

Abstract
Pulmonary tumor thrombotic microangiopathy (PTTM) is a highly fatal complication of cancer leading to acute cor pulmonale and pulmonary hypertension. We present a case of 47-year-old male patient who developed acute breathlessness and died suddenly. The pulmonary vessels at autopsy on histopathologic examination showed the presence of fibrocellular intimal proliferation, fibrin thrombi and few tumor emboli consisting of malignant adenocarcinoma cells. There was associated lymphangiosis carcinomatosis. No primary visceral tumor was found despite extensive search. The patient had died following acute cor pulmonale with sudden pulmonary hypertension due to PTTM. This entity (PTTM) must be kept as a differential diagnosis in patients presenting with acute breathlessness especially in cases of cancers.
KEY WORDS: Acute cor pulmonale, adenocarcinoma, carcinomatosis endarteritis, pulmonary tumor thrombotic microangiopathy
INTRODUCTION
Pulmonary tumor thrombotic microangiopathy (PTTM) also known as carcinomatosis endarteritis is a highly fatal respiratory complication seen in cases of malignancies especially adenocarcinomas of the stomach.[1,2,3] It was first described by von Herbay et al.[1] There are only around 80 cases reported in literature so far including less than 10 cases where the primary malignancy has not been detected even after extensive search.[4,5] The clinical diagnosis is extremely difficult and is most often detected at autopsy. The patients develop sudden pulmonary hypertension and acute cor pulmonale.[6]
CASE REPORT
We present an autopsy case of a 47-year-old male patient who developed acute breathlessness and died suddenly. At autopsy there was mild right ventricular dilatation and lungs showed few firm areas and prominent bronchovasculature. No mass lesion was noted anywhere. On microscopy, the lungs showed the presence of florid fibrocellular intimal proliferation of the arterioles and small arteries [Figure 1]. Vessels showed fibrin thrombi and occasional vessel showed tumor emboli composed of neoplastic adenocarcinoma cells showing glandular and occasional signet ring morphology. There was evidence of lymphangiosis carcinomatosis [Figure 2]. There were similar tumor emboli in the myocardium, peripancreatic tissue, and perigastric lymph nodes [Figure 3]. Despite extensive sectioning no primary tumor was found. The immunohistochemistry results showed positivity for pan keratin indicating an epithelial tumor. Tumor cells were negative for CK 7, CK10, TTF 1, and PSA. The final cause of death was given as acute cor pulmonale following pulmonary tumor thrombotic microangiopathy in an unknown primary adenocarcinoma.
Figure 1.
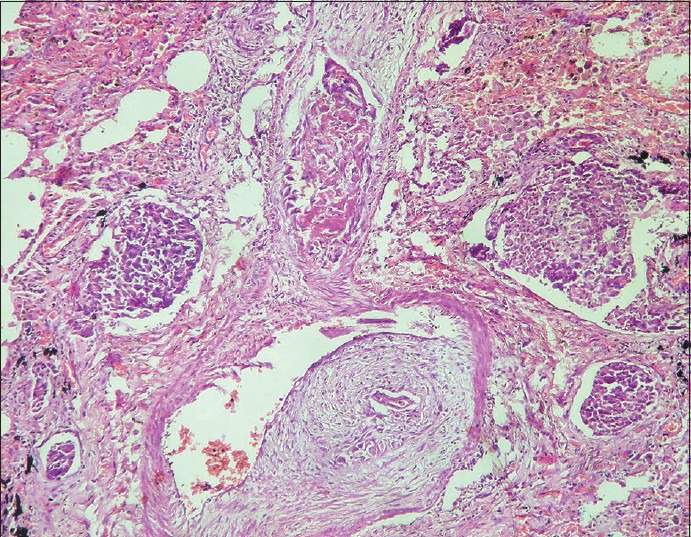
Lungs showing presence of florid fibrocellular intimal proliferation with fibrin thrombi of the arterioles and small arteries (H and E, ×100)
Figure 2.
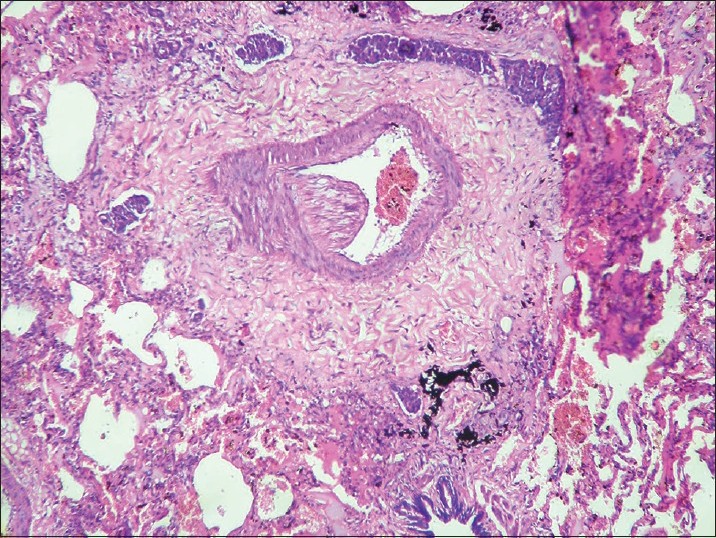
Lungs showing presence of lymphangiosis carcinomatosis (H and E, ×100)
Figure 3.
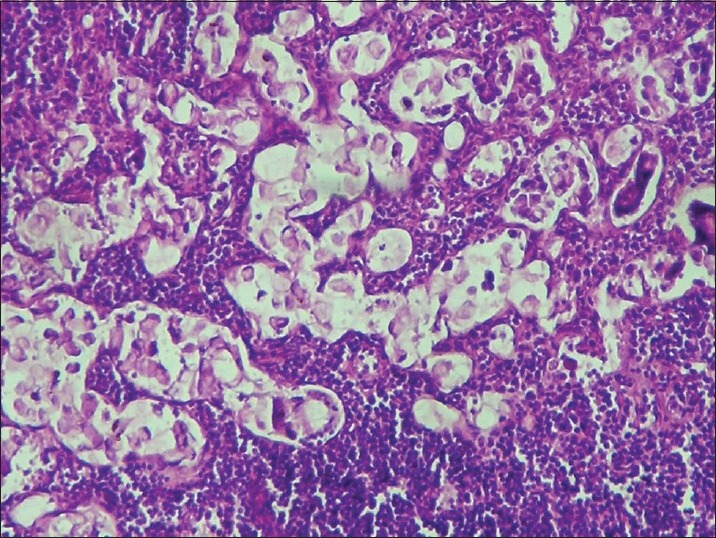
Signet ring cells seen in the lymph nodes (H and E, ×400)
DISCUSSION
PTTM is characterized by intimal proliferation in pulmonary small arteries and arterioles with or without tumor emboli leading to vascular stenosis and pulmonary hypertension. There is no distinct pulmonary tumour mass or interstitial involvement. It was first described by von Herbay et al.[1] There are around 80 cases reported in literature so far. In our case also there was no mass lesion or parenchymal involvement by the tumor. There was florid fibrointimal proliferation, fibrin thrombi with some showing occasional tumor emboli and lymphangimatosis carcinomatosis. The tumor cells in this condition invade the pulmonary vascular system occluding the small arteries, arterioles and activate coagulation systems releasing inflammatory mediators, growth factors like serotonin, vascular endothelial growth factor and osteopontin. Some authors have proposed screening with serum VEGF and D - dimer testing for early detection of PTTM.[7] The primary sites of malignancy reported are gastrointestinal tract, ovary, breast, pancreas, liver, uterus, gall bladder, and prostate.[8] However, rarely there are reported cases where primary has not been detected inspite of extensive search and immunohistochemical stains.[4] In our case too despite an extensive search no primary mass was found. Also immunohistochemistry was equivocal with no specific markers positive. Thus, our case belongs to the rare set of PTTM with unknown primary of which only less than 10 cases have been reported.[4,5] PTTM is a rare condition with very high mortality. It should be distinguished from ordinary pulmonary thromboembolism and primary pulmonary hypertension and should be considered as a differential diagnosis in patients with acute respiratory symptoms especially in cases with an underlying cancer. There are only occasional case reports of antemortem diagnosis with patient recovering completely, and hence it is important to have a higher clinicopathological awareness of diagnosing this highly fatal condition.[9] Role of 2-(F-18)-fluoro-2-deoxy-d-glucose positron emission tomography (FDG-PET) has been described in literature and has been described to be helpful for the diagnosis of PTTM.[10,11]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.von Herbay A, Illes A, Waldherr R, Otto HF. Pulmonary tumor thrombotic microangiopathy with pulmonary hypertension. Cancer. 1990;66:587–92. doi: 10.1002/1097-0142(19900801)66:3<587::aid-cncr2820660330>3.0.co;2-j. [DOI] [PubMed] [Google Scholar]
- 2.Guimarães MD, Almeida MF, Brelinger A, Barbosa PN, Chojniak R, Gross JL. Diffuse bronchiolitis pattern on a computed tomography scan as a presentation of pulmonary tumor thrombotic microangiopathy: A case report. J Med Case Rep. 2011;5:575. doi: 10.1186/1752-1947-5-575. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gru AA, Pai RK, Roma AA. Pulmonary tumor thrombotic microangiopathy in patients with low-grade ovarian serous neoplasms: A clinicopathologic review of 2 cases of a previously unknown association. Int J Gynecol Pathol. 2012;31:438–42. doi: 10.1097/PGP.0b013e318249287d. [DOI] [PubMed] [Google Scholar]
- 4.Hazeki N, Kobayashi K, Yamamoto M, Kotani Y, Kondo T, Nishimura Y. Pulmonary tumor thrombotic microangiopathy associated with cancer of unknown origin. [Article in Japanese] Nihon Kokyuki Gakkai Zasshi. 2009;47:1030–5. [PubMed] [Google Scholar]
- 5.Patrignani A, Purcaro A, Calcagnoli F, Mandolesi A, Bearzi I, Ciampani N. Pulmonary tumor thrombotic microangiopathy: The challenge of the antemortem diagnosis. J Cardiovasc Med (Hagerstown) 2013 doi: 10.2459/JCM.0b013e328354e473. [DOI] [PubMed] [Google Scholar]
- 6.Yokomine T, Hirakawa H, Ozawa E, Shibata K, Nakayama T. Pulmonary thrombotic microangiopathy caused by gastric carcinoma. J Clin Pathol. 2010;63:367–9. doi: 10.1136/jcp.2010.075739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kuwabara H, Yoshida S, Takasu T, Yuki M, Goto I, Hanafusa T, et al. Pulmonary tumor thrombotic microangiopathy caused by gastric cancer. Ann Thorac Med. 2012;7:168–9. doi: 10.4103/1817-1737.98853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pinckard JK, Wick MR. Tumour-related thrombotic pulmonary microangiopathy: Review of pathologic findings and pathophysiologic mechanism. Ann Diagn Pathol. 2000;4:154–7. doi: 10.1016/s1092-9134(00)90038-8. [DOI] [PubMed] [Google Scholar]
- 9.Miyano S, Izumi S, Takeda Y, Tokuhara M, Mochizuki M, Matsubara O, et al. Pulmonary tumor thrombotic microangiopathy. J Clin Oncol. 2007;25:597–9. doi: 10.1200/JCO.2006.09.0670. [DOI] [PubMed] [Google Scholar]
- 10.Cicone F, Del Forno M, Papa A, Comito F, Festa A, Uccini S, et al. Fatal pulmonary tumour thrombotic microangiopathy: Do typical FDG-PET findings exist? Nuklearmedizin. 2012;51:N6–9. [PubMed] [Google Scholar]
- 11.Tashima Y, Abe K, Matsuo Y, Baba S, Kaneko K, Isoda T, et al. Pulmonary tumor thrombotic microangiopathy: FDG-PET/CT findings. Clin Nucl Med. 2009;34:175–7. doi: 10.1097/RLU.0b013e3181966f5c. [DOI] [PubMed] [Google Scholar]