

In Brief
This cross-sectional audit investigates the prevalence and determinants of anemia in older people with diabetes attending an outpatient clinic. Anemia was found to be highly prevalent, affecting 59% of patients. Older age and longer duration of diabetes were the main predictors of anemia, whereas the presence of chronic kidney disease was a mediator rather than a direct cause.
The prevalence of anemia increases with increasing age, affecting ∼ 10% of the general population ≥ 65 years of age.1 However, the prevalence of anemia in patients with diabetes could be double this figure.2 Anemia in patients with diabetes is likely to be related to renal insufficiency. However, it has been shown that diabetes increases the risk for developing anemia by two- to threefold compared to those without diabetes and similar renal function, suggesting that diabetes is associated with other underlying causes of anemia in addition to renal impairment.2
In the elderly, anemia is an independent predictor of adverse outcomes such as poor quality of life, falls, decreased physical function, impaired cognition, increased infections, and mortality.3 It has also been shown that anemia is associated with impaired activities of daily living, increased disability, and hospitalization.4,5 Therefore, recognizing and treating the underlying cause of the anemia is an important aspect of patient care.
Underlying causes of anemia in older people with diabetes are likely to be multiple, including decreased renal function, inflammation, bone marrow suppression, and nutritional deficiencies.6 Although the prevalence of anemia increases with age,7 there is a dearth of literature investigating the burden of anemia in old (≥ 75 years of age) and very old (≥ 85 years of age) individuals with diabetes. The aim of this study was to investigate the prevalence and determinants of anemia among older people with diabetes (≥ 75 years of age) attending a long-term follow-up in a single outpatient clinic.
Design and Methods
The setting for this cross-sectional audit was an outpatient diabetes clinic for older people (≥ 75 years of age) in a District General Hospital in the United Kingdom. The clinic is run by a geriatrician with a special interest in diabetes. Older patients attending the clinic have access to care provided by a diabetes specialist nurse, physiotherapist, occupational therapist, dietitian, and chiropodist to provide a holistic approach to patients’ needs as well as onsite vascular surgery and psychogeriatric services. The clinic runs weekly and accepts referrals from the community, other hospital-based outpatient clinics, and inpatient departments as follow-up after hospital discharge.
The study population included all patients in long-term follow-up (> 2 years) who attended the outpatient clinic during a consecutive 3-month period.
Data collection
Baseline characteristics such as age, sex, ethnic origin, comorbidities, number of medications, and social circumstances were collected during patient interviews, and laboratory results for each patient were downloaded from the central database of the pathology laboratory using patient details. To avoid acute fluctuations in the laboratory results, averages during the past 24 months were calculated. Laboratory values collected included hemoglobin (Hb) level (g/l), estimated glomerular filtration rate (eGFR; ml/min/1.73 m2 based on the Modified Diet in Renal Disease study equation),8 A1C (%), and hematinic studies such as iron profile, vitamin B12, and folic acid levels.
Anemia detection
The prevalence of anemia was determined if the average Hb level during the past 24 months was below the normal range used by the hospital laboratory (< 120 g/l for women and < 140 g/l for men).
Determinants of anemia
We examined five potential variables as determinants of anemia: older age (≥ 85 years of age), longer duration of diabetes (> 15 years), uncontrolled diabetes (A1C > 7.5%), multiple comorbidities (> 4), and presence of chronic kidney disease (CKD), defined as an eGFR < 60 ml/min/1.73 m2.
Statistical analysis
Continuous variables are presented as means and standard deviations (SDs), and categorical variables are presented as percentages. A χ2 test was used to compare categorical variables, Fisher’s exact test was used when the expected cell value was < 5, a t test was used for continuous variables, and a two-sided P of < 0.05 was considered significant. We performed an initial univariate and then a multivariate logistic regression analysis using the presence of anemia as the outcome or the dependent factor and the above-mentioned five variables individually and then in combination as the predictors. Odds ratios (ORs) and 95% confidence intervals (CIs) were used to estimate the association between outcome and variables. Statistical analysis was performed using the statistical software package Stata, version 10 (StataCorp LP, College Station, Tex.)
Study Results
Baseline characteristics
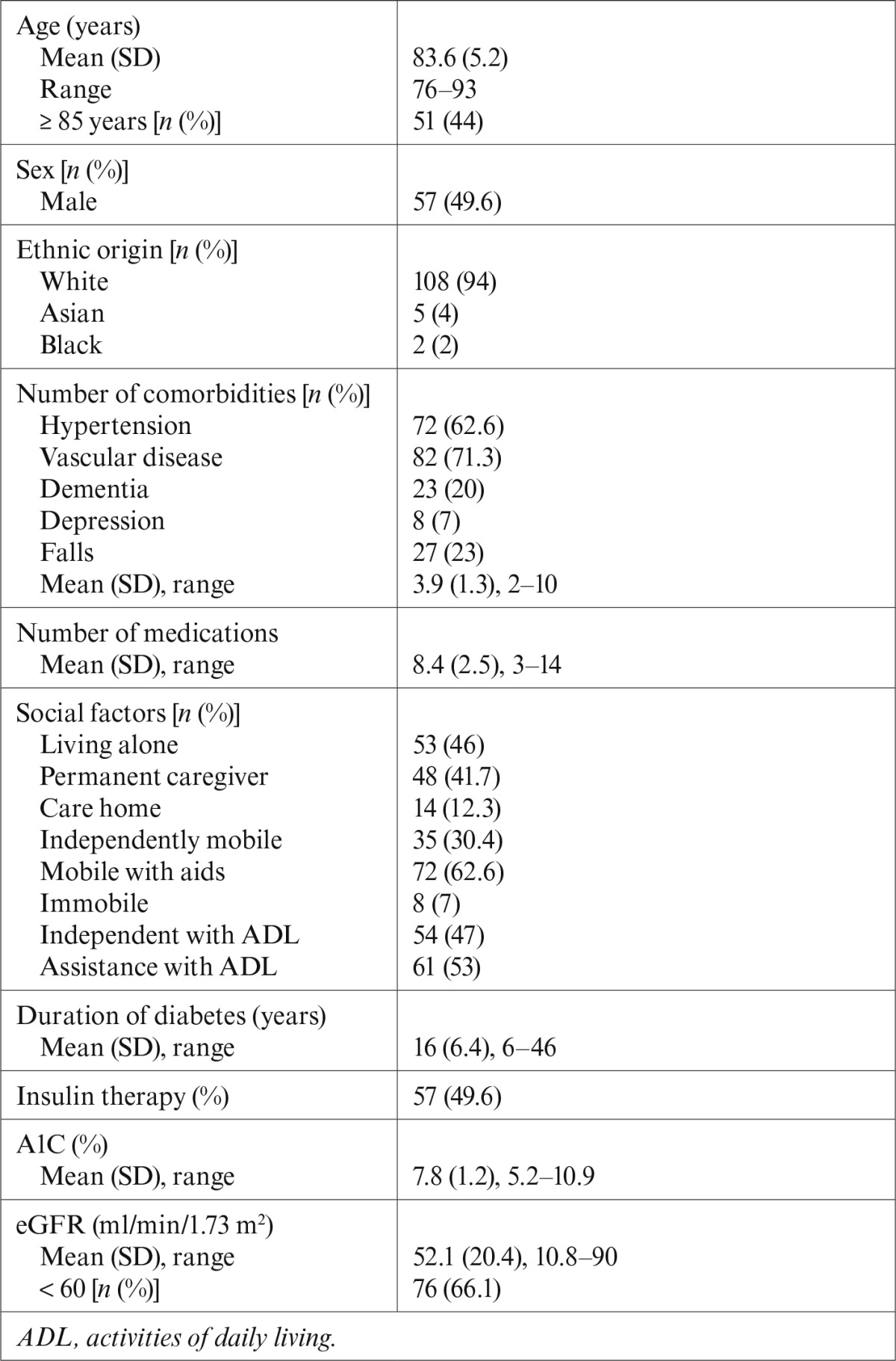
A total of 142 patients attended the outpatient clinic during the 3-month period. Twenty-seven patients had been attending the clinic for < 2 years and were excluded from the study. The remaining 115 patients had had long-term follow-up in the clinic (> 2 years) and formed the study population. Baseline characteristics are summarized in Table 1. All patients were > 75 years of age (mean age 83.6 [SD 5.2] years), and 51 (44%) were ≥ 85 years of age. Most patients (88%) lived in their own home and had a long duration of diabetes (mean duration 16.0 [SD 6.4] years). CKD was prevalent in 66.1% of patients. Three patients had a history of treated breast cancer, two had prostate cancer, and two had bowel cancer. No patients in the cohort had active or terminal cancer. Only six patients reported drinking a little alcohol socially.
Table 1.
Baseline Characteristics of All Patients (n = 115)
Prevalence of anemia
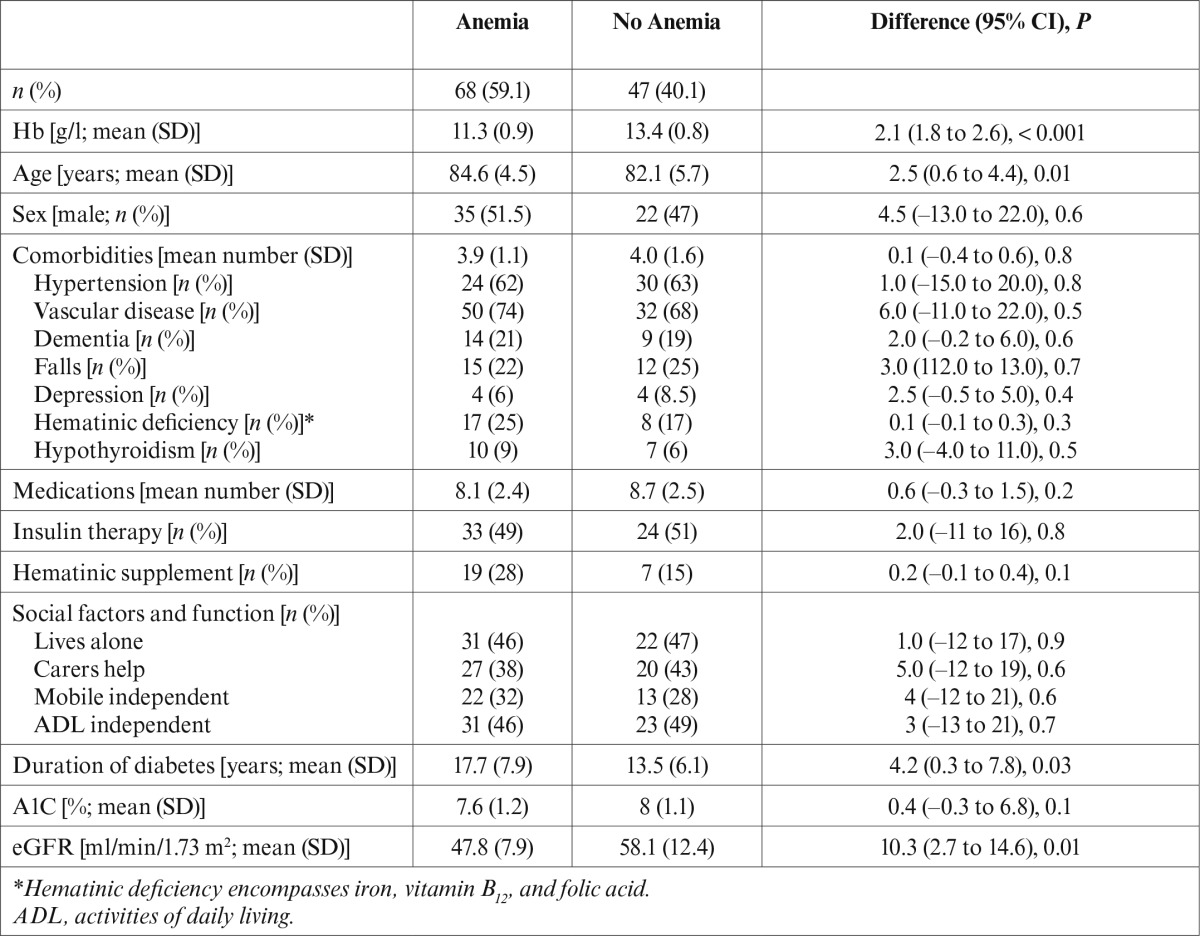
Anemia was prevalent in 68 patients (59%), of whom 35 were men and 33 were women. There was no history of hereditary anemias such as thalassemia or sickle cell disease. The majority of anemia (80%) was normocytic; anemia was microcytic in 17% and macrocytic in 3% of patients. There was no significant difference between patients with or without anemia regarding sex, number of comorbidities, number of medications, insulin therapy, hematinic therapy, social factors, or functional status (Table 2). The use of metformin, pioglitazone, angiotensin-converting enzyme (ACE) inhibitors, angiotensin receptor blockers (ARBs), or antiplatelets was similar in both groups.
Table 2.
Comparison of Patients With and Without Anemia
Determinants of anemia
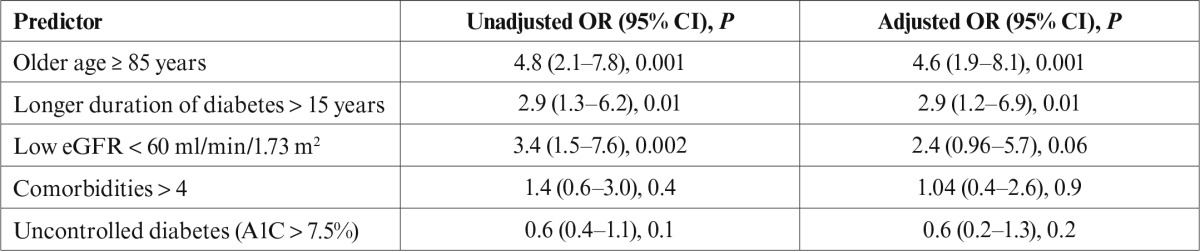
Patients with anemia were significantly older (84.6 vs. 82.1 years, P = 0.01), had a longer duration of diabetes (17.7 vs. 13.5 years, P = 0.03), and had lower eGFRs (47.8 vs. 58.1 ml/min/1.73 m2, P = 0.01) than patients without anemia. In the univariate logistic regression analysis, three of the five potential determinants significantly predicted anemia: older age ≥ 85 years (OR 4.8, 95% CI 2.1–7.8, P = 0.001), longer duration of diabetes > 15 years (OR 2.9, 95% CI 1.3–to 6.2, P = 0.01), and CKD (OR 3.4, 95% CI 1.5–7.6, P = 0.002), whereas number of comorbidities and diabetes control were not significant. However, in the multivariate logistic regression analysis, only older age (OR 4.6, 95% CI 1.9–8.1, P = 0.001) and longer duration of diabetes (OR 2.9, 95% CI 1.2–6.9, P = 0.01) remained significant, whereas the effect of CKD was reduced to borderline significance (OR 2.4, 95% CI 0.96–5.7, P = 0.06) (Table 3).
Table 3.
Univariate and Multivariate Analysis of Possible Predictors of Anemia
Discussion
This study demonstrates a higher prevalence of anemia (59%) in older people (> 75 years of age) with diabetes attending an outpatient clinic. Previous studies of a younger population (average age 65 years) with similar renal function to our population (CKD in ∼ 70% of subjects) have reported a lower prevalence (∼ 20%) of anemia in patients with diabetes, suggesting that our higher prevalence is likely to be the result of the older age of our population.2 Anemia prevalence increases with age, reaching up to 26% of the general older population (≥ 85 years of age),9 but is significantly higher in people with diabetes, reaching up to 78.6% of diabetic centenarians, confirming the contributing effect of diabetes to the prevalence of anemia.10
The cause of diabetes’ contribution to anemia development is still unclear. In the Cardiovascular Health Study,11 although diabetes predicted hemoglobin decline by –0.9 g/l (95% CI –01.8 to –0.02), it did not predict the development of anemia (OR 1.04, 95% CI 0.78–1.38), whereas baseline increasing age and CKD predicted both hemoglobin decline and anemia over a 3-year period (–1.5 g/l, 95% CI –2.4 to –0.6, and –0.9 g/l, 95% CI –1.6 to –0.3, for hemoglobin decline and 1.96, 95% CI 1.45–2.64, and 1.39, 95% CI 1.13–1.71, respectively, for anemia development). The discrepancy in the effect of diabetes causing hemoglobin decline but not leading to anemia development could be because of the short (3-year) duration of the study.
In our study, long duration of diabetes (> 15 years), CKD, and older age (≥ 85 years) were the main predictors of anemia. However, in the multiple logistic regression analysis, the effect of CKD on anemia prediction almost disappeared after adjustment for diabetes duration and older age. This suggests that CKD acts as a mediator rather than a direct cause of anemia in older people with diabetes. In other words, anemia in older people with diabetes is mainly driven by age and duration of diabetes rather than by renal function. Our population was old enough and had a long enough duration of diabetes to show this effect, which has not been seen in previous studies of younger populations.2 This may explain why the prevalence of anemia was still higher in people with diabetes than in those without diabetes who had similar renal function.12 Diabetes, independent of renal function, has recently been shown to increase the risk of anemia (OR 2.15, 95% CI 1.07–4.31).12 The results of our study question the accepted concept that anemia in diabetes is mainly caused by a decline in renal function and suggests that, in older people with diabetes, anemia is mainly related to older age and longer duration of diabetes, which may have different or additional mechanisms for anemia.
Although drug therapy such as metformin, pioglitazone, ACE inhibitors, ARBs, and antiplatelets may be associated with anemia, we did not find this association in our study.13–17 Although we did not measure nutritional status, it is unlikely that the anemia in this study was caused by chronic blood loss or nutritional deficiencies because the anemia was normochromic in the majority of patients (80%), there were no patients in our cohort suffering from chronic bowel disease, and there was no association with hematinic deficiency or hematinic supplement use.
The anemia shown in this study is likely to be related to aging and to be of unexplained etiology. This finding may explain the failure of interventions with erythropoiesis-stimulating agents to normalize hemoglobin levels in older patients with diabetes and CKD that also showed increased incidence of vascular complications and even mortality.18
Our study also suggests that anemia in this age-group of older patients with diabetes could be a marker of the severity or long duration of diabetes, especially when investigations for anemia reveal no obvious cause. Whether novel interventions to increase hemoglobin will have a role in ameliorating the adverse health outcomes of diabetes requires future studies.
Conclusion
Anemia is highly prevalent in older people with diabetes. Older age and duration of diabetes were identified as significant predictors of anemia, whereas CKD was found to act as a mediator rather than a direct cause. In some very old patients, anemia appears to be related to aging, and its etiology remains unexplained. Therefore, no treatment has been well studied. It remains to be determined whether interventions to improve hemoglobin concentration will be associated with improved function or survival.
REFERENCES
- 1.Patel KV: Epidemiology of anemia in older adults. Semin Hematol 45:210–217, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Thomas MC, MacIsaac RJ, Tsalamandris C, Molyneaux L, Goubina I, Fulcher G, Yue D, Jerums G: The burden of anaemia in type 2 diabetes and the role of nephropathy: a cross-sectional audit. Nephrol Dial Transplant 19:1792–1797, 2004 [DOI] [PubMed] [Google Scholar]
- 3.Lash AA, Coyer SM: Anemia in older adults. Medsurg Nurs 17:298–304, 2008 [PubMed] [Google Scholar]
- 4.den Elzen WP, Willems JM, Westendorp RG, de Craen AJ, Assendelft WJ, Gussekloo J: Effect of anemia and comorbidity on functional status and mortality in old age: results from the Leiden 85-Plus Study. CMAJ 181:151–157, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Riva E, Tettamanti M, Mosconi P: Association of mild anemia with hospitalization and mortality in the elderly: the Health and Anemia population-based study. Haematologica 94:22–28, 2009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Makipour S, Kanapuru B, Ershler WB: Unexplained anemia in the elderly. Semin Hematol 45:250–254, 2008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Tettamanti M, Lucca U, Gandini F, Recchia A, Mosconi P, Apolone G, Nobili A, Tallone MV, Detoma P, Giacomin A, Clerico M, Tempia P, Savoia L, Fasolo G, Ponchio L, Porta MGD, Riva E: Prevalence, incidence and types of mild anemia in the elderly: the “Health and Anemia” population-based study. Haematologia 95:1849–1856, 2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Klahr S, Levey AS, Beck GJ, Caggiula AW, Hunsicker L, Kusek JW, Striker G: The effects of dietary protein restriction and blood-pressure control on the progression of renal disease. Modification of Diet in Renal Disease Study Group. N Engl J Med 330:877–884, 1994 [DOI] [PubMed] [Google Scholar]
- 9.Guralnik JM, Eisenstaedt RS, Ferrucci L, Klein HG, Woodman RC: Prevalence of anemia in persons 65 years and older in the United States: evidence for a high rate of unexplained anemia. Blood 104:2263–2268, 2004 [DOI] [PubMed] [Google Scholar]
- 10.Davey A, Lele U, Elias MF, Dore GA, Siegler IC, Johnson MA, Hausman DB, Tenover JL, Poon LW: Diabetes mellitus in centenarians. J Am Geriatr Soc 60:468–473, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Zakai NA, French B, Arnold AM, Newman AB, Fried LF, Robbins J, Chaves P, Cushman M: Hemoglobin decline, function, and mortality in the elderly: the Cardiovascular Health Study. Am J Hematol 88:5–9, 2013 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Chagai G, Dovrish Z, Nira KM, Bornstein G, Leibowitzet A: Diabetes mellitus with normal renal function is associated with anemia. Diabetes Metab Res Rev 30:291–296, 2014 [DOI] [PubMed] [Google Scholar]
- 13.Liu KW, Dai DLK, Ho W, Lau E, Woo J: Metformin-associated vitamin B12 deficiency in the elderly. Asian J Gerontol Geriatr 6:82–87, 2011 [Google Scholar]
- 14.Berria R, Glass L, Mahankali A, Miyazaki Y, Monroy A, De Filippis E, Cusi K, Cersosimo E, DeFronzo RA, Gastaldelli A: Reduction in hematocrit and hemoglobin following pioglitazone treatment is not hemodilutional in type II diabetes mellitus. Clin Pharmacol Ther 82:275–281, 2007 [DOI] [PubMed] [Google Scholar]
- 15.Leshem-Rubinow E, Steinvil A, Zeltser D, Berliner S, Rogowski O, Chodick G, Shalev V: Association of angiotensin-converting enzyme inhibitor therapy initiation with a reduction in hemoglobin levels in patients without renal failure. Mayo Clin Proc 87:1189–1195, 2012 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Mohanram A, Zhang Z, Shahinfar S, Lyle PA, Toto RD: The effect of losartan on hemoglobin concentration and renal outcome in diabetic nephropathy of type 2 diabetes. Kidney Int 73:630–636, 2008 [DOI] [PubMed] [Google Scholar]
- 17.Hammerman-Rozenberg R, Jacobs JM, Azoulay D, Stessman J: Aspirin prophylaxis and the prevalence of anaemia. Age Ageing 35:514–517, 2006 [DOI] [PubMed] [Google Scholar]
- 18.Singh AK, Szczech L, Tang KL, Barnhart H, Sapp S, Wolfson M, Reddan D: Correction of anemia with epoetin alfa in chronic kidney disease. N Engl J Med 355:2085–2098, 2006 [DOI] [PubMed] [Google Scholar]