

Abstract
Aims and objectives
Transradial interventions are gaining popularity in recent years. However the radial artery being small, there is a limitation in using interventional devices through this route. We have measured radial and ulnar arteries size in adult patients at our tertiary care cardiology center in southern Rajasthan.
Method
Adult patients >30 years, who came for Echocardiography at a tertiary care center were included. Radial and ulnar arteries inner diameters were measured 2–3 cm above the Styloid process in both forearms with the Ultrasonography. Patient information about weight, height, diabetes and hypertension were collected. Body mass index and Body surface area were calculated.
Results
We studied 204 patients, which includes 60.8% males. Mean diameter was 2.325 ± 0.4 mm mm for radial arteries and 2.358 ± 0.39 mm for ulnar arteries (p = 0.24). Hypertensive and male patients had larger mean radial artery diameter than non hypertensive (2.383 mm v/s 2.272 mm, p = 0.006) and female patients (2.37 mm v/s 2.26 mm, p = 0.008) respectively. Diabetic patients (2.305 mm) had nonsignificantly smaller radial arteries diameters than nondiabetics (2.329 mm, p = 0.6). We calculated correlations between radial arteries diameters and Body surface area, Body mass index, height and weight of patients, none of these correlations were statistically significant (r = 0.30, r = 0.28, r = 0.07, r = 0.031 respectively).
Conclusion
Mean radial artery diameter (2.325 ± 0.4 mm) in the study was slightly smaller than ulnar artery (2.358 ± 0.39 mm). Males and hypertensives had a larger mean radial artery diameter than females and non hypertensives. Radial artery inner diameter measurement by Ultrasonography may be more helpful than Allen's test for ideal selection of cases.
Keywords: Radial, Ulnar, Ultrasound
1. Introduction
Radial artery is being increasingly used by cardiologists for diagnostic and interventional purpose since last two decades after the work of Campeau1 and Kiemeneij.2 It is a safe alternative to the femoral route, however, transradial access is limited by a significantly higher rate of procedural failure because of small size of radial artery.3 Devices and catheters used for femoral route may not work through radial approach.
There is not much literature on predictors of radial artery size in an individual. Hypertension, non diabetics and male sex have been found to be associated with larger radial artery diameter.4–6 In these studies there was no correlation of radial artery diameters with Body mass index or Body surface area. The mean internal diameter of radial artery has been reported to be 3.67 ± 0.8 mm in the western population7 compared to 2.63 ± 0.35 mm in Asian population.8 Radial Artery is also being increasingly used in India for diagnostic and interventional purposes. There are not much reported data on size of radial arteries in the Indian population.
Ulnar artery is also being used by some investigators for coronary angiography and the procedure is found to be safe.9,10 There is no consensus regarding the size of distal ulnar artery in comparision to distal radial artery. Some investigators found ulnar artery larger than radial artery,6,11,12 while others contradicted this finding.4,13
The aims of this study were to measure radial and ulnar arteries diameter in the adult population by Ultrasound and evaluate the factors which can predict the size of radial or ulnar artery, so that one can know the appropriate size of devices and catheters suitable for radial or ulnar cardiac interventions.
2. Patients and methods
This cross sectional observational study was conducted in Hindustan Zinc Limited Cardiology Center, Department of Cardiology, Rabindra Nath Tagore Medical College, Udaipur, India, in June and July 2011.
Patients more than 30 years of age, who came to echocardiography laboratory for echocardiography, were included in the study. Internal diameters of right and left radial, and right and left ulnar were measured with the Doppler vascular probe of 5–11 MHz of GE vivid 7 dimension machine. 204 patients were included in the study. Age, gender, history of hypertension, history of diabetes, weight and height of the patient were collected at the time of radial and ulnar artery measurement. Body surface area (Mosteller formula)14 and Body mass index were derived from height and weight.
Radial and ulnar arteries diameters were measured 2–3 cm above the tip of Styloid Process. The smallest internal diameters of radial and ulnar arteries were recorded after comparing the size in both; longitudinal and transverse sections.
Continuous variables were expressed as mean ± SD. Independent t test was used to analyze data in between groups. A p value <0.05 was considered statistically significant.
Pearson's correlation coefficient was used to show relations between body parameters and radial and ulnar arteries diameters.
3. Results
We studied 204 patients which includes 60.8% males. 48.0% of patients were hypertensive and 15.2% were diabetic. Average age of patients in the study was 56.87 years.
Total 404 radial arteries of both the forearms (2 patients have undergone CABG with use of radial conduit and in other 2, radial arteries were not palpable or aberrant) were studied. The mean internal diameters of right and left radial arteries were 2.329 ± 0.4 mm and 2.322 ± 0.4 mm respectively (p value 0.86). The mean diameter of all the radial arteries was 2.325 ± 0.4 mm. Total 402 ulnar arteries of both the forearms (6 were not palpable or aberrant) were studied. The mean internal diameters of right and left ulnar arteries were 2.339 ± 0.37 mm and 2.376 ± 0.4 mm respectively (p value 0.34). The mean diameter of all the ulnar arteries was 2.358 ± 0.39 mm. Fig. 1 shows that difference between mean radial and ulnar arteries internal diameters at wrist was non significant (p value 0.24).
Fig. 1.
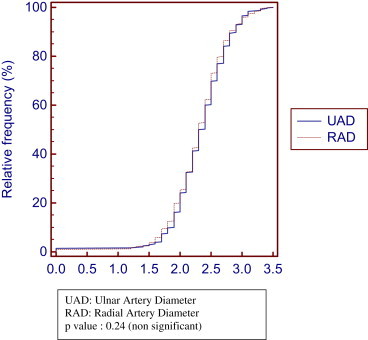
Comparision of radial and ulnar artery diameter frequency distribution curve.
Table 1 shows radial and ulnar arteries inner diameters with variables like sex, hypertension and diabetes. The mean diameter of radial arteries in males was 2.369 ± 0.41 mm in comparison to females 2.259 ± 0.39 mm (p value <0.01). Similar result was found for ulnar arteries of males in comparison to females, 2.408 ± 0.4 mm and 2.282 ± 0.36 mm respectively (p value <0.01). Hypertensive patients had larger radial arteries (2.383 ± 0.4 mm) in comparison to non hypertensive patients (2.272 ± 0.41 mm, p value < 0.01). Diabetic patients (2.305 ± 0.40 mm) had smaller mean radial artery diameter than non diabetics (2.329 ± 0.41 mm), but this difference was not significant (p value 0.06). There were no significant correlations of radial arteries inner diameters, with Body surface area (r = 0.30) and Body mass index (r = 0.28). Similarly no correlations were found with height and weight of the patients (r = 0.07, r = 0.30 respectively). Table 2 shows that 20 patients (9.8%) had both radial artery diameter less than 2 mm (outer diameter of 4F sheath), out of these 20 patients only 3 (1.5%) patients had Ulnar artery of both hand size less than 2 mm. Another 35 (17.2%) patients (total 55 (26.9%) patients, including those who had size less than 2.0 mm) had radial artery size of both hands less than 2.3 mm (5F sheath outer diameter) and 67 patients (32.8%) had radial artery size between 2.3 and 2.6 mm less (6F sheath outer diameter is 2.6 mm).
Table 1.
Radial and ulnar arteries mean diameters in different subgroups.
| Radial arteries mean diameter (mm) | Ulnar arteries mean diameter (mm) | |||
|---|---|---|---|---|
| 1.Gender | ||||
| Male | 2.369 ± 0.41 | p ≤ 0.01 | 2.408 ± 0.4 | p ≤ 0.01 |
| Female | 2.259 ± 0.39 | 2.282 ± 0.36 | ||
| 2.Hypertension | ||||
| Yes | 2.383 ± 0.4 | p ≤ 0.01 | 2.393 ± 0.39 | p = 0.07 |
| No | 2.272 ± 0.41 | 2.324 ± 0.38 | ||
| 3.Diabetes | ||||
| Yes | 2.305 ± 0.40 | p = 0.06 | 2.352 ± 0.37 | p = 0.49 |
| No | 2.329 ± 0.41 | 2.389 ± 0.44 | ||
Table 2.
Radial and ulnar arteries diameters in comparison to outer diameter of standard sheaths of different size.
| Radial arteries of both forearms | Radial and ulnar arteries of both forearms | |
|---|---|---|
| <2.0 mm (4F OD) | 20 (9.8%) | 3 (1.4%) |
| 2.0–2.3 mm (5F OD) | 35 (17.2%) | 18 (8.4%) |
| 2.3–2.6 mm (6F OD) | 67 (32.8%) | 62 (30.4%) |
| 2.6–2.8 mm (7F OD) | 36 (17.6%) | 40 (19.6%) |
4. Discussion
This study showed that male and hypertensive patients had larger radial arteries diameter than female and nonhypertensive. Non diabetic patients also had larger arteries than diabetic patients but this difference was not significant. Ulnar arteries were marginally larger than radial arteries at the level of wrist but this difference did not reach level of significance.
Mean diameter of radial arteries (2.325 ± 0.4 mm) in this study was smaller than western population (3.67 ± 0.8 mm).7 Similarly Mean radial artery diameters were larger in Japanese study by Saito et al15 and Korean study by Yoo8 than in the current study. But the current findings were similar to other studies in South East Asian countries like Pakistan (2.25 ± 0.4 mm) by Asharaf et al6 and Singapore (2.45 ± 0.54 mm) by Loh et al.4 So it seems that radial arteries diameters are smaller in South East Asian countries than other parts of the world.
Males had larger radial arteries diameters than females in the current study. This finding correlates with previous studies.4,6,15 Loh et al ascribe this finding to the larger size of males, but we found no correlations between radial artery size and body parameters.
Hypertensive patients had larger diameters of radial arteries than non hypertensives in the present study. This finding is similar to studies by Loh et al4 and Khader et al,5 but in contrast to the study by Asharaf et al6 and Khader et al5 found larger diameters of radial arteries in patients with hypertension due to increased compliance. Loh4 proposed compensatory enlargement of radial arteries similar to effect of hypertensive heart disease. We propose that vasodilators used as antihypertensive may be a factor other than the above two proposed mechanisms. Non diabetic patients had larger radial arteries than diabetic, but this difference did not reach significance level (p = 0.06). This observation is similar to that of other investigators.4,6 Ruengkularh and colleagues16 and Chowdhry et al17 also demonstrated that factors predictive of intimal hyperplasia and atherosclerosis in radial arteries were age and diabetes.
We found no significant correlations between radial artery diameters and body parameters like Body surface area, Body mass index, height and weight, similar to Ashraf et al6 and Saito S et al.15
Outer diameter of 5F, 6F and 7F introducer sheaths are usually 2.3 mm, 2.6 mm and 2.8 mm respectively. Outer diameter of introducer sheaths vary according to manufacturer. In our study we found that 55 (26.9%) patients had radial arteries internal diameters smaller than 2.3 mm (5F introducer sheath outer diameter) in both forearms. Out of these 55 patients only 21 (10.2%) had ulnar arteries diameters smaller than 2.3 mm, so ulnar arteries may be a suitable alternative in patients who have smaller radial arteries. In practice it was found that success rate of transradial intervention was more than 95%.3 Saito S et al said that radial arteries can be expanded over resting diameters during sheath insertion.15 They found that radial artery internal diameter/sheath outer diameter ratio (RAID/SOD) >1 is associated with 4% severe flow reduction in comparison to RAID/SOD <1, which is associated with 13% severe flow reduction.15
Ultrasound examination is superior to quantitative angiography for measurement of radial arteries diameter in view of its noninvasive nature, absence of in dwelling catheter or contrast induced spasm and the facility of simultaneous measurement of blood flow. It may be a valuable screening tool for radial artery diameter measurement in population with a likelihood of having smaller radial arteries. It is also helpful for new radial interventionists, for ideal selection of cases. In patients with a small radial artery, ulnar artery may be used alternatively for intervention. Other options to prevent failure or complication in transradial intervention may be use of sheath less catheters, spasmolytic cocktail and adequate anticoagulation.
5. Conclusion
Mean radial artery internal diameter in the study was 2.325 ± 0.4 mm. Ulnar arteries (2.358 ± 0.39 mm) were slightly larger than radial arteries. Males and hypertensive had larger radial arteries. No other variable significantly predicts size of radial artery. Size of radial arteries was smaller in our study than western countries but similar to other studies in Pakistan and Singapore. Ultrasound examination is a useful noninvasive measurement for arteries of the forearms. Ultrasound helps in ideal selection of sheaths and catheters for transradial intervention which cannot be predicted by Allen's test alone.
Conflicts of interest
All authors have none to declare.
References
- 1.Campeau L. Percutaneous radial artery approach for coronary angiography. Catheter Cardiovasc Diagn. 1989;16:111–121. doi: 10.1002/ccd.1810160103. [DOI] [PubMed] [Google Scholar]
- 2.Kiemeneij F., Laarman G.J. Percutaneous transradial artery approach for coronary stent implantation. Catheter Cardiovasc Diagn. 1993;30:173–178. doi: 10.1002/ccd.1810300220. [DOI] [PubMed] [Google Scholar]
- 3.Brueck M., Bandorski D., Kramer W. A randomized comparison of transradial versus transfemoral approach for coronary angiography and angioplasty. J Am Coll Cardiol Intv. 2009;2:1047–1054. doi: 10.1016/j.jcin.2009.07.016. [DOI] [PubMed] [Google Scholar]
- 4.Loh Y.J., Naka M., Tan W.D., Lin C.H., Tan Y.S., Chua Y.L. Factors influencing radial artery size. Asian Cardiovasc Thorac Ann. 2007;15:324–326. doi: 10.1177/021849230701500412. [DOI] [PubMed] [Google Scholar]
- 5.Khder Y., Bray-Deboscs L., Aliot E., Zannad F. Effects of blood pressure control on radial artery diameter and compliance in hypertensive patients. Am J Hypertens. 1997;10:269–274. doi: 10.1016/s0895-7061(96)00347-0. [DOI] [PubMed] [Google Scholar]
- 6.Asharaf T., Panhwar Z., Habib S., Memon M.A., Shamsi F., Arif J. Size of radial and ulnar artery in local population. J Pak Med Assoc. 2010;60:817–819. [PubMed] [Google Scholar]
- 7.Monségu J., Bertrand B., Schiano P. Radial artery occlusion after transradial artery procedures: an ultrasonographic analysis. Am J Cardiol. 2002;90:166H. [Google Scholar]
- 8.Yoo B.S., Lee S.H., Ko J.Y. Procedural outcomes of repeated transradial coronary procedure. Catheter Cardiovasc Interv. 2003;58:301–304. doi: 10.1002/ccd.10400. [DOI] [PubMed] [Google Scholar]
- 9.Aptecar E., Dupony P., Chaouch M.C., Bussy N., Caterino G. Percutaneous transulnar artery approach for diagnostic and therapeutic coronary interventions. J Invasive Cardiol. 2005;17:312. [PubMed] [Google Scholar]
- 10.Knebel Alexis Vasiluk, Cardoso Cristiano Oliveira, Rodrigues La Hore Correa. Safety and feasibility of transulnar cardiac catheterization. Tex Heart Inst J. 2008;35:268–272. -7. [PMC free article] [PubMed] [Google Scholar]
- 11.Gray H. 38th ed. Churchill Livingstone; London: 1995. Anatomy of the Human Body. [Google Scholar]
- 12.Vogelzang R.L. Arteriography of the hand and wrist. Hand Clin. 1991;7:63–86. [PubMed] [Google Scholar]
- 13.Brzeniski M., Luisetti T., London M.J. Radial artery cannulation: a comprehensive review of recent anatomic and physiological investigations. Anesth Analg. 2009;109:1763–1781. doi: 10.1213/ANE.0b013e3181bbd416. [DOI] [PubMed] [Google Scholar]
- 14.Mostellr R.D. Simplified calculation of body surface area. N Eng J Med. 1987;22:1098. doi: 10.1056/NEJM198710223171717. [DOI] [PubMed] [Google Scholar]
- 15.Saito S., Hajimethari, Hosekawa G., Tanaka S. Influence of the ratio between radial artery inner diameter and sheath outer diameter on radial artery flow after transradial coronary intervention. Catheter Cardiovasc Interv. 1999;46:173–178. doi: 10.1002/(SICI)1522-726X(199902)46:2<173::AID-CCD12>3.0.CO;2-4. [DOI] [PubMed] [Google Scholar]
- 16.Ruengsakulrach P., Sinclair R., Komeda M., Raman J., Gordon I., Buxton B. Comparative histopathology of radial artery versus internal thoracic artery and risk factors for development of intimal hyperplasia and atherosclerosis. Circulation. 1999;100:139–144. doi: 10.1161/01.cir.100.suppl_2.ii-139. [DOI] [PubMed] [Google Scholar]
- 17.Chowdhery U.K., Airan B., Mishra P.K. Histopathology and morphometry of radial artery conduits: basic study and clinical application. Ann Thorac Surg. 2004;78:1614–1621. doi: 10.1016/j.athoracsur.2004.03.105. [DOI] [PubMed] [Google Scholar]