

A 59-year-old man was arrested for unruly public behavior. He was subsequently found unresponsive with bilateral upper extremity extensor posturing and lower extremity triple flexion when stimulated. Over the next 48 hours, he awoke and became belligerent. MRI revealed innumerable cortical microhemorrhages on susceptibility-weighted imaging (figure, A) and asymmetric subcortical T2 hyperintensities (figure, B) consistent with cerebral amyloid angiopathy–related inflammation (CAA-ri).1 With corticosteroid treatment, he rapidly became calm and conversant, returning to near his premorbid baseline with only mild residual confusion within 1 week. CAA-ri is an uncommon, possibly autoimmune2 variant of CAA characterized by cognitive changes, seizures, headaches, and often, responsiveness to immunosuppressive therapy.1
Figure. Cerebral amyloid angiopathy–related inflammation.
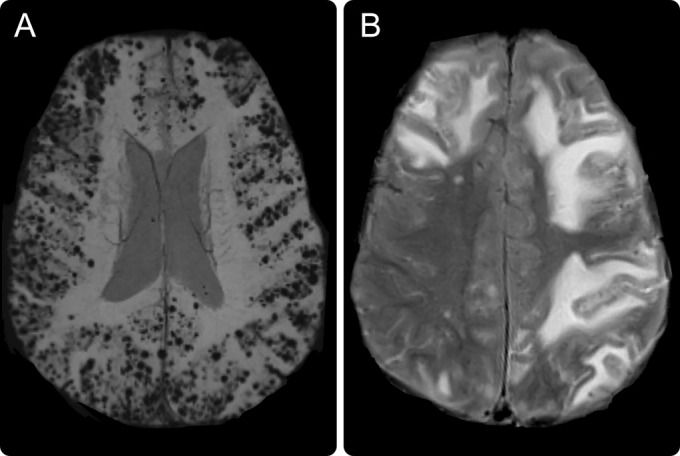
MRI demonstrates innumerable lobar microhemorrhages on susceptibility-weighted imaging sequence (A) and asymmetric subcortical T2 hyperintensities on fluid-attenuated inversion recovery sequence (B).
AUTHOR CONTRIBUTIONS
Dr. Berkowitz conceived of the manuscript, drafted the initial manuscript, revised the manuscript, created the figure, and revised the accompanying PowerPoint. Dr. Baker revised the manuscript. Dr. Miller revised the manuscript and developed the accompanying PowerPoint. Dr. Greenberg drafted the initial manuscript and revised the manuscript.
STUDY FUNDING
No targeted funding reported.
DISCLOSURE
A. Berkowitz reports no relevant disclosures. He receives royalties from Clinical Pathophysiology Made Ridiculously Simple (Medmaster, Inc.) and The Improvising Mind (Oxford University Press). J. Baker, J. Miller, and S. Greenberg report no disclosures relevant to the manuscript. Go to Neurology.org for full disclosures.
MYSTERY CASE RESPONSES
The Mystery Case series was initiated by the Neurology® Resident & Fellow Section to develop the clinical reasoning skills of trainees. Residency programs, medical student preceptors, and individuals were invited to use this Mystery Case as an educational tool. Responses were solicited through a group e-mail sent to the American Academy of Neurology Consortium of Neurology Residents and Fellows and through social media.
All the responses we received came from individuals rather than groups. Sixty percent of respondents correctly stated that the lobar microhemorrhages seen on the patient's susceptibility-weighted imaging sequence and the subcortical hyperintensities on the T2 sequence are most consistent with CAA-ri. A total of 47% of respondents correctly identified corticosteroid therapy as the treatment of choice for this condition.
This case highlights the importance of MRI in diagnosing this rare, but often treatable, variant of CAA.
Andrew Schepmyer, MD
University of British Columbia, Vancouver, Canada
REFERENCES
- 1.Kinnecom C, Lev MH, Wendell L, et al. Course of cerebral amyloid angiopathy–related inflammation. Neurology 2007;68:1411–1416. [DOI] [PubMed] [Google Scholar]
- 2.Piazza F, Greenberg SM, Savoiardo M, et al. Anti-amyloid β autoantibodies in cerebral amyloid angiopathy-related inflammation: implications for amyloid-modifying therapies. Ann Neurol 2013;73:449–458. [DOI] [PubMed] [Google Scholar]