | 8.97 | 6.40 |
| 17 | 77.31 | 73.41 | 68.45 | 63.49 | 58.54 | 53.62 | 48.71 | 43.81 | 38.95 | 34.15 | 29.46 | 24.90 | 20.47 | 16.26 | 12.42 | 9.14 | 6.51 |
| 18 | 77.54 | 73.63 | 68.67 | 63.70 | 58.76 | 53.83 | 48.91 | 44.01 | 39.14 | 34.33 | 29.63 | 25.05 | 20.60 | 16.38 | 12.52 | 9.21 | 6.56 |
| 19 | 76.99 | 73.11 | 68.16 | 63.20 | 58.26 | 53.35 | 48.44 | 43.56 | 38.71 | 33.92 | 29.25 | 24.70 | 20.29 | 16.11 | 12.30 | 9.05 | 6.46 |
| 20 | 79.48 | 75.52 | 70.53 | 65.55 | 60.58 | 55.61 | 50.65 | 45.71 | 40.78 | 35.90 | 31.11 | 26.42 | 21.84 | 17.45 | 13.38 | 9.84 | 6.97 |
| 21 | 78.82 | 74.87 | 69.89 | 64.92 | 59.95 | 55.00 | 50.05 | 45.11 | 40.21 | 35.35 | 30.59 | 25.94 | 21.40 | 17.06 | 13.07 | 9.62 | 6.82 |
| 22 | 79.32 | 75.35 | 70.37 | 65.39 | 60.42 | 55.46 | 50.50 | 45.56 | 40.64 | 35.76 | 30.98 | 26.30 | 21.73 | 17.35 | 13.30 | 9.79 | 6.93 |
| Total | 78.26 | 74.32 | 69.35 | 64.38 | 59.42 | 54.48 | 49.54 | 44.62 | 39.73 | 34.89 | 30.16 | 25.54 | 21.04 | 16.75 | 12.82 | 9.43 | 6.70 |
Table 4 . Ecological relationship between life expectancy and social classes, level of education, and family expenditures .
| Main variable | Subgroups | Mean (SD) | p-value |
| Social class | SC-1 | 77.19 (1.42) | <0.001 |
| SC-2 | 76.74 (1.50) | ||
| SC-3a | 76.51 (1.50) | ||
| SC-3b | 76.28 (1.44) | ||
| SC-4 | 76.32 (1.45) | ||
| SC-5 | 76.05 (1.36) | ||
| Total | 76.48 (1.47) | ||
| Education | Illiterate | 76.00 (1.34) | <0.001 |
| Primary | 76.17 (1.39) | ||
| High-school and Diploma | 76.46 (1.48) | ||
| Bachelor of Science and Under | 76.98 (1.49) | ||
| Master of Science and Higher | 77.38 (1.39) | ||
| Total | 76.47 (1.49) | ||
| Household costs | First quintile (20%) | 76.20 (1.39) | <0.001 |
| Second quintile (40%) | 76.30 (1.44) | ||
| Third quintile (60%) | 76.45 (1.48) | ||
| Fourth quintile (80%) | 76.61 (1.53) | ||
| Fifth quintile (100%) | 76.91 (1.55) | ||
| Total | 76.50 (1.50) |
LE and SES
The highest and lowest mean of LE observed in SC1 and SC5, were 77.19 and 76.05 years, respectively. The variances between sub-groups of SES indicator were not equal (p < 0.001). Meanwhile, the mean of LE was significantly different in SES classes (p < 0.001). Notably, the mean of LE within the SC3b and SC4 was not different (p > 0.1).
LE and Total Costs
The lowest mean of LE was observed in the first group (percentile 20), with the lowest non-food costs, and calculated 76.20 years. The variances between sub-groups of total costs indicator were not equal (p<0.001). Meanwhile, the mean of LE was significantly different in total costs groups (p< 0.001).
LE and Education
The lowest observed mean of LE in the first category (illiterate), was 76 years. The variances between sub-groups of education indicator were not equal (p<0.001). Meanwhile, the mean of LE was significantly different in education groups (p< 0.001).
Discussion
In this research, we studied intra-city differences for LE in Tehran mega-city. We further tried to visualize distribution of LE across 22 districts of Tehran for better understanding of associated changes in LE of general population. In addition, using results of Tehran’s Urban HEART-1 project (18), the role of SES, total costs, and education disparities were characterized on LE within various districts. As a main result, substantial disparities were observed among LE of Tehran’s 22 districts. As illustrated in Figure 1, the populations of the northern part districts, are most advantaged districts with higher SES, benefited with more LE compared to southern districts. Meanwhile, the maximum LE was 80 years in females living in north and minimum 72.7 years in males of southern parts which indicate that socioeconomic inequalities within cities could have direct influence on LE within Tehran population.
This is the first report of direct calculation of life expectancy using registered data in Tehran, which inturn correlated with contextual ecologic data of households living in different districts. In previous study, Fereshtehnejad et al. (2010) reported an estimation of LE using a large population sample, which indicated that LE was largely influenced by contextual variables, such as level of education, family size, household expenditures, and social class (19).
Although the influences of various variables of socioeconomic position (20-24), GNP (25), and education level (12-13, 26), on LE have been studied in global and national-scales among populations of countries and states, there are few reports that study these relations within city populations (9). For example, a study in Philadelphia demonstrated that child mortality rate (CMR) in 1971 was 22-per-thousands while at the same time the gap for CMR in two different districts was 18-per-thousands (27). Haan et al., (1987), also, studied white and non-white residents of two federally specified impoverished and advantaged areas of Oakland, Alameda, California for nine-years from 1965 to 1974, and reported that both resident groups of poor areas experienced significantly higher mortalities versus well-off areas (28). McCord and Freeman (1990) studied male residents of Central Harlem health district in New York City, where 41 percent were below the poverty line and predominantly black. They reported an extremely high mortality for them identical or less to rural males of less developed countries (29). Geronimus et al., (1996) studied residents of sixteen persistent poor and affluent areas of different cities in the United States, where the mortality rates of black males (i.e., in Harlem) were escalated compared to advantaged residential places (30). Guest et al., (1998) studied 308 populations of Chicago (77 community areas by gender and by two ethnicities) and estimated their mortality rates. In fact, they have found consistent results with McCord and Freeman (1990) in which mortality rates of black males were three-fold more than non-black males and six-fold more than non-black females (31). Thus, mortality rates and LE have been reported to be quite different within city areas.
In essence, extensive national- and regional-scale studies have studied the role of different socioeconomic and sociodemographic status measures on longevity and life expectancy (9, 24, 32-35). Kulkarni et al., (2011) studied LE disparities across United States counties and found a considerable gap of 15.2 and 12.5 years for men and women, respectively (24). Clarke et al., (2010) reported a substantial impact of neighborhood SES among different age, genders, and ethnicities on LE. They have found that those males of California, which are in the poorest 20% neighborhoods, have the same LE as males of those developing countries that low LEs have been reported for them (32). In another report among general population by Tarkiainen et al., (2012), the role of Finnish people’s income was studied on LE over 20 years. Noteworthy, a gap of LE by 5.1 years among males and 2.9 years among females was observed within maximum and minimum income quintiles (34). Tobias and Cheung (2003), also, studied three ethnicities (i.e., Mäori, Pacific, and European) of New Zealand within four periods from 1995 to 2000, and analyzed LE with increasing/decreasing of deprivation in small areas. Thus, they found a strong association between LE and deprivation, in which longevity of males living in rich areas was nine-years more than their counterparts in deprived areas (36). Besides, a negative correlation between education level of the people and life expectancy has been reported in Bangladesh and Norwegian territories in which educated people have higher longevity (9, 33). Identically, an inverse relationship between education level of the people and longevity has been reported from the United States in which higher mortality rates have been reported for poorly educated people compared with those benefited from better education (37).
Limitations
The first limitation of this study was due to high and unpredictable rate of migration and relocation among the districts. This might have changed somewhat the amount of calculated LEs. The second limitation was ecologic design of the study, which harbored some inherent weaknesses. In fact, ecologic studies suffer from effect of a variety of confounding factors. The third limitation which highlighted specifically in developing countries as well as Iran was mortality registration. The mortality system of record in developing countries suffers from some weaknesses, especially in lower age groups like those with fewer than one year old. This problem might also affect the amount of calculated LEs. However, although the resulted were affected by these limitations, we believe there are considerable validities within these data.
Conclusion
Our findings highlight the inequalities in life expectancy across districts of a megacity, in particular the SES differentials of LE. This study demonstrated that LE had important different within city districts, especially within mega-cities. These inequalities, in fact, underline the importance of resources management within specific regions of the cities—to enhance the quality of life as well as the LE of populations. Meanwhile, LE may be influenced by different factors, such as socioeconomic position, and variations of LE within city districts can be a mirror of inequalities. Nonetheless the results of this study may pave the way for health policy makers, urban planners and health professionals to think more about socioeconomic determinants of this important outcome of health status.
Acknowledgments
This study was part of the MSc thesis in Epidemiology completed by Yaser Mokhayeri, and has been supported by Tehran University of Medical Sciences (grant number 90-12-5-18051). We would like to also thank Behesht-e-Zahra Cemetery Organization and Urban HEART project team members for their wholehearted cooperation in this study. Noteworthy, we extend our unlimited gratitude to Prof. Michael Brauer (School of Population and Public Health, The University of British Columbia, Vancouver, Canada) for his invaluable comments on previous version of the paper. Finally, the authors declare that they have no conflict of interest.
Cite this article as: Mokhayeri Y, Mahmoudi M, Haghdoost A.A, Amini H, Asadi-Lari M, Holakouie Naieni K. How within-city socioeconomic disparities affect life expectancy? Results of Urban HEART in Tehran, Iran. Med J Islam Repub Iran 2014 (26 July). Vol. 28:80.
References
- 1.Mathers C. D, et alHealthy life expectancy in 191 countries, 1999. The Lancet. 2001;357(9269):1685–1691. doi: 10.1016/S0140-6736(00)04824-8. [DOI] [PubMed] [Google Scholar]
- 2.Pourmalek F. et al. Direct estimation of life expectancy in the Islamic Republic of Iran in 2003. Eastern Mediterranean Health Journal. 2009;15(1):76–84. [PubMed] [Google Scholar]
- 3. WHO. Life tables for WHO Member States. 2012 April 15, 2012]; Available from: http://www.who.int/healthinfo/statistics/mortality_life_tables/en/.
- 4.Marmot M. Social determinants of health inequalities. Lancet. 2005;365(9464):1099–1104. doi: 10.1016/S0140-6736(05)71146-6. [DOI] [PubMed] [Google Scholar]
- 5.Woods L.M. et al. Geographical variation in life expectancy at birth in England and Wales is largely explained by deprivation. Journal of Epidemiology and Community Health. 2005;59(2):115–120. doi: 10.1136/jech.2003.013003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Groenewegen P.P, Westert G.P, Boshuizen H.C. Regional differences in healthy life expectancy in the Netherlands. Public Health. 2003;117(6):424–429. doi: 10.1016/S0033-3506(03)00100-8. [DOI] [PubMed] [Google Scholar]
- 7.Crimmins E.M, Saito Y. Trends in healthy life expectancy in the United States, 1970-1990: gender, racial, and educational differences. Social Science & Medicine. 2001;52(11):1629–1641. doi: 10.1016/s0277-9536(00)00273-2. [DOI] [PubMed] [Google Scholar]
- 8.Regidor E. et al. Trends in the association between average income, poverty and income inequality and life expectancy in Spain. Social Science & Medicine. 2003;56(5):961–971. doi: 10.1016/s0277-9536(02)00107-7. [DOI] [PubMed] [Google Scholar]
- 9. Hurt L.S, Ronsmans C, and Saha S. Effects of education and other socioeconomic factors on middle age mortality in rural Bangladesh. Journal of Epidemiology and Community Health 2004; 58(4): p. 315-320. [DOI] [PMC free article] [PubMed]
- 10. Camargos M.C, Machado C.J, and do Nascimento Rodrigues R. Disability life expectancy for the elderly, city of Sao Paulo, Brazil, 2000: gender and educational differences. Journal of Biosocial Science 2007; 39(3): p. 455-63. [DOI] [PubMed]
- 11. Manton K.G, Stallard E, and Corder L. Education-specific estimates of life expectancy and age-specific disability in the U.S. elderly population: 1982 to 1991. Journal of Aging and Health 1997; 9(4): p. 419-50. [DOI] [PubMed]
- 12. Meara E.R, Richards S, and Cutler D.M. The gap gets bigger: changes in mortality and life expectancy, by education, 1981-2000. Health Affairs (Millwood) 2008; 27(2): p. 350-60. [DOI] [PMC free article] [PubMed]
- 13. Shkolnikov V.M, et al. The changing relation between education and life expectancy in central and eastern Europe in the 1990s. Journal of Epidemiology and Community Health 2006; 60(10): p. 875-81. [DOI] [PMC free article] [PubMed]
- 14. Statistical Centre of Iran. Estimated Population of Country Cities for 2010. 2012 April 15, 2012]; Available from: http://www.amar.org.ir/default-2649.aspx.
- 15. Amini H, et al. Land use regression models to estimate the annual and seasonal spatial variability of sulfur dioxide and particulate matter in Tehran, Iran. Science of the Total Environment 2014; 488: p. 343-353.. [DOI] [PubMed]
- 16. Behesht-e-Zahra Cemetery Organization, death data for 2010. 2011: Tehran, Iran.
- 17. 0 United Nations Population Division, MORTPAK for Windows 2003, United Nations: New York.
- 18. Asadi-Lari M, et al. The application of urban health equity assessment and response tool (Urban HEART) in Tehran; concepts and framework. Medical Journal of the Islamic Republic of Iran 2010; 24(3): p. 175-185. [PMC free article] [PubMed]
- 19. Fereshtehnejad S.M, et al. Estimation of Life Expectancy and its Association with Social Determinants of Health (SDH) in Urban Population of different districts of Tehran in 2008 (Urban HEART Study). Teb & Tazkieh 2010; (77): p. 25-44.
- 20. Shah A, et al. A cross-national study of the relationship between elderly suicide rates and life expectancy and markers of socioeconomic status and health care. International Psychogeriatrics 2008; 20(2): p. 347-60. [DOI] [PubMed]
- 21. Singh G.K, and Siahpush M. Widening socioeconomic inequalities in US life expectancy, 1980-2000. International Journal of Epidemiology 2006; 35(4): p. 969-79. [DOI] [PubMed]
- 22. Kurimori S, et al. Calculation of prefectural disability-adjusted life expectancy (DALE) using long-term care prevalence and its socioeconomic correlates in Japan. Health Policy 2006; 76(3): p. 346-58. [DOI] [PubMed]
- 23. Kaneda T, Zimmer Z, and Tang Z. Socioeconomic status differentials in life and active life expectancy among older adults in Beijing. Disability and Rehabilitation 2005; 27(5): p. 241-51. [DOI] [PubMed]
- 24. Kulkarni S.C, et al. Falling behind: life expectancy in US counties from 2000 to 2007 in an international context. Population Health Metrics 2011; 9(1): p. 16. [DOI] [PMC free article] [PubMed]
- 25. Heinemann L, Dinkel R, and Gortler E. Life expectancy in Germany: possible reasons for the increasing gap between East and West Germany. Reviews on Environmental Health 1996; 11(1-2): p. 15-26. [DOI] [PubMed]
- 26. Minicuci N, and Noale M. Influence of level of education on disability free life expectancy by sex: the ILSA study. Experimental Gerontology 2005; 40(12): p. 997-1003. [DOI] [PubMed]
- 27. Mausner J.S, and Kramer S. Epidemiology: An introductory text. 1985, Philadelphia: W.B. Saunders Company.
- 28. Haan M, Kaplan G.A, and Camacho T. Poverty and health prospective evidence from the alameda county study1. American Journal of Epidemiology 1987; 125(6): p. 989-998. [DOI] [PubMed]
- 29. McCord C, and Freeman H.P. Excess mortality in Harlem. New England Journal of Medicine 1990; 322(3): p. 173-177. [DOI] [PubMed]
- 30. Geronimus A.T, et al. Excess mortality among blacks and whites in the United States. New England Journal of Medicine 1996; 335(21): p. 1552-1558. [DOI] [PubMed]
- 31. Guest A.M, Almgren G, and Hussey J.M. The ecology of race and socioeconomic distress: infant and working-age mortality in Chicago. Demography 1998; 35(1): p. 23-34. [PubMed]
- 32. Clarke C.A, et al. Racial and social class gradients in life expectancy in contemporary California. Social Science & Medicine 2010; 70(9): p. 1373-1380. [DOI] [PMC free article] [PubMed]
- 33. Steingrímsdóttir Ó.A, et al. Trends in life expectancy by education in Norway 1961–2009. European Journal of Epidemiology 2012; p. 1-9. [DOI] [PubMed]
- 34. Tarkiainen L, et al. Trends in life expectancy by income from 1988 to 2007: decomposition by age and cause of death. Journal of Epidemiology and Community Health 2012; 66(7): p. 573-578. [DOI] [PubMed]
- 35. Carter K.N, Blakely T, and Soeberg M. Trends in survival and life expectancy by ethnicity, income and smoking in New Zealand: 1980s to 2000s. New Zealand Medical Journal 2010; 123(1320): p. 13-24. [PubMed]
- 36. Tobias M.I, and Cheung J. Monitoring health inequalities: life expectancy and small area deprivation in New Zealand. Population Health Metrics 2003; 1(2): p. 14. [DOI] [PMC free article] [PubMed]
- 37. Pappas G, et al. The increasing disparity in mortality between socioeconomic groups in the United States, 1960 and 1986. New England Journal of Medicine 1993; 329(2): p. 103-109. [DOI] [PubMed]