

Introduction
Syringomas are benign neoplasm originating from the eccrine sweat duct. They commonly present as soft, flesh coloured to slightly yellow dermal papules on the lower eyelids of healthy individuals. Generalised eruptive form is a rare clinical variant of this benign eccrine sweat gland neoplasm. This occurs mainly in women at puberty or later in life. First described by Jacquet and Darier in 1987, the lesions occur in large numbers and in successive crops on the anterior chest, neck, upper abdomen and axilla. The lesions consist of asymptomatic, multiple, small, firm, skin-coloured or slightly yellowish papules typically present in a bilaterally symmetrical distribution.1 Skin biopsy is required to confirm the diagnosis. Treatment of this benign condition is cosmetic only in both localised and eruptive form.2 An unusual case of a 39-year-old male with 24 years history of eruptive syringomas is being presented.
Case report
A 39-year-old male patient presented to the skin department of a United Nations hospital with 24 years history of diffuse numerous papular eruptions over face, trunk and upper extremity. The majority of the lesions were present over anterior aspect of body. The lesions developed initially over the cheeks below the eyelids and gradually spread over to the forehead, temples, trunk, neck and arms over the next 5 years. There after the lesions remained stable without progression to other areas of the body. The lesions were not associated with local or systemic symptoms. Other family members were not affected. Dermatological examination revealed well demarcated, firm, hyperpigmented, brownish, flat topped papules of variable size (1–3 mm in diameter) over the neck, chest and abdomen resembling verruca plana (Fig. 1) and well demarcated, firm, hyperpigmented papules with variable size (1–2 mm in diameter) over the face (Fig. 2), lower back and upper extremities resembling acneiform eruptions. Similar lesions were seen grouped around the umbilicus (Fig. 3). The lesions did not reveal scaling, vesiculation, erosion or crusting. The examination of the mucous membranes, palms and soles, hair and nails was normal. No other systematic involvement was noted. Eruptive xanthomas, eruptive syringoma and mild form of Darier's disease were considered in the differential diagnosis. Laboratory investigations including routine haematological examination, liver and renal function tests were all within normal limits. Serum lipids were not raised. Skin biopsy was performed from a lesion on the abdomen. Histopathological examination of the biopsy revealed a well-circumscribed lesion embedded in an eosinophilic stroma. This lesion was formed of small ducts lined by two-cell thick epithelium and few of them were showing comma-shaped extensions (Fig. 4). Based on the clinical and histopathological appearance of the lesions, a diagnosis of generalised eruptive syringoma was made. Since the distribution of lesions was generalised, surgical options were not considered and the patient was advocated cap isotretinoin 40 mg OD for 16 weeks. However, no significant clinical improvement was seen. The patient was subsequently lost to follow up.
Fig. 1.

Photograph showing well demarcated, hyperpigmented, brownish, flat topped papules of variable size (1–3 mm in diameter) over the neck, chest and abdomen resembling verruca plana.
Fig. 2.

Photograph showing well demarcated, hyperpigmented, brownish papules with variable size (1–2 mm in diameter) over the face resembling acneiform eruptions.
Fig. 3.

Photograph showing hyperpigmented grouped papules around the umbilicus.
Fig. 4.
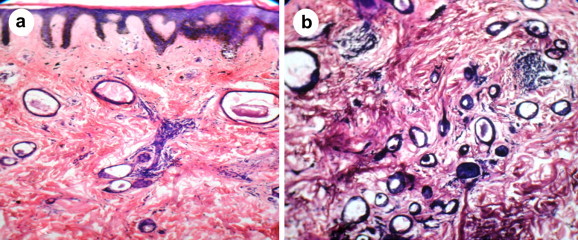
H & E stained section showing eccrine ductal structures embedded in an eosinophilic stroma. Some of the ducts are showing characteristic tadpole like appearance.
Discussion
Syringomas are benign adnexal neoplasia that are derived from eccrine ductal elements. Syringomas first appear during puberty or the third or the fourth decade.3,4 The incidence of syringomas appears to be higher in Asians and African-Americans. Although the clinical variants localised on the eyelid is more common, many other clinical variants are reported. Friedman and Butler proposed a classification, which consists of four groups according to their clinical features and associations, namely localised form, generalised eruptive form, a form associated with trisomy 21 and familial form.3 In eruptive syringoma a rare clinical variant, the lesions consists of small skin-coloured or yellowish dermal papules and are usually smaller than 3 mm in diameter found in the axillae, chest and abdomen, in addition to the usual site on the upper part of the cheek and the lower eyelids. They are usually symmetrical and appear in clusters. Syringomas are characterised histologically by the presence of cystic ductal structures lined by two layers of cells. Cells of the duct show a comma like tail of epithelial cells at one end giving the appearance of tadpole.5 Our 39-year-old male patient presented with unusual hyperpigmented, flat topped papular lesions, few of them grouped, showing pseudo koebnerisation resembling flat warts over the neck, chest and abdomen and acneiform like eruptions over the face with sparing of axilla and legs. The diagnosis was established by performing a skin biopsy which demonstrated multiple small ducts lined by rows of flattened epithelial cells with epithelial strands within the upper and mid-dermis (Haematoxylin & eosin) giving rise to the characteristic tadpole appearance (Fig. 4). Cosmesis is the main reason for treatment, and there is no long-term significant morbidity associated with syringomas. Treatment modalities are multiple but unsatisfactory. The main aim of the treatment is to minimise scarring and to prevent recurrence. Different treatment modalities include surgical excision, electrocautery, cryotherapy, dermabrasion, trichloroacetic acid, carbon dioxide laser ablation and oral and topical retinoids. Our case had widespread lesions which were involving large parts of the body, hence all surgical modalities of treatment were not considered due to the risk of scarring and the patient was subjected to oral isotretinoin therapy.
Generalised eruptive syringoma is an exotic rarity and our case was further unusual due to the presence of hyperpigmented lesions clinically resembling verrucae plana over the neck and trunk.
Conflicts of interest
All authors have none to declare.
References
- 1.Jamalipour M., Mitra H., Rajabi P. Generalised eruptive syringoma. Indian J Dermatol. 2009;54(1):65–67. doi: 10.4103/0019-5154.48992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Teixeira M., Ferreira M., Machado S., Alves R., Selores M. Eruptive syringomas. Dermatol Online J. 2005;11:34. [PubMed] [Google Scholar]
- 3.Friedman S.J., Butler D.F. Syringoma presenting as milia. J Am Acad Dermatol. 1987;16:310–314. doi: 10.1016/s0190-9622(87)70041-3. [DOI] [PubMed] [Google Scholar]
- 4.Soler-Carrilo J., Estrach T., Mascaró J.M. Eruptive syringoma: 27 new cases and review of the literature. J Eur Acad Dermatol Venereol. 2001;15:242–246. doi: 10.1046/j.1468-3083.2001.00235.x. [DOI] [PubMed] [Google Scholar]
- 5.Nair P.S. A clinicopathological study of skin appendageal tumours. Indian J Dermatol Venereol Leprol. 2008;74:550. doi: 10.4103/0378-6323.44339. [DOI] [PubMed] [Google Scholar]