

Abstract
Injury is a major public health problem in India. As very few studies are available from rural areas, hence the present study was carried out to study the epidemiology of injuries in the rural areas of Maharashtra. A cross-sectional study was carried out in Primary Health Centres (PHC) of a district in Maharashtra. 4790 subjects were studied using a two stage sampling technique. During last one year, 19.0% (95% CI: 17.7%–19.9%) had at least one injury. Majority of injuries (94.0%) were unintentional while assault and suicide related injuries were 37 (4.1%) and 10 (1.1%) respectively. Age, sex, education, occupation and socio-economic status were significantly associated with injuries.
Keywords: Injuries, Wounds, Falls, Road traffic crashes, Occupational injuries
Introduction
Globally, injuries account for 10% of all disability adjusted life years (DALYs) lost, and this is projected to possibly increase to 20% by 2020.1 In India, 3,42,309 accidental deaths were reported during year 2008.2 As per Gururaj et al in 2005, road traffic injuries resulted in the death of an estimated 110,000 persons, 2.5 million hospitalizations, 8–9 million minor injuries and economic losses to the tune of 3% of gross domestic product (GDP) in India.3 Maharashtra, accounting for 9.3% of country's population has, reported almost one sixth (18.3%) of accidental deaths due to unnatural causes. The major unnatural causes of accidental deaths were due to road accidents (37.1%), drowning (8.5%), railway accidents and rail-road accidents (8.3%), poisoning (7.6%) and sudden deaths (7.1%).2 A precise understanding of this mechanism is crucial to develop and implement mechanism for prevention and control of injuries. Many injuries are linked to social, environmental, cultural and biological issues in causation.3 Lack of good quality national or regional data has thwarted the recognition of injuries as public health problems as most of the studies are hospital based and from urban areas.4 There is a paucity of data related to injuries from rural areas in spite of the fact that a large number of population resides in rural areas. Therefore, this study was conducted to study the epidemiology of injuries in rural areas of Maharashtra.
Material and methods
This cross-sectional study was conducted in all 24 villages under Primary Health Centre, Kharangana (Gode) situated in Maharashtra state of India with a population of 34,940.
Proportion of injury over last 1 year came out to be 12% in a pilot study. Considering this as the minimal expected proportion and 5% alpha error, 10% relative error in the estimate of prevalence and the design effect of 1.5, the sample size required was 4400. Considering the average number of members in a family to be 4, total families to be sampled were 1100. All the members of the family were included in the study. Total 4790 subjects of all age were studied. Probability proportionate to size (PPS) of the village was used to decide the number of families to be sampled from each of the 24 villages. Required numbers of families were selected by systematic random sampling in each village. The study was approved by Institutional Ethics Committee.
Data was collected by using pre-tested interview schedule through house to house visits after obtaining written informed consent. A recall period of one month, three months and one year was used. For this study, injury has been defined as “external force/non-contagious substance striking the body or entering into the body and causing anatomical discontinuity of tissue or derange physiological function of the body”.5 The data were analyzed using Epi_info 6.04d.
Results
During last one year, 901 (19.0%; 95% CI: 17.7%–19.9%) had at least one injury. During last 3 months and one month 561 (11.8%; 95% CI: 10.8%–12.6%) and 294 (6.1%; 95% CI: 5.5%–6.8%) of the study subject had at least one injury, respectively (Table 1).
Table 1.
Magnitude of injury.
| Injury | Injury events (N = 4790) | Percentage | 95% CI |
|---|---|---|---|
| In last 1 month | 294 | 6.1% | 5.5%–6.8% |
| In last 3 month | 561 | 11.8% | 10.8%–12.6% |
| In last 1 year | 901 | 19.0% | 17.7%–19.9% |
Majority of injuries (94.0%) were unintentional while assault and suicide related injuries were 37 (4.1%) and 10 (1.1%) respectively. Out of the unintentional injuries, 281 (31.1%) were due to fall followed by Road traffic accident 229 (25.4%), Occupational injuries were 206 (23.0%) (Fig. 1).
Fig. 1.

Types of injuries.
Road was the most common place of sustaining injury 429 (47.7), followed by farm 268 (29.8%) while other places were at home 137 (15.1%), and in commercial area 36 (4.0%) (Fig. 2). Working in farm 260 (28.9%) was the most common activity at the time of sustaining an injury followed by traveling in/on vehicle 225 (25.0%). Other important activities that led to injuries were playing on the ground (18.4%), doing household work (13.2%) and standing/walking on the road (6.9%). Cut and abrasion were the most common 595 (66.0%) type of injuries followed by fracture 150 (16.6%). Highest proportion (23.2%) of injury was in 25–59 years of age followed by 19.5% in 15–24 years which are the economically productive groups. This was followed by elderly population (17.6%).
Fig. 2.
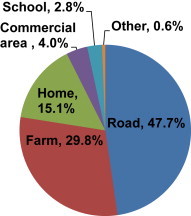
Place of injury.
Proportion of injury was 23.2% among males as compared to 13.8% in females. The proportion of injury was higher among below poverty line (BPL) subjects (20%) than that of subject from above poverty line (APL) families. Proportion of injury was maximum i.e. 29.8% among non-agricultural laborers followed by 26.3% cultivators and 18.4% among students. Highest proportion of injury (24.6%) was observed among subjects with primary education followed by those with middle and secondary education (19.7%). It was the least (15.0%) among those who had education of higher secondary and above. These were statistically significant association of injuries with age, sex, socio-economic status, occupation and education. Proportion of injuries did not differ significantly by marital status of study subjects (Table 2).
Table 2.
Socio-demographic correlates of injury.
| Age in years | Total (N = 4790) | Number with injury (%) | P-value |
|---|---|---|---|
| <5 | 259 | 44 (17.0) | <0.05 |
| 5–14 | 1014 | 158 (15.6) | |
| 15–24 | 2263 | 440 (19.5) | |
| 25–59 | 701 | 163 (23.2) | |
| 60 and above | 553 | 97 (17.6) | |
| Sex | |||
| Female | 2249 | 310 (13.8) | <0.05 |
| Male | 2541 | 591 (23.2) | |
| Socioeconomic status | |||
| Above poverty line | 1970 | 340 (17.2) | <0.05 |
| Below poverty line | 2820 | 561 (20.0) | |
| Occupation | |||
| House wife/not working | 911 | 116 (12.8) | <0.05 |
| Student | 1262 | 233 (18.4) | |
| Non-agricultural laborer | 363 | 108 (29.8) | |
| Agricultural laborer | 1416 | 249 (17.6) | |
| Cultivator | 593 | 156 (26.3) | |
| Business and service | 245 | 39 (16.0) | |
| Education | |||
| Illiterate | 867 | 154 (17.8) | <0.05 |
| Primary | 444 | 109 (24.6) | |
| Middle and secondary | 2498 | 490 (19.7) | |
| Higher secondary & above | 981 | 148 (15.0) | |
| Marital status | |||
| Unmarried | 2021 | 383 (18.9) | >0.05 |
| Married | 2520 | 479 (19.0) | |
| Widow/widower/divorced/separated | 249 | 39 (15.6) | |
Discussion
In the present study, we found that during last one year 19.0% of the study subjects had at least one injury. During last 3 months and one month, 11.8% and 6.1% of the study subjects had at least one injury, respectively. High prevalence of 30.6% was reported from rural Pondicherry.6 In similar study, from Sri Lanka, prevalence of injury was 2% during the last 30 days.7 In the present study, majority of the injuries were unintentional (94.0%). Studies from rural area of Pondicherry and Andhra Pradesh have reported about 99.2% and 96.5% of the injuries were unintentional.6,8
In the present study, 31.1% of the injuries were due to fall followed by road traffic accident. Occupational injuries were 23.0%. The assault and suicides related injuries were 4.1% and 1.1%, respectively. A study from Andhra Pradesh reported that the leading causes of injury was falls (38%) and road traffic crashes (25%).8 Study in Delhi reported fall (38%) was commonest mode of injury followed by road traffic injury (31%). Hospital based studies from rural Maharashtra also reported that road traffic injuries were the commonest cause amounting to 46.8% and 56.3%.9,10 A study from rural Pondicherry showed that most common causes of injuries were fall on the ground from height (7.4%), road traffic accidents (5.6%), and agriculture related injuries (5%).6 The findings of different studies are similar to that of our study. However, Lamawansa et al reported that, 28.2% injuries were due to animal bites, 18.8% were due to falls, 11.8% due to road traffic accidents.11 In the present study, road was the most common place of sustaining injury 47.7%, followed by farm 29.8%. Similarly, a study from Sri Lanka showed majority (41.1%) of injuries occurred at road, and 34% at home.11 In Delhi, most of the injuries occurred at home (41.26%) followed by road (39.8%).5 Findings of the Sri Lankan study was in concordance with our findings while Delhi study findings were different. The differences may be attributed to the study setting and the present study being a rural based, agriculture was the commonest occupation. Differences in cultures, occupations and lifestyle of the study subjects lead to differences in the findings.
To conclude, in the process of economic development and modernization, there is a phenomenal increase in injuries. Injury has so far lacked public awareness and is underrecognized as public health problem in India. This paper presents the evidence that there is high morbidity due to injuries in rural area of central India. The leading causes of injury were found to be falls, road traffic crashes and occupational which are all preventable. Age, sex, socio-economic status, occupation and less education were significantly associated with injuries.
Conflicts of interest
All authors have none to declare.
References
- 1.Verma P.K., Tewari K.N. World Health Organization; Delhi: 2003. Injury Prevention and Control: An Epidemiological Study of Injuries in the Area of Municipal Corporation of Delhi. [Google Scholar]
- 2.Murray C.J.L., Lopez A.D. Harvard School of Public Health; Boston: 1996. The Global Burden of Disease: A Comprehensive Assessment of Mortality and Disability from Diseases, Injuries and Risk Factors in 1990 and Projected to 2020. [Google Scholar]
- 3.National Crime Records Bureau . Ministry of Home Affairs, Government of India; New Delhi: 2008. Accidental Deaths and Suicides in India. [Google Scholar]
- 4.Gururaj G. Ministry of Health and Family Welfare, Government of India; New Delhi: 2005. Injuries in India: A National Perspective. [Google Scholar]
- 5.Gururaj G., Bengaluru Injury Surveillance Collaborators Group . National Institute of Mental health and Neuro Sciences; Bengaluru: 2010. Bengaluru Road Safety and Injury Prevention Programme: Injury Snapshots and Activity Profile 2010. Publication No: 72. [Google Scholar]
- 6.Ganapathy K., Dongre A.R., Mahalakshmy T. Epidemiology of injury in rural Pondicherry, India. J Inj Violence Res. 2010:1–5. doi: 10.5249/jivr.v3i2.74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Navaratne K.V., Fonseka P., Rajapakshe L. Population-based estimates of injuries in Sri Lanka. Inj Prev. 2009;15(3):170–175. doi: 10.1136/ip.2008.019943. [DOI] [PubMed] [Google Scholar]
- 8.Cardona M., Joshi R., Ivers R.Q. The burden of fatal and non-fatal injury in rural India. Inj Prev. 2008;14(4):232–237. doi: 10.1136/ip.2007.018259. [DOI] [PubMed] [Google Scholar]
- 9.Swarnakar M., Singh P., Dwivedi S. Pattern of trauma in central India: an epidemiological study with special reference to mode of injury. Int J Epidemiol. 2010;9(1) ispub.com/IJE/9/1/4726 Online [Accessed on 20.07.2013] [Google Scholar]
- 10.Agrawal A., Galwankar S., Kapil V. Epidemiology and clinical characteristics of traumatic brain injuries in a rural setting in Maharashtra, India 2007–2009. Int J Crit Illn Inj Sci. 2012;2(3):167–171. doi: 10.4103/2229-5151.100915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lamawansa M.D., Piyathilake A. Incidence of physical injuries in a rural Community in Sri Lanka: results of the first community survey in Sri Lanka. Indian J Commun Med. 2008;33(4):238–242. doi: 10.4103/0970-0218.43229. [DOI] [PMC free article] [PubMed] [Google Scholar]