

Abstract
Introduction:
Stone disease is a significant and world-wide health problem. Recently, certain drugs have been used as a supplement to observation alone in an effort to improve spontaneous stone expulsion. We evaluated the efficacy of nifedipine and alfuzosin in the medical treatment of symptomatic, uncomplicated distal ureteral stones.
Materials and Methods:
This was a randomized controlled prospective study to determine the efficacy of alfuzosin and nifedipine as an adjunctive medical therapy, to increases the stone-expulsion rates in distal ureteric calculus of size ≤10 mm. Investigators and patients were blinded to the randomization scheme. Patients were randomly divided into three equal groups of 35 patients each. Patients in Group I received tablet nifedipine 30 mg/day, Group II received alfuzosin 10 mg/day and Group III was the control group received tablet diclofenac sodium. The patient blood pressure, stone position on imaging, number of pain attacks, time of stone-expulsion, hospital re-admission and any adverse events were assessed. Patients were followed-up weekly and continued until the patient was rendered stone free or up to 28 days. Statistical analysis was performed and P < 0.05 was considered to be significant.
Results:
Stone-expulsion was observed in 60%, 85.7% and 20% patients in Group I, II and III respectively. A statistically significant difference was noted in between Groups I versus III, Groups II versus III and Groups I versus II (P < 0.0001, P < 0.0001, and P < 0.0315 respectively). The mean number of pain attacks was 2.91 ± 1.01 for Group I, 1.8 ± 0.83 for Group II, and 2.82 ± 1.12 for Group III, which is statistical significant in Groups II versus III, and Groups I versus II (P < 0.001 and P < 0.001). Hospital re-admission rate was less in treatment groups when compare to control group (P < 0.0001).
Conclusion:
The use of alfuzosin and nifedipine as a medical expulsive therapy for distal ureteric stones proved to be safe and effective in term of increased stone-expulsion rate, reduced pain attacks and decrease hospital re-admissions.
Keywords: Alfuzosin, distal ureteral stones, medical expulsive therapy, nifedepine
INTRODUCTION
Urinary stone disease is a common condition affecting up to 12% of the world population. A large number of patients presenting in surgical emergency have symptoms and signs of ureteric colic. Many of these patients suffer from distal ureteric stones (70%). Spontaneous expulsion of distal ureteral stones of ≤10 mm diameter occurs in 25-53% of cases.[1] The watchful waiting approach can result in complications, such as infection of the urinary tract, hydronephrosis, and deranged renal function.[2] Ureteric stones have been treated traditionally with interventional techniques like ureteroscopy or open surgery. In recent years, medical expulsive therapy (MET) has been used in the management of distal ureteric stones as a supplement to conservative treatment. Drugs such as α1 receptor blockers, calcium channel blockers, prostaglandins synthesis inhibitors, antihistamines, glyceryl trinitrate, and corticosteroids are used for MET. Factors influencing the spontaneous passage of ureteral stones are stone size, configuration, location, smooth muscle spasm, sub-mucosal edema, and anatomy.[3,4,5]
Alpha blockers, calcium channel blockers are the most commonly used drugs for MET. Tamsulosin has been the most commonly studied α−1 blocker; however, alfuzosin is a combined α−1 A and α−1 D selective adrenergic antagonist resulting in relaxation of distal ureteric smooth muscles to facilitate passage of stone, and relieving pain. It is easily available and has less cardiac and ejaculatory side effects. Nifedipine is a calcium channel blocker, which acts by relieving the smooth muscle spasm in the ureter without interfering with its peristaltic activity. It is effective in stone-expulsion and relieving pain.[4] Therefore, we performed a comparative study to evaluate the efficacy of nifedipine and alfuzosin in the medical management of symptomatic, uncomplicated distal ureteral stones.
MATERIALS AND METHODS
Between November 2008 -and October 2010, patients presenting with renal colic were enrolled for this double-blind, randomized, controlled study. Patients were assessed with history, physical examination and investigated with complete blood count, blood urea, serum creatinine, routine urine analysis, X-rays kidney, ureter, and bladder (KUB), ultrasonography, intravenous urography and helical computed tomography (CT) whenever was necessary. Patients ≥8 years of either sex with a single, unilateral ureteral stone of ≤10 mm were included. The distal ureter was defined as the segment from the lower border of the sacroiliac joint to the vesico-ureteric junction. Patients having previous surgery on the ipsilateral ureter, bilateral ureteric stones, multiple stones, solitary kidney, urinary tract infection, moderate or severe hydronephrosis, contraindications for non-steroidal anti-inflammatory drugs (e.g. gastritis), known allergy to tamsulosin or alfuzosin, renal insufficiency, or currently on α-blocker therapy, and pregnant or lactating women were excluded. The study was approved by the ethical committee of hospital.
Sample size calculation and randomization
Spontaneous expulsion rate for lower ureteric stones ranges between 25% and 60%. We took an average rate of spontaneous stone-expulsion as 40% and also considered an expected increase of this rate by 35% from baseline after MET. Taking significance level α at 95% and power of study 80%, the sample size was calculated by using formula [N = 2 ×{z1−α + z1−β/d−δ0}2 × p (1 − p), where N = size/group; P = spontaneous expulsion rate; Zα = standard normal deviate for one sided test; d = expected difference: δ0 = clinically acceptable margin (taken as 0.05). The sample size for each group was fixed at 35 and total for three groups was 105. Block randomization was used to achieve balance in the allocation of patients to different treatment groups. To get 35 patients in each group, 7 blocks of sample size 15 were created by a statistician. The details of blocks were given to the pharmacist. Packaging of drugs was done in this order to achieve blinding. After taking written informed consent, patients received tablet nifedipine 30 mg/day in Group I, tablet alfuzosin 10 mg/day in Group II and tablet diclofenac sodium in Group III as a control group. Patients in all 3 groups received tablet diclofenac sodium (50 mg) every 12 hourly for 1 week and injection diclofenac sodium (75 mg) as needed. An intramuscular injection Tramadol hydrochloride 100 mg was given for persistent pain.
Patients were followed-up weekly up to 28 days; history of stone passage, number of pain episodes were recorded and investigated with routine urine examination, kidney function test and X-ray KUB. Patients were advised to watch for stone-expulsion. Medications were stopped after spontaneous stone-expulsion, any intervention before the end of the study, and adverse effect. For patients with a stone-free ureter on the last imaging, but no documented stone-expulsion, the last date of positive stone status was recorded. Abdominal CT was performed for patients with radiolucent stones if the stone was not expelled by the end of the study. Patients underwent ureteroscopic stone removal for persistent stones after 28 days. Patients having uncontrollable pain were readmitted for injectable analgesics and medication was continued. The blood pressure, stone position on imaging, number of pain attacks, time of stone-expulsion, hospital re-admission and any adverse events were recorded.
Statistical analysis
Data analysis was performed using Statistical Package for the Social Sciences trial version 17.1 statistical software. Student's t-test, ANOVA, Chi-square, and Fisher's exact test were applied as required. The power of the study was 0.80, and the level of significance was 95%.
RESULTS
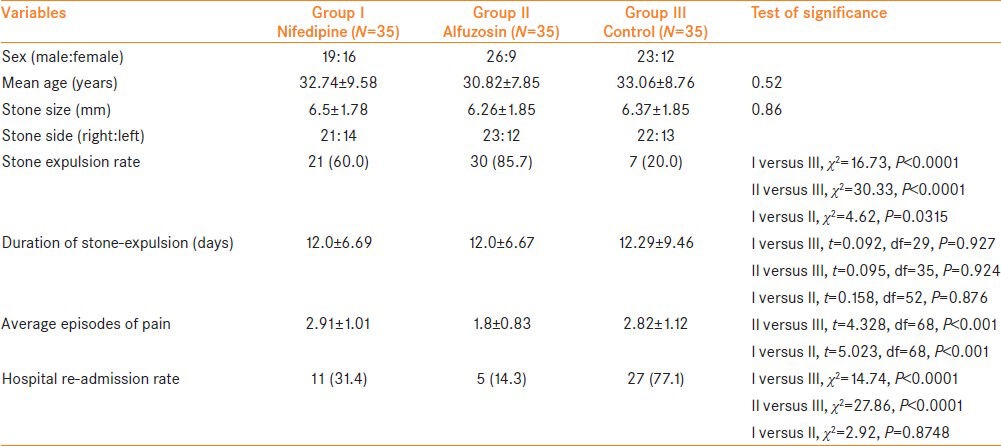
A total of 246 patients with symptoms of ureteric colic were assessed for inclusion, of which 102 patients were excluded as they did not have distal urolithiasis. Of the remaining 146 patients, 105 were eligible and included for the study. [Figure 1]. Group I had 19 male and 16 female (mean age: 32.74 ± 9.58 years), Group II had of 26 male and 9 female (mean age: 30.82 ± 7.85 years), and Group III had 23 male and 12 female (mean age: 33.06 ± 8.76 years). The mean stone size was 6.5 ± 1.78 mm for Group I, 6.26 ± 1.85 mm for Group II, and 6.37 ± 1.85 mm for Group III. There were no statistically significant differences between the groups in terms of sex, age, or stone size (P > 0.05).
Figure 1.
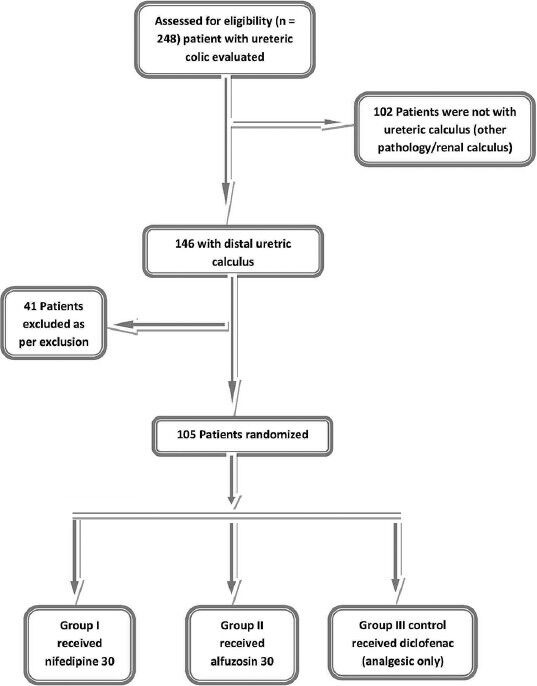
Trial profile all randomized patients completed trial
A statistical significant difference was observed for stone-expulsion rate between Group I versus Group II (60% vs. 85.7%, P < 0.0315), Group I versus Group III (60% vs. 20%, P < 0.000) and Group II versus Group III (85.7% vs. 20%, P < 0.000). Average time for stone-expulsion was 12.6 ± 6.69 days in Group I, 12.0 ± 6.67 days in Group II, and 12.29 ± 9.46 days in Group III. No statistically significant difference was observed in time for stone-expulsion between these groups.
Patients taking alfuzosin had fewer pain attacks compared with others. The average number of pain attacks was 2.91 ± 1.01 for Group I, 1.8 ± 0.83 for Group II, and 2.82 ± 1.12 for Group III patients. A significant statistical difference was observed between Groups II versus III, and Groups I versus II (P < 0.001 and P < 0.001, respectively).
Hospital re-admissions due to uncontrollable pain occurred in 43 patients: 11 patient (31.4%) in Group I, five patients (14.3%) in Group II, and 27 patients (77.1%) in Group III. The difference was statistically significant (P < 0.0001) in Group I versus Group II and Group II versus Group III [Table 1].
Table 1.
Demographic data of all 3 groups
DISCUSSION
Recent advances in ureteric stone management have allowed these to be treated using minimally invasive techniques, which have increased success rates and decreased treatment related morbidity. These advances include shock wave lithotripsy and ureteroscopic lithotripsy. Although these approaches are less invasive than traditional open surgical methods, they are expensive and have inherent risks. Consequently, observation has been advocated for small ureteral stones which have a high probability to pass spontaneously. Observation can be supplemented by using MET. The factors influencing expulsion of calculi include stone size, shape, and location, ureteric edema, and convolutions. (Of these, the location of the calculus and its size are the most important factors.[1]
Malin et al. first demonstrated the presence of alpha - adrenergic receptors in the human ureter in 1970.[6] Recently, Sigala et al.[7] studied the presence of α−1 adrenergic receptor gene and protein expression in the proximal, middle, and distal ureter. Characteristic distribution of α−1 receptor subtypes in distal, middle, and proximal segments is α 1D > α 1A > α 1B.[8] α−1D was the most common receptor present in all portions of the ureter. It has the strongest effect on the contractions of distal ureter and bladder detrusor, especially for the ureter-bladder wall section, and therefore plays an important role in the distal ureter. α−1 receptor blockers relax ureteral smooth muscle, reduce peristalsis frequency and amplitude, decrease intraluminal pressure of the ureter, enhance transportation capability and pulses of urine. Moreover, they establish pressure gradient surrounding calculi by increasing the pressure above calculi, relax smooth muscles of the bladder neck and urethra, and finally form one thrust to expel calculi. α1-receptor blockers can also affect the C-type fast fiber of the spinal cord and the sympathetic post-ganglionic neuron; block the pain transmission pathway to central nervous system and reduce renal colic during the process of calculi expulsion.[9] Hellstrom and Sikka[10] studied the effect of tamsulosin and alfuzosin on ejaculatory function and concluded that marked decrease in ejaculatory volume in almost 90% of subjects and anejaculation in approximately 35% of individuals taking tamsulosin. Thus, we chose to study alfuzosin to avoid ejaculatory disturbance.
The basic functional unit of the ureter is the smooth muscle cell, which reacts to calcium concentration change: contraction with an increase in calcium concentration and diastole when calcium concentration decreases. Ideal MET drugs should inhibit incongruous contraction but without influencing the slow peristalsis. Previous studies indicated that calcium antagonist could inhibit the fast contraction phase of animal and human ureter, but without any effect on the tonic activities.[11,12] Therefore, this kind of drug was thought to have potential use for calculi expulsion. Nifedipine is one potential calcium channel antagonist with lows adverse effect. In an article in 1994 Borghi et al.[13] demonstrated the efficacy of calcium channel blockers in the treatment of ureteral stones. They enrolled 86 patients to receive methylprednisolone with placebo or nifedipine. Patients receiving nifedipine had a significantly higher rate of stone passage compared with the placebo group, 87% versus 65%.
A meta-analysis compared stone passage rates in patients who were given calcium channel blockers or α1-adrenergic receptor antagonist versus controls who did not receive these medications. They demonstrated a 65% greater chance of passing a ureteral stone in patients who received either medication.[14] Another study also showed that calcium channel antagonist could promote distal calculi expulsion and reduce analgesia requirement, renal colic rate, and hospitalization rate.[15]
The comparison of alfuzosin and tamsulosin in the management of lower ureteral calculi has shown that both drugs increase the stone-expulsion rate (82.3% vs. 70.5%), decrease expulsion time (12.3 versus 14.5) and reduce the need for analgesics[16] We chose Alfuzosin because it is easily available and like tamsulosin has comparatively less cardiac side effects than other alpha1 blockers like doxazosin or terazosin. Moreover, it is a combined α1 A and α1 D – selective adrenergic antagonist. Pedro et al.[17] conducted a double-blinded placebo-controlled trial on 76 patients to test the efficacy of alfuzosin for distal ureteral stones, and concluded that alfuzosin improves patient comfort associated with stone passage and decreases the time to distal ureteral stone passage but does not increase the rate of spontaneous stone passage (77.1% for placebo and 73.5% for alfuzosin, P = 0.83). Whereas in our study statistically significant difference was noted in alfuzosin (85.7%) and nifedipine (60%) for stone-expulsion rates (P < 0.05) when compared with control group (20%). In another randomized placebo-controlled trial study done by Pirzada et al.[18] on 60 patients to test the efficacy of alfuzosin in kidney stones which are fragmented by extracorporeal shock-wave lithotripsy and authors concluded that stone-expulsion was significantly higher in alfuzosin group when compared to placebo (76.7% and 46.7% respectively, P = 0.01).
Our results confirmed the efficacy of nifedipine and alfuzosin for distal ureteric stones. Nearly60% of patient taking nifedipine and 85.7% of patients taking alfuzosin were able to expel their stones at the end of study compared to 20% in the control group. Alfuzosin was found to be significantly better in term of stone-expulsion compared to nifedipine and control group (P < 0.05). Moreover, both nifedipine and alfuzosin groups hade significantly less hospital re-admission rate as compared to the control group (P < 0.0001).
Nifedipine and alfuzosin also decreased the frequency of pain attacks. Patients taking alfuzosin had significantly less pain as compared to nifedipine and placebo group (P < 0.001). Use of α-blockers for expulsion of ureteral stones probably decreases the analgesic requirement in two ways: Expulsion of stones, leading to longer stone free periods, and blockade of C-fibers. It is difficult to assess which of these may be primarily responsible for decreasing the analgesic requirement, because α-blockers are known to be associated with both.
The most frequently reported adverse event with α blockers was transient hypotension[19] Pedro et al. reported 12% adverse events in the alfuzosin group compared with 0% in the placebo group.[17] whereas Yilmaz et al. have reported no serious adverse events.[20] In the present study, MET related side effects were observed in four patients (three patients taking alfuzosin developed retrograde ejaculation and one patient taking nifedipine developed an episode of hypotension), but they were able to complete the study. No patients developed serious side effects during the study period. Patients who were not stone free after the 4 week follow-up were successfully treated with ureteroscopy. This study demonstrated that neither watchful waiting nor medical therapy seems to negatively affect the success rate of stone removal.
CONCLUSIONS
Medical expulsion therapy is a useful adjunct to observation in the conservative management of ureteral stones. The use of alfuzosin and nifedipine for uncomplicated distal ureteric stones is safe and effective in term of increased stone-expulsion rate, reduced pain attacks and decrease hospital re-admissions. Alfuzosin was found to be significantly better in terms of stone-expulsion rate and pain attacks as compared to nifedipine.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Segura JW, Preminger GM, Assimos DG, Dretler SP, Kahn RI, Lingeman JE, et al. Ureteral stones clinical guidelines panel summary report on the management of ureteral calculi. The American urological association. J Urol. 1997;158:1915–21. doi: 10.1016/s0022-5347(01)64173-9. [DOI] [PubMed] [Google Scholar]
- 2.Lotan Y, Gettman MT, Roehrborn CG, Cadeddu JA, Pearle MS. Management of ureteral calculi: A cost comparison and decision making analysis. J Urol. 2002;167:1621–9. [PubMed] [Google Scholar]
- 3.Porpiglia F, Destefanis P, Fiori C, Fontana D. Effectiveness of nifedipine and deflazacort in the management of distal ureter stones. Urology. 2000;56:579–82. doi: 10.1016/s0090-4295(00)00732-9. [DOI] [PubMed] [Google Scholar]
- 4.Dellabella M, Milanese G, Muzzonigro G. Efficacy of tamsulosin in the medical management of juxtavesical ureteral stones. J Urol. 2003;170:2202–5. doi: 10.1097/01.ju.0000096050.22281.a7. [DOI] [PubMed] [Google Scholar]
- 5.Coll DM, Varanelli MJ, Smith RC. Relationship of spontaneous passage of ureteral calculi to stone size and location as revealed by unenhanced helical CT. AJR Am J Roentgenol. 2002;178:101–3. doi: 10.2214/ajr.178.1.1780101. [DOI] [PubMed] [Google Scholar]
- 6.Malin JM, Jr, Deane RF, Boyarsky S. Characterisation of adrenergic receptors in human ureter. Br J Urol. 1970;42:171–4. doi: 10.1111/j.1464-410x.1970.tb10018.x. [DOI] [PubMed] [Google Scholar]
- 7.Sigala S, Dellabella M, Milanese G, Fornari S, Faccoli S, Palazzolo F, et al. Evidence for the presence of alpha1 adrenoceptor subtypes in the human ureter. Neurourol Urodyn. 2005;24:142–8. doi: 10.1002/nau.20097. [DOI] [PubMed] [Google Scholar]
- 8.Obara K, Takeda M, Shimura H, Kanai T, Tsutsui T, Komeyama T, et al. Alpha-1 adrenoreceptors subtypes in the human ureter. Characterization by RT-PCR and in situ hybridization. J Urol. 1996;155:472A. [Google Scholar]
- 9.Kinnman E, Nygårds EB, Hansson P. Peripheral alpha-adrenoreceptors are involved in the development of capsaicin induced ongoing and stimulus evoked pain in humans. Pain. 1997;69:79–85. doi: 10.1016/s0304-3959(96)03257-5. [DOI] [PubMed] [Google Scholar]
- 10.Hellstrom WJ, Sikka SC. Effects of acute treatment with tamsulosin versus alfuzosin on ejaculatory function in normal volunteers. J Urol. 2006;176:1529–33. doi: 10.1016/j.juro.2006.06.004. [DOI] [PubMed] [Google Scholar]
- 11.Andersson KE, Forman A. Effects of calcium channel blockers on urinary tract smooth muscle. Acta Pharmacol Toxicol (Copenh) 1986;58(Suppl 2):193–200. doi: 10.1111/j.1600-0773.1986.tb02536.x. [DOI] [PubMed] [Google Scholar]
- 12.Hannappel J, Rohrmann D, Lutzeyer W. Pharmacologic modification of ureteral activity. Urologe A. 1986;25:246–51. [PubMed] [Google Scholar]
- 13.Borghi L, Meschi T, Amato F, Novarini A, Giannini A, Quarantelli C, et al. Nifedipine and methylprednisolone in facilitating ureteral stone passage: A randomized, double-blind, placebo-controlled study. J Urol. 1994;152:1095–8. doi: 10.1016/s0022-5347(17)32511-9. [DOI] [PubMed] [Google Scholar]
- 14.Hollingsworth JM, Rogers MA, Kaufman SR, Bradford TJ, Saint S, Wei JT, et al. Medical therapy to facilitate urinary stone passage: A meta-analysis. Lancet. 2006;368:1171–9. doi: 10.1016/S0140-6736(06)69474-9. [DOI] [PubMed] [Google Scholar]
- 15.Seitz C, Liatsikos E, Porpiglia F, Tiselius HG, Zwergel U. Medical therapy to facilitate the passage of stones: What is the evidence? Eur Urol. 2009;56:455–71. doi: 10.1016/j.eururo.2009.06.012. [DOI] [PubMed] [Google Scholar]
- 16.Agrawal M, Gupta M, Gupta A, Agrawal A, Sarkari A, Lavania P. Prospective randomized trial comparing efficacy of alfuzosin and tamsulosin in management of lower ureteral stones. Urology. 2009;73:706–9. doi: 10.1016/j.urology.2008.11.013. [DOI] [PubMed] [Google Scholar]
- 17.Pedro RN, Hinck B, Hendlin K, Feia K, Canales BK, Monga M. Alfuzosin stone expulsion therapy for distal ureteral calculi: A double-blind, placebo controlled study. J Urol. 2008;179:2244–7. doi: 10.1016/j.juro.2008.01.141. [DOI] [PubMed] [Google Scholar]
- 18.Pirzada AJ, Anwar A, Atif J, Memon I, Ariz M. Role of alpha-1 blocker in expulsion of stone fragments after extracorporeal shock wave lithotripsy for renal stones. J Ayub Med Coll Abbottabad. 2011;23:125–9. [PubMed] [Google Scholar]
- 19.Cooper JT, Stack GM, Cooper TP. Intensive medical management of ureteral calculi. Urology. 2000;56:575–8. doi: 10.1016/s0090-4295(00)00658-0. [DOI] [PubMed] [Google Scholar]
- 20.Yilmaz E, Batislam E, Basar MM, Tuglu D, Ferhat M, Basar H. The comparison and efficacy of 3 different alpha1-adrenergic blockers for distal ureteral stones. J Urol. 2005;173:2010–2. doi: 10.1097/01.ju.0000158453.60029.0a. [DOI] [PubMed] [Google Scholar]