

Abstract
This study examined the convergence and divergence in mothers’ and children’s reports of maternal support following disclosures of childhood sexual abuse (CSA). One hundred and twenty mothers and their children (ages 7 to 17 years) reported on two aspects of support following CSA disclosures: mothers’ belief in the child’s disclosure and parent-child discussion of the abuse incident. Whereas 62% of mothers’ and children’s reports on mothers’ belief of the disclosure positively converged (i.e., both reported that mothers “completely believed” the child’s disclosure), 37% of mothers’ and children’s reports diverged, and the remaining 1% negatively converged (i.e., both reported that the mother only believed the child “somewhat”). Positively convergent responses were associated with youths’ lower risk for tobacco and illicit drug use. Forty four percent of mothers’ and children’s reports on whether details of the CSA were discussed positively converged (i.e., both reported that details were discussed), 33% diverged, and 23% negatively converged (i.e., both reported that details were not discussed). Relative to other patterns of reporting, negatively convergent responses were associated with higher levels of trauma symptoms. Findings have implications for identifying high-risk mother-child dyads based on patterns of informant reporting following CSA.
Keywords: Childhood Sexual Abuse, Maternal Support, Parent-Child Report
Maternal support is a strong predictor of children’s recovery and healthy development following CSA disclosures (Everson, Hunter, Runyon, Edelsohn, & Coulter, 1991; Fromuth, 1986; Johnson & Kenkel, 1991; Spaccarelli & Kim, 1995; Tremblay, Hébert, & Piché, 2000). In fact, maternal support is more predictive of children’s outcomes than the actual characteristics of the abuse, including the type or duration of the abuse or the child’s relationship with the perpetrator (Deblinger, Steer, & Lippmann, 1999; Everson et al., 1991; Fromuth, 1986; Johnson & Kenkel, 1991; Spaccarelli & Kim, 1995; Tremblay et al., 2000). Parents and children often differ in their perceptions of the quality and amount of maternal support provided following CSA disclosures (Bolen, 1998; Bolen & Lamb, 2007; Deblinger et al., 1999; Morrison & Clavenna-Vallerroy, 1998). However, to our knowledge, the actual convergence or divergence in parent-child perceptions of maternal support following CSA has not been systematically examined. The current study adopts methods for detecting informant discrepancies from the larger body of literature on child mental health and psychosocial adjustment (i.e., Chi & Hinshaw, 2002; De Los Reyes, Goodman, Kliewer, & Reid-Quiñones, 2010). In this study, we investigated the prevalence of convergent and divergent ratings of maternal support following CSA disclosure and the degree to which they predicted youth psychosocial functioning.
Maternal Support following CSA Disclosure
Converging evidence suggests that maternal support following CSA disclosure is critical for children’s healthy psychosocial adjustment (Conte & Schuerman, 1987; Elliot & Carnes, 2001; Kendall-Tackett, Williams, & Finkelhor, 1993; Paredes, Leifer, & Kilbane, 2001; Tufts New England Medical Center, 1984). CSA victims who receive high levels of maternal support following CSA disclosure respond more adaptively to stress (Esparza, 1993), exhibit fewer sexual behavior problems (Adams-Tucker, 1982; Friedrich, Urquiza, & Beilke, 1986; Liefer et al., 1993), show lower internalizing and externalizing symptoms (Bolen & Lamb, 2007; Deblinger et al., 1999; Feiring, Coates, & Taska, 2001; Gold, Milan, Mayall, & Johnson, 1994; Gries et al., 2000), and are less likely to engage in cigarette smoking or drug use (Chen, Tyler, Whitbeck, & Hoyt, 2000; Hadland et al., 2012), than youth who receive insufficient support. Parental support following CSA is not only critical for optimal psychosocial development during childhood and adolescence, but has also been associated with interpersonal adjustment in adulthood (Adams & Bukowski, 2007; Liang, Williams, & Siegel, 2006).
Informant Convergence and Divergence in Reports of Maternal Support
Assessments of maternal support following CSA typically rely on either mother or child reports. However, there are often significant discrepancies in mother’s and children’s reports of maternal support following CSA (Bolen & Lamb, 2007; Deblinger et al., 1999; Johnson & Kenkel, 1991; Spacarelli & Fuchs, 1997). In past studies, mothers’ and children’s independent reports have predicted different aspects of children’s adjustment following CSA disclosure (Avery, Massat, & Lundy, 1998; Esparza, 1998; Morrison & Clavenna-Valleroy, 1998). A large body of literature on child adjustment suggests that divergence in parent and child reports of parental behavior is clinically meaningful. Discordance in ratings of parental monitoring and discipline have been associated with children’s heightened risk for internalizing problems (Gaylord, Kitzmann, & Coleman, 2003; Guion, Mrug, & Windle, 2009), poor social competence (Carlson, Cooper, & Spradling, 1991; Guion et al., 2009), and delinquency (De Los Reyes et al., 2010). Discrepancies in parents’ and children’s reports of parental quality, warmth, and family functioning have also been associated with both internalizing and externalizing problems in children (Feinberg, Howe, Reiss, & Hetherington, 2000; Guion et al., 2009; Ohannessian, Lerner, Lerner, & von Eye, 2000) and adolescents (Pelton & Forehand, 2001; Pelton, Steele, Chance, & Forehand, 2001). In addition to representing normative parent-child reporting differences, these discrepancies are considered reflective of problematic parent-child communication patterns, attachment relationship quality, and family conflict or dysfunction (Barker, Bornstein, Putnick, Hendricks, & Suwalsky, 2007; Ehrlich, Cassidy, & Dykas, 2011; Feinberg et al., 2000; Ferdinand, van der Ende, & Verhulst, 2004; Gaylord et al., 2003, Grills & Ollendick, 2003; Welsh, Galliher, & Powers, 1998). Furthermore, many consider parent-child reporting discrepancies as useful for predicting children’s risk for maladjustment and for guiding treatment (Feinberg et al., 2000; Guion et al., 2009; Mounts, 2007).
Current Study
Taking into account convergence and divergence in reports of maternal support at the time of CSA disclosure may offer a useful preliminary index of parent-child relationship quality and risk for child maladjustment following CSA. The current study examined the prevalence and predictive value of mother-child convergence and divergence of two forms of post-disclosure-related support among victims of CSA. The first form of support concerned mothers’ belief in the child’s disclosure. The second concerned mother-child discussion of the abuse incident following the disclosure. We also examined whether patterns of convergence and divergence in these aspects of maternal support were associated with children’s psychosocial adjustment. We hypothesized that mothers and children whose reports positively converged (i.e., when both informants reported that mothers believed the child’s disclosure and/or that details were discussed) would show more positive psychosocial adjustment (i.e., fewer post-disclosure trauma symptoms and lower frequency of substance use) than dyads whose reports diverged or whose reports negatively converged (i.e., when both informants reported that support was non-optimal).
Method
Participants
Participants were 120 children and mothers (or female guardians) who resided in the south-eastern region of the United States and who were evaluated at a child advocacy center (CAC) following reports of CSA. Inclusion criteria were that: a) children were 7–17 years old; b) children were victims of sexual abuse involving physical contact (e.g., fondling, penetration) as determined by a professionally-conducted forensic evaluation; and c) mothers were not complicit or involved in the sexual abuse (i.e., “non-offending”) as determined by the forensic examiner. Exclusion criteria included psychotic behavior during the forensic evaluation, significant cognitive disability or mental retardation, or inability to speak Spanish or English; however, no cases were excluded based on these criteria.
Participants were recruited over a 3-year period from a CAC as part of a first time forensic assessment following reports of CSA (see Figure 1 for recruitment details). Prior to the onset of study recruitment, all procedures were approved by the Institutional Review Board at the [NAME OF UNIVERSITY DELETED FOR BLIND REVIEW] and by the Human Research Committee of the CAC. To recruit families, trained female research staff approached all parents and children who presented for a forensic assessment during this 3.5 year period. Parents provided consent to be contacted by phone to hear about research opportunities. Families who were determined to meet eligibility criteria, based on a review of CAC records, were contacted by phone and invited to participate. An in-person research visit at the CAC was scheduled for families who expressed interest. Female graduate students in counseling programs and doctoral-level psychologists conducted all assessments. Assessments for mothers and children were conducted separately.
Figure 1.
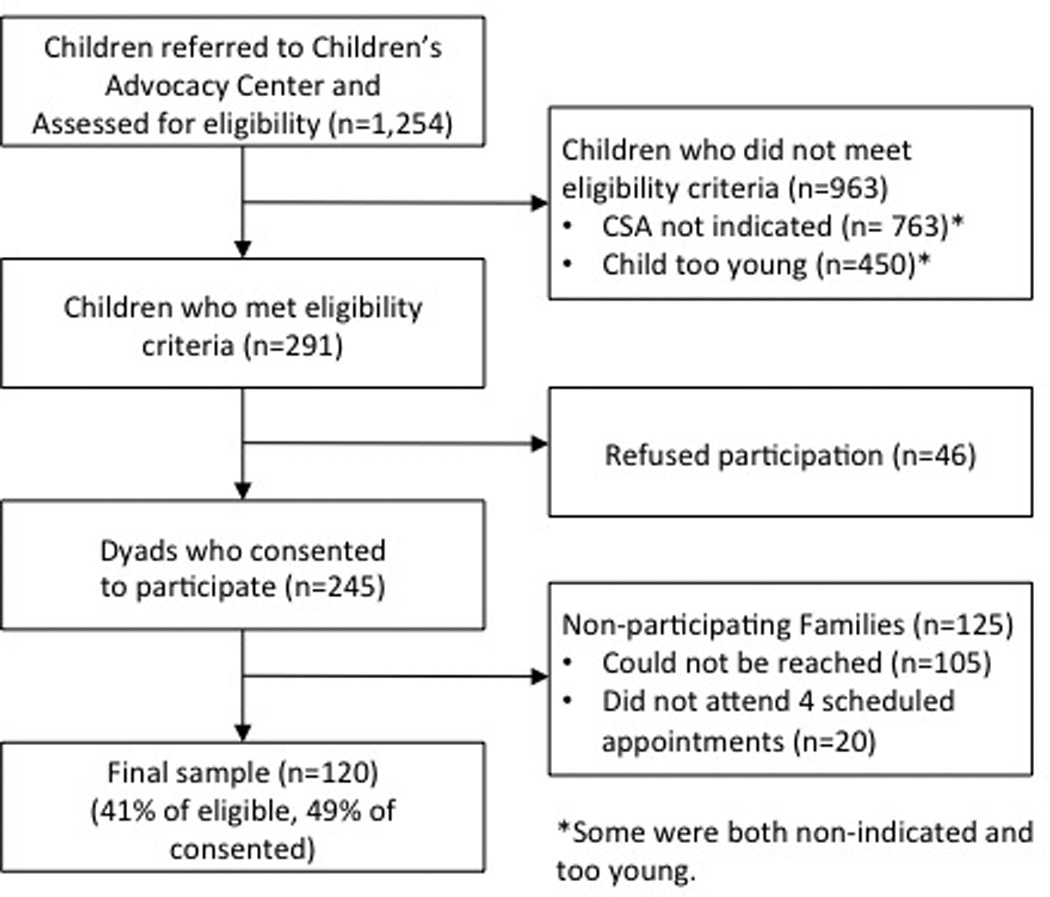
Recruitment of final sample from child advocacy center following reports of CSA
Of the final sample of 120 children, 85% (n = 102) were female, with an average age of 11.57 years (SD = 2.69, range 7–17 years). With regard to racial and ethnic composition, 42% of the children were African American, 56% were White, and 2% were biracial. Eighty-six percent of the caregivers were biological mothers, 12% were kinship caregivers, 1% were adoptive mothers, and 1% were step-mothers. Of caregivers, 42% were African American, 57% were White, and 1% were classified as “other”. Caregivers ranged in age from 24 to 67 years with an average age of 38.4 years (SD = 9.0 years). Eighteen percent of the caregivers reported a yearly income of less than $10,000, 27% reported a yearly income between $10–20,000, 17% reported an income between $21–30,000, 9% reported an income of $31–40,000, 9% reported an income of $41–50,000, and 20% reported an income of more than $50,000. With regard to marital status, 53% of the caregivers were married or living with a partner, 19% were single, 26% were divorced or separated, and 2% were widowed. In terms of educational status, 22% of the caregivers did not complete high school, 30% graduated from high school, 34% received an associates degree or attended some college, 10% graduated from college, and 4% received a graduate degree.
Measures
Structured Clinical Interviews
A structured interview was used to ask children about their sexual and physical abuse history, exposure to inter-parental violence, family relationships, legal and child protective service involvements, previous and current mental health treatment, and demographic information (Nugent, Saunders, Williams, Hanson, Smith, & Fitzgerald, 2009). Mothers were asked about their family history, their own exposure to sexual and physical assault, the reported CSA incident, social service intervention, and demographic information. Mothers and children were interviewed separately.
Illicit Drug Use
A structured clinical interview was used to ask children about their drug use following the CSA. Specifically, children were asked, “Since the abuse, have you tried: cigarette smoking, smokeless tobacco (i.e., chewing tobacco or snuff), alcohol (i.e., beer, wine, liquor, or any other alcoholic beverage), prescription medication but without a doctor’s prescription, or street drugs (i.e., drugs that are not prescribed by a doctor and are not used for medical purposes)?” Children responded “yes” or “no” to each question. Two scores were calculated for analyses. The first was whether or not youth engaged in tobacco use (cigarette smoking or any form of smokeless tobacco) since their disclosure. The second was the number of illicit drugs (alcohol, prescription medications, street drugs) tried since their disclosure.
Maternal Support Following CSA Disclosure
Mothers and children were asked about the mother’s response to the child’s CSA disclosure. Specifically, mothers were asked, “When you first learned about the abuse, did you believe that it happened as described?” Mothers had the option of responding “no,” “somewhat,” or “completely.” Children were asked, “How much did your mom believe the abuse happened?” Children had the option of responding, “my mother did not believe me at all”, “my mother believed me somewhat”, or “my mother believed me completely”. Response patterns were classified as positively convergent if both the mother and child reported that the mother “believed the child completely” and negatively convergent if both the mother and child reported that the mother believed the child “somewhat,” or both reported that the mother did not believe the child “at all”. Responses were identified as divergent if mothers’ and children’s responses conflicted on whether mothers believed the child’s disclosure.
Next, mothers and children were asked whether they talked about the abuse incident with each other following the disclosure. Specifically, mothers were asked, “Have you ever, at any time, talked with your child about the details of what happened?”. Children were asked, “Have you ever, at any time, talked with your mother about the details of what happened?”. Mothers and children responded “yes” or “no” to this question. Responses were classified as positively convergent if they both responded “yes” and negatively convergent if they both responded “no.” Responses were classified as divergent if mothers and children responded with conflicting reports.
Trauma Symptom Checklist for Children (TSCC)
The TSCC (Briere, 1996) was developed as a parent report instrument for assessing children’s trauma-related symptoms. This instrument has been validated for children ranging in age from 8 to 16 years. From the fifty-four items, six scales are calculated including children’s anxiety, depression, anger, posttraumatic stress, dissociation, and sexual concerns. In addition to these six scales, two validity scales are calculated to reveal patterns of hyper- or hypo-responding. Past research has indicated adequate internal consistency and validity of the measure (Briere, 1996; Crouch, Smith, Ezzell, & Saunders, 1999).
Results
Prevalence of Convergence and Divergence in Reports of Maternal Support
First, we examined convergence and divergence in mothers’ and children’s reports of whether the mother believed the CSA disclosure. Of the 120 participants, data were missing for 36 children and 5 mothers; this was mostly due to participant refusal, except for two mothers and two children who reported that they were “unsure”. Missing data on this variable were not associated with child age, gender, severity of abuse experience, reports of trauma symptoms on the TSCC, cigarette use, or illicit drug use (all p-values > .05).
Convergence and divergence in reports was examined on the 71 remaining dyads: 62% (n = 44) of reports on whether mothers believed the child’s disclosure were positively convergent, and 4% (n = 3) were negatively convergent. In all three cases of negative convergence, mothers and children reported that the mother believed the child “somewhat”. No dyads both reported that the child’s disclosure was not believed “at all”. The remaining 34% of dyads (n = 24) varied in the manner in which their reports diverged. In the majority of cases, children reported that their mothers “completely” believed their disclosures whereas mothers reported that they only “somewhat” believed (n = 13) or did not believe their child’s disclosure “at all” (n = 5). In two cases, children reported that their mothers only “somewhat” believed them, while mothers reported that they “completely” believed their child’s disclosure. In four cases, children reported that their mothers “somewhat” believed their disclosures, while mothers reported that they did not believe their child’s disclosure “at all.”
Next we examined convergence and divergence in reports on whether details of the CSA incident were discussed. Data were missing for 3 children and 3 mothers on this item; response patterns were examined in the remaining 114 cases. Missing data were not associated with any demographic or outcome variable. On this item, 44% (n = 50) positively converged, and 23% (n = 26) negatively converged. Of the 33% of mothers and children whose responses diverged, 53% (n = 20) of mothers reported that they discussed the details of the abuse incident while their child reported that details of the abuse incident were not discussed, and 47% (n = 18) reported that details were not discussed while their child reported that details of the abuse incident were discussed.
Associations between discrepancies in reporting and child psychosocial functioning
Because CSA severity has been predictive of child outcomes (Browne & Finkelhorne, 1986), abuse severity (as indicated by the presence of a penetration sexual assault; Senn, Carey, Vanable, Coury-Doniger, & Urban, 2007) was included as a covariate in primary analyses. Due to the broad age range of youth in this sample, we explored whether child age moderated associations between mother-child reports of support following CSA and child functioning. The matrix of inter-correlations of the covariates, independent variables, and dependent variables is presented in Table 1.
Table 1.
Zero-order Correlations between Child Age, Gender, Abuse Severity, Maternal Support Discrepancies, and Psycho-social Functioning
| age | gen | sev | bel | det | anx | dep | ang | ptsd | diss | sex | tob | drug | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| age | 1 | - | - | - | - | - | - | - | - | - | - | - | |
| gen | .045 | 1 | - | - | - | - | - | - | - | - | - | - | |
| sev | .174 | −.049 | 1 | - | - | - | - | - | - | - | - | - | |
| bel | −.068 | .052 | .033 | 1 | - | - | - | - | - | - | - | - | |
| det | −.176 | −.167 | −.236* | −.008 | 1 | - | - | - | - | - | - | - | |
| anx | −.089 | .100 | .186* | −.032 | −.194* | 1 | - | - | - | - | - | - | |
| dep | −.016 | .193* | .067 | −.073 | −.181 | .656** | 1 | - | - | - | - | - | |
| ang | .146 | .193* | .040 | .032 | −.195* | .568** | .663** | 1 | - | - | - | - | |
| ptsd | −.008 | .041 | .157 | −.171 | −.220* | .813** | .667** | .535** | 1 | - | - | - | |
| diss | .039 | .103 | .180 | −.037 | −.204* | .708** | .706** | .693** | .753** | 1 | - | - | |
| sex | .106 | .098 | .300** | −.016 | −.248** | .517** | .501** | .481** | .508** | .475** | 1 | ||
| tob | .496** | .222* | .028 | −.197 | −.073 | .203* | .259** | .457** | .181* | .240** | .202* | 1 | - |
| drug | .416** | .104 | .090 | −.107 | .121 | .149 | .271** | .346** | .226* | .336** | .164 | .559** | 1 |
Note: age = child age at assessment; gen = child gender; sev = severity of abuse; bel = discrepancies in reports of whether mothers believed disclosure; det = discrepancies in reports on whether details of abuse were discussed; anx = TSCC ratings of anxiety; dep = TSCC ratings of depression; ang = TSCC ratings of anger; ptsd = TSCC ratings of post traumatic stress; diss = TSCC ratings of dissociation; sex = TSCC ratings of sexual concerns; tob = child use of tobacco products drug = child number of illicit drugs used
p < .05;
p < .001.
First we examined whether convergence and divergence in reports of mothers’ belief in the child’s disclosure was associated with the child’s substance use and mental health functioning. Given insufficient power to detect significant differences between all permutations of divergence, we compared mothers and children whose reports positively converged (i.e., both reported that the mother “completely believed” the child’s disclosure) to all other patterns of responses.
Results of analyses indicated significant associations between patterns of reporting of mothers’ belief in the disclosure and youth’s tobacco use, OR = .28 [95% CI = .08–.93] and illicit drug use F (1, 66) = 7.16, p < .01. When reports were positively convergent, children were less likely to have tried cigarettes or engage in illicit drug use following the abuse, compared to cases that diverged or were negatively concordant (see Figure 1). Patterns of reporting on whether mothers believed in the child’s CSA reporting was not significantly associated with youth trauma symptoms. Child age did not significantly interact with reports of mothers’ belief in the disclosure to predict tobacco or illicit drug use.
Next, we examined associations between convergent and divergent response patterns regarding discussion of the abuse incident and children’s substance use and mental health functioning. Results of a MANOVA, with age included as a between-subjects variable, revealed a significant main effect of patterns of reporting on child mental health symptoms, including anxiety, F (3, 112) = 3.82, p < .05, depression, F (3, 112) = 2.75, p < .05, trauma symptoms, F (3, 112) = 3.5, p < .05, dissociation, F (3, 112) = 3.96, p < .05, and sexual concerns F (3, 112) = 3.54, p < .05. A marginally significant association was found in association with children’s anger symptoms, F (3, 112) = 2.52, p < .10. Post hoc comparison tests revealed that anxiety, trauma symptoms, and dissociation were significantly elevated when patterns of reporting were negatively convergent, relative to divergent and positively convergent response patterns. Child depression, anger, and sexual concerns were significantly elevated in negatively convergent cases relative both to positively convergent cases and to divergent cases in which mothers reported that details were discussed while children reported that details were not discussed (see Figure 2).
Figure 2. Convergence and divergence in reports of whether mothers believed children’s disclosures as associated with child reports of illicit drug use.
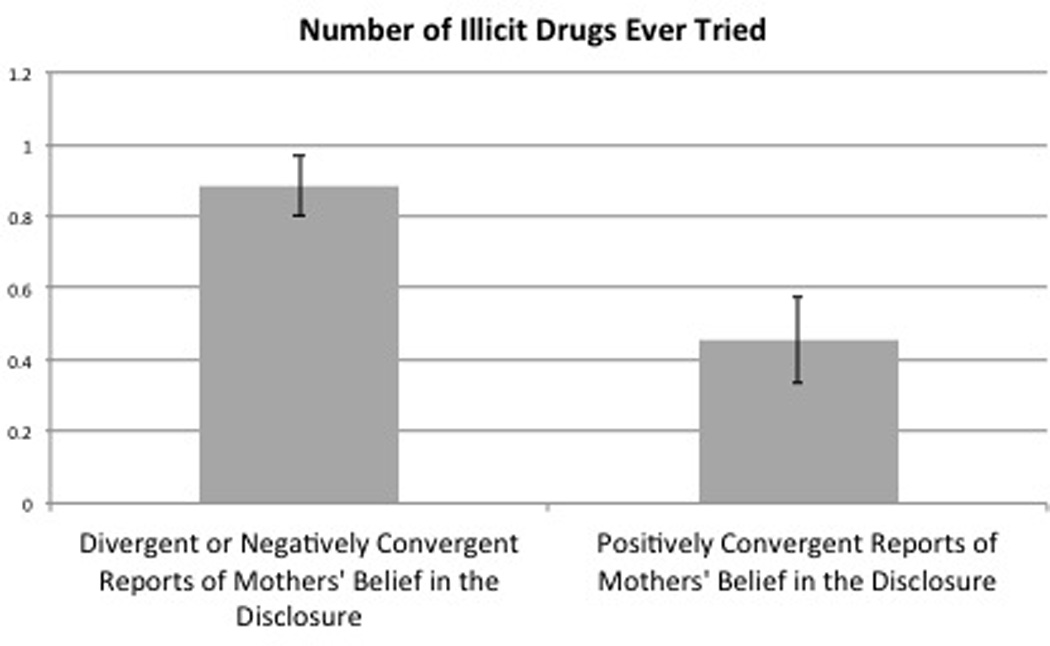
Positively convergent reports of whether mothers believed the child’s disclosure (i.e., when both mothers and children reported that mothers believed the child’s disclosure) were associated with lower risk for illicit drug use than divergent reports (i.e., when mothers’ and children’s reports of whether the mother believed the child’s disclosure conflicted) or negatively convergent reports (when mothers and children reported that the disclosure was believed “somewhat”.)
In most cases, youth trauma symptoms were not significantly different in positively convergence versus divergent cases, except for symptoms of depression. Children’s depression symptoms were higher in divergent cases (in which mothers reported that details were not discussed while children reported that they were discussed) compared to cases in which response patterns positively converged (see Figure 2). Child age did not significantly interact with associations between parent-child response patterns and trauma symptoms. Convergence and divergence in mothers’ and children’s reports of whether details were discussed were not associated with tobacco or illicit drug use.
Discussion
Though past studies have indicated that maternal support following CSA disclosure predicts children’s recovery and overall adjustment, few studies have examined the convergence or divergence in mothers and children’s reports of maternal support. The current study investigated rates of convergence and divergence in mothers’ and children’s reporting of two domains of maternal support. The first concerned maternal belief in the child’s disclosure and the second concerned mother-child discussion about the abuse following the disclosure. Next, these patterns of reporting were examined in association with children’s psychosocial functioning.
Results of this study revealed significant heterogeneity in response patterns of the two aspects of maternal support following CSA disclosure. In terms of mothers’ belief in the child’s disclosure, more than half of mothers’ and children’s responses positively converged (both mothers and children reported that mothers believed the child’s disclosure). In the remaining cases, the majority of response patterns diverged. Interestingly, very few cases were negatively convergent; those that diverged were cases in which both mothers and children reported that mothers believed the disclosure “somewhat.” In this sample, no mothers and children converged in reporting that mothers didn’t believe the child’s disclosure “at all”.
In terms of convergence and divergence in reports of whether details were discussed, less than half of mothers’ and children’s reports positively converged (i.e., both mothers and children reported that details of the abuse were discussed), and about one fifth of dyads’ reports negatively converged. Around one third of all cases were divergent, with an approximately equal distribution of cases in which mothers reported that details were discussed while the child reported the opposite, and visa versa.
Consistent with expectations, variability in response patterns predicted youth psychosocial functioning following CSA disclosure. Youth were at lower risk for reporting tobacco and drug use when mothers’ and children’s reports of mothers’ belief of the disclosure positively converged. Further, youth were at highest risk for all trauma symptoms when both mothers’ and children’s reports on whether they discussed the abuse incident negatively converged. For some symptoms (anxiety, PTSD, and dissociation), levels were higher in cases of negatively convergent responses versus all other forms of reporting. For others (depression, anger, and sexual concerns), levels were higher in cases of negatively convergent responses relative only to cases of positively convergent responses and specific divergent responses (but only those characterized by mothers reporting that details were discussed while children reported that details were not discussed). Contrary to expectations, divergent responses, as a whole, did not predict higher risk for mental health problems. However, specific forms of divergence, in which mothers reported that details were not discussed while children reported that they were discussed, tended to place children at higher risk for depressive symptoms, in comparison to positively convergent responses.
Given our limited sample size in analyses involving mothers’ belief in the child’s disclosure, we were not able to examine the individual contribution of each permutation of mother-child divergence. However, we had more power to do so in our examinations of mothers’ and children’s reports of whether they discussed details of the abuse. Results of these analyses revealed that the direction of the divergence may be clinically meaningful. Somewhat surprisingly, children were more at risk for problematic outcomes when they reported optimal levels of support while their mothers report non-optimal levels of support. This may result from compromises in caregiving that may be more common among mothers who report that they do not believe their child’s disclosure, even when the child perceives otherwise. This “maternal disbelief” may override the protective factor associated with youth’s perceiving that their disclosure was believed. Future work investigating caregiving dynamics associated with divergent perceptions of support may shed light on this issue.
Findings support prior literature suggesting that variability on parent versus child reporting on parenting behavior is related to poor behavioral and mental health outcomes for children (e.g., De Los Reyes, 2010; Guion et al., 2009). An exciting implication of this study is the relevance for treatment efforts designed to facilitate children’s recovery from CSA. Consideration of whether reports of support positively converge, negatively converge, or diverge following disclosures of CSA may be useful in identifying children at highest risk for maladjustment following CSA. Attending to these nuances may improve screening techniques that identify children and parents who need more support to facilitate optimal recovery from CSA. Further, comparing mothers and children’s response patterns may supplement existing evidence-based treatment techniques that encourage parent-child communication about CSA (e.g., Trauma-Focused Cognitive-Behavior Therapy; Cohen, Mannarino, & Deblinger, 2006).
Despite these implications, the current findings should be interpreted within the context of several limitations, one of which is the cross sectional design of the study. As such, we cannot conclude that drug use and mental health problems were a consequence of CSA or of mothers and children diverging in their perceptions of maternal support following CSA. It is possible that children who exhibit higher trauma symptoms or substance use are less likely to have supportive relationships with their parents in general, especially following a traumatic incident. Further, this investigation only examined two of several domains of maternal support following CSA identified in prior work. Additional domains of maternal support (i.e., providing ongoing emotional support, protecting the child from perpetrator or other threats to safety, offering professional services; Everson et al., 1991; Johnson & Kenkel, 1991; Morisson & Clavenna Valleroy, 1998; Morrow & Sorell, 1989; Waterman, Kelly, Oliveri, & McCord, 1993) should be considered in future investigations.
Mothers and children who participated in this study may represent a unique sample of children who are victims of CSA. Dyads were among those who received an assessment at a CAC. Therefore, these findings do not generalize to a potentially higher risk group of children who do not disclose CSA to caregivers or who do disclose CSA but are not brought in for an assessment at a CAC. Our sample included mostly female children age seven years and older; therefore, it will be important to examine whether these effects replicate in a younger sample of youth, and whether these effects depend on the child’s gender. While our focus here was on convergence in children’s and non-offending mothers’ reports of responses to disclosure, it may also be important to consider additional support figures, such as fathers, secondary caregivers, relatives, or members of the community, who may also facilitate children’s recovery from CSA.
Despite these limitations, the results from the current study have important implications for predicting which youth are at highest risk for maladjustment following CSA. Assessing the convergence or divergence of reports may be instrumental in designing intervention programs that aim to improve communication patterns between parents and children as part of CSA treatment. In summary, these findings are a first step in understanding how convergence and divergence in reporting of parental support following disclosures may predict children’s and families’ recovery from the trauma of CSA.
Figure 3. Convergence and divergence in reports of whether mothers and children discussed details of abuse as associated with children’s mental health symptoms.
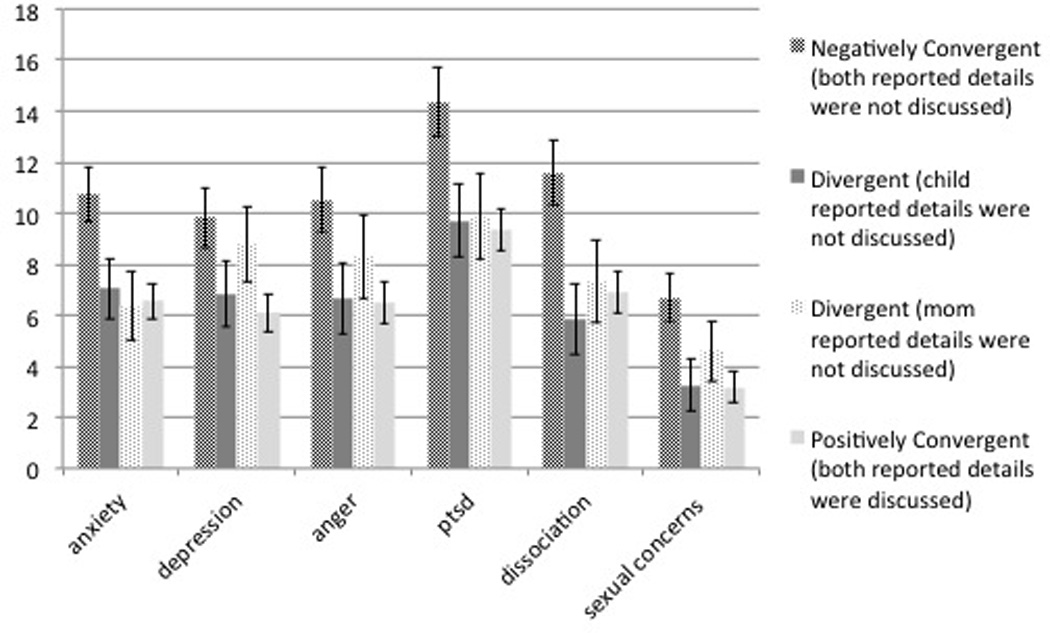
Negatively convergent responses (i.e., when both mothers and children reported that details were discussed) were associated with lowest risk for all symptoms than positively convergent responses (i.e., when both mothers and children reported that details were discussed). Depression symptoms were higher when reports diverged than when reports positively converged, but only for cases in which mothers reported that details were not discussed, while children reported that details were discussed.
Acknowledgements
Preparation of this manuscript was supported by T32 MH018869 (Dean G. Kilpatrick, PI). The original research was supported by funding from the US Department of Health and Human Services Administration on Children and Families (Daniel W. Smith, PI).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Adams RE, Bukowski WM. Relationships with mothers and peers moderate the association between childhood sexual abuse and anxiety disorders. Child Abuse and Neglect. 2007;31(6):645–656. doi: 10.1016/j.chiabu.2006.12.011. [DOI] [PubMed] [Google Scholar]
- Adams-Tucker C. Proximate effects of sexual abuse in childhood: A report on 28 children. The American Journal of Psychiatry. 1982;139:1252–1256. doi: 10.1176/ajp.139.10.1252. [DOI] [PubMed] [Google Scholar]
- Avery L, Massat C, Lundy M. The relationship between parent and child reports of parental supportiveness and psychopathology of sexually abused children. Child & Adolescent Social Work Journal. 1998;15:187–205. [Google Scholar]
- Barker ET, Bornstein MH, Putnick DL, Hendricks C, Suwalsky JD. Adolescent-mother agreement about adolescent problem behaviors: Direction and predictors of disagreement. Journal of Youth and Adolescence. 2007;36:950–962. [Google Scholar]
- Bolen RM. Predicting risk to be sexually abused: A comparison of logistic regression to event history analysis. Child Maltreatment. 1998;3:157–170. [Google Scholar]
- Bolen RM, Lamb JL. Parental support and outcome in sexually abused children. Journal of Child Sexual Abuse: Research, Treatment, & Program Innovations for Victims, Survivors, & Offenders. 2007;16:33–54. doi: 10.1300/J070v16n02_03. [DOI] [PubMed] [Google Scholar]
- Briere J. Trauma Symptom Checklist for Children. Odessa, Fl: Psychological Assessment Resources; 1996. [Google Scholar]
- Browne A, Finkelhorne D. Impact of child sexual abuse: A review of the research. Psychological Bulletin. 1986;99:66–77. [PubMed] [Google Scholar]
- Carlson CI, Cooper CR, Spradling VY. Developmental implications of shared versus distinct perceptions of the family in early adolescence. New Directions for Child Development. 1991;51:5113–5132. [Google Scholar]
- Chen X, Tyler KA, Whitbeck LB, Hoyt DR. Early Sexual Abuse, Street Adversity, and Drug Use Among Female Homeless and Runaway Adolescents in the Midwest. Journal Of Drug Issues. 2004;34(1):1–21. [Google Scholar]
- Chi TC, Hinshaw SP. Mother-child relationships of children with ADHD: The role of maternal depressive symptoms and depression-related distortions. Journal Of Abnormal Child Psychology: An Official Publication Of The International Society For Research In Child And Adolescent Psychopathology. 2002;30:387–400. doi: 10.1023/a:1015770025043. [DOI] [PubMed] [Google Scholar]
- Cohen JA, Mannarino AP, Deblinger E. Treating Trauma and Traumatic Grief in Children and Adolescents. New York: The Guilford Press; 2006. [Google Scholar]
- Conte JR, Schuerman JR. Factors associated with an increased impact of child sexual abuse. Child Abuse & Neglect. 1987;11:201–211. doi: 10.1016/0145-2134(87)90059-7. [DOI] [PubMed] [Google Scholar]
- Conte JR, Schuerman JR. The effects of sexual abuse on children: A multidimensional view. Journal Of Interpersonal Violence. 1987;2(4):380–390. [Google Scholar]
- Crouch JL, Smith DW, Ezzell CE, Saunders BE. Measuring reactions to sexual trauma among children: Comparing the children's impact of traumatic events scale and the trauma symptom checklist for children. Child Maltreatment. 1999;4:255–263. [Google Scholar]
- Deblinger E, Steer RA, Lippmann J. Two-year follow-up study of cognitive behavioral therapy for sexually abused children suffering post-traumatic stress symptoms. Child Abuse & Neglect. 1999;23:1371–1378. doi: 10.1016/s0145-2134(99)00091-5. [DOI] [PubMed] [Google Scholar]
- De Los Reyes A, Goodman KL, Kliewer W, Reid-Quiñones K. The longitudinal consistency of mother-child reporting discrepancies of parental monitoring and their ability to predict child delinquent behaviors two years later. Journal Of Youth And Adolescence. 2010;39:1417–1430. doi: 10.1007/s10964-009-9496-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ehrlich KB, Cassidy J, Dykas MJ. Reporter discrepancies among parents, adolescents, and peers: Adolescent attachment and informant depressive symptoms as explanatory factors. Child Development. 2011;82:999–1012. doi: 10.1111/j.1467-8624.2010.01530.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elliot AN, Carnes CN. Reactions of non-offending parents to the sexual abuse of their child: A review of the literature. Child Maltreatment. 2001;6:314–331. doi: 10.1177/1077559501006004005. [DOI] [PubMed] [Google Scholar]
- Esparza D. Maternal support and stress response in sexually abused girls ages 6–12. Issues in Mental Health Nursing. 1993;14:85–107. doi: 10.3109/01612849309006892. [DOI] [PubMed] [Google Scholar]
- Everson MD, Hunter WM, Runyon DK, Edelsohn GA, Coulter ML. Maternal support following disclosure of incest. Philadelphia, PA, US: Brunner/Mazel; 1991. [DOI] [PubMed] [Google Scholar]
- Feinberg M, Howe G, Reiss D, Hetherington EM. Relationship between perceptual differences of parenting and adolescent antisocial behavior and depressive symptoms. Journal of Family Psychology. 2000;14:531–555. [PubMed] [Google Scholar]
- Feiring C, Coates DL, Taska LS. Ethnic status, stigmatization, support, and symptoms development following sexual abuse. Journal of Interpersonal Violence. 2001;16:1307–1329. [Google Scholar]
- Ferdinand RF, van der Ende J, Verhulst FC. Parent adolescent disagreement regarding psychopathology in adolescents from the general population as a risk factor for adverse outcome. Journal of Abnormal Psychology. 2004;113:198–206. doi: 10.1037/0021-843X.113.2.198. [DOI] [PubMed] [Google Scholar]
- Friedrich WN, Urquiza AJ, Beilke RL. Behavior problems in sexually abused young children. Journal of Pediatric Psychology. 1986;11:47–57. doi: 10.1093/jpepsy/11.1.47. [DOI] [PubMed] [Google Scholar]
- Fromuth ME. The relationship of childhood sexual abuse with later psychological and sexual adjustment in a sample of college women. Child Abuse & Neglect. 1986;10:5–15. doi: 10.1016/0145-2134(86)90026-8. [DOI] [PubMed] [Google Scholar]
- Gaylord NK, Kitzmann KM, Coleman JK. Parents’ and children's perceptions of parental behavior: Associations with children's psychosocial adjustment in the classroom. Parenting: Science and Practice. 2003;3:23–47. [Google Scholar]
- Gold SR, Milan LD, Mayall A, Johnson AE. A cross-validation study of the trauma symptom checklist: The role of mediating variables. Journal of Interpersonal Violence. 1994;9:12–26. [Google Scholar]
- Gries LT, Goh DS, Andrews MB, Gilbert J, Praver F, Stelzer DN. Positive reaction to disclosure and recovery from child sexual abuse. Journal of Child Sexual Abuse: Research, Treatment, & Program Innovations for Victims, Survivors, & Offenders. 2000;9:29–51. [Google Scholar]
- Grills AE, Ollendick TH. Multiple informant agreement and the Anxiety Disorders Interview Schedule for Parents and Children. Journal Of The American Academy Of Child & Adolescent Psychiatry. 2003;42:30–40. doi: 10.1097/00004583-200301000-00008. [DOI] [PubMed] [Google Scholar]
- Guion K, Mrug S, Windle M. Predictive value of informant discrepancies in reports of parenting: Relations to early adolescents' adjustment. Journal Of Abnormal Child Psychology: An Official Publication Of The International Society For Research In Child And Adolescent Psychopathology. 2009;37:17–30. doi: 10.1007/s10802-008-9253-5. [DOI] [PubMed] [Google Scholar]
- Hadland SE, Werb D, Kerr T, Fu E, Wang H, Montaner JS, Wood E. Childhood sexual abuse and risk for initiating injection drug use: A prospective cohort study. Preventive Medicine: An International Journal Devoted To Practice And Theory. 2012;55(5):500–504. doi: 10.1016/j.ypmed.2012.08.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson BK, Kenkel MB. Stress, coping, and adjustment in female adolescent incest victims. Child Abuse & Neglect. 1991;15:293–305. doi: 10.1016/0145-2134(91)90073-m. [DOI] [PubMed] [Google Scholar]
- Kendall-Tackett KA, Williams LM, Finkelhor D. Impact of sexual abuse on children: A review and synthesis of recent empirical studies. Psychological Bulletin. 1993;113:164–180. doi: 10.1037/0033-2909.113.1.164. [DOI] [PubMed] [Google Scholar]
- Leifer M, Shapiro JP, Kassem L. The impact of maternal history and behavior upon foster placement and adjustment in sexually abused girls. Child Abuse & Neglect. 1993;17:755–766. doi: 10.1016/s0145-2134(08)80006-3. [DOI] [PubMed] [Google Scholar]
- Liang B, Williams LM, Siegel JA. Relational outcomes of childhood sexual trauma in female survivors: A longitudinal study. Journal of Interpersonal Violence. 2006;21(1):42–57. doi: 10.1177/0886260505281603. [DOI] [PubMed] [Google Scholar]
- Morrison NC, Clavenna-Valleroy J. Perceptions of maternal support as related to self-concept and self-report of depression in sexually abused female adolescents. Journal of Child Sexual Abuse: Research, Treatment, & Program Innovations for Victims, Survivors, & Offenders. 1998;7:23–40. [Google Scholar]
- Morrow K, Sorell GT. Factors affecting self-esteem, depression, and negative behaviors in sexually abused female adolescents. Journal Of Marriage And The Family. 1989;51(3):677–686. [Google Scholar]
- Mounts NS. Adolescents’ and their mothers’ perceptions of parental management of peer relationships. Journal of Research on Adolescence. 2007;17:169–178. [Google Scholar]
- Nugent NR, Saunders BE, Williams LM, Hanson RF, Smith DW, Fitzgerald MM. Posttraumatic stress symptom trajectories in children living in families reported for family violence. Journal of Traumatic Stress. 2009;22:460–466. doi: 10.1002/jts.20440. [DOI] [PubMed] [Google Scholar]
- Ohannessian C, Lerner RM, Lerner JV, von Eye A. Adolescent-parent discrepancies in perceptions of family functioning and early adolescent self-competence. International Journal Of Behavioral Development. 2000;24:362–372. [Google Scholar]
- Paredes M, Leifer M, Kilbane T. Maternal variables related to sexually abused children's functioning. Child Abuse & Neglect. 2001;25(9):1159–1176. doi: 10.1016/s0145-2134(01)00268-x. [DOI] [PubMed] [Google Scholar]
- Pelton J, Forehand R. Discrepancy between mother and child perceptions of their relationship: I. Consequences for adolescents considered within the context of parental divorce. Journal Of Family Violence. 2001;16:1–15. [Google Scholar]
- Pelton J, Steele RG, Chance M, Forehand R. Discrepancy between mother and child perceptions of their relationship: II. Consequences for children considered within the context of maternal physical illness. Journal Of Family Violence. 2001;16:17–35. [Google Scholar]
- Senn T, Carey M, Vanable P, Coury-Doniger P, Urban M. Characteristics of Sexual Abuse in Childhood and Adolescence Influence Sexual Risk Behavior in Adulthood. Archives of Sexual Behavior. 2007;36:637–645. doi: 10.1007/s10508-006-9109-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spaccarelli S, Fuchs C. Variability in symptom expression among sexually abused girls: Developing multivariate models. Journal of Clinical Child Psychology. 1997;26:24–35. doi: 10.1207/s15374424jccp2601_3. [DOI] [PubMed] [Google Scholar]
- Spaccarelli S, Kim S. Resilience criteria and factors associated with resilience in sexually abused girls. Child Abuse & Neglect. 1995;19:1171–1182. doi: 10.1016/0145-2134(95)00077-l. [DOI] [PubMed] [Google Scholar]
- Tremblay C, Hébert M, Piché C. Type I and type II posttraumatic stress disorder in sexually abused children. Journal of Child Sexual Abuse: Research, Treatment, & Program Innovations for Victims, Survivors, & Offenders. 2000;9:65–90. [Google Scholar]
- Tufts New England Medical Center, Division of Child Psychiatry. Sexually exploited children: Service and research project. Final report for the Office of Juvenile Justice and Delinquency Prevention. Washington, DC: U.S. Department of Justice; 1984. [Google Scholar]
- Waterman J, Kelly RJ, Oliveri M, McCord J. Behind the playground walls: Sexual abuse in preschools. New York, NY US: Guilford Press; 1993. [Google Scholar]
- Welsh DP, Galliher RV, Powers SI. Divergent realities and perceived inequalities: Adolescents', mothers', and observers’ perceptions of family interactions and adolescent psychological functioning. Journal of Adolescent Research. 1998;13:377–402. [Google Scholar]