

Abstract
Objective
This in vitro study aimed to evaluate the influence of different surface treatments, 3 luting agents and thermocycling on microtensile bond strength (µTBS) to zirconia ceramic.
Material and Methods
A total of 18 blocks (5x5x4 mm) were fabricated from zirconia ceramic (ICE Zirkonia) and duplicated into composite blocks (Alphadent). Ceramic blocks were divided into 3 groups (n=6) according to the following surface treatments: airborne-particle abrasion (AA), silica-coating, (SC) (CoJet) and silica coating followed by silane application (SCSI) (ESPE Sil). Each group was divided into 3 subgroups (n=2) according to the 3 luting agents used. Resin-modified glass-ionomer cement (RMGIC, Ketac Cem Plus), self-adhesive resin cement (UN, RelyX Unicem) and adhesive resin cement (ML, MultiLink Automix) were used for bonding composite and zirconia blocks. Each bonding assembly was cut into microbars (10 mm long and 1±0.1 mm2). Seven specimens of each subgroup were stored in water bath at 37ºC for 1 week. The o ther 7 specimens were stored in water bath at 37ºC for 30 days then thermocycled (TC) for 7,500 cycles. µTBS values were recorded for each specimen using a universal testing machine. Statistical analyses were performed using a 3-way ANOVA model followed by serial 1-way ANOVAs. Comparison of means was performed with Tukey's HSD test at (α=0.05).
Results
µTBS ranged from 16.8 to 31.8 MPa after 1 week and from 7.3 to 16.4 MPa after 30 days of storage in water and thermocycling. Artificial aging significantly decreased µTBS (p<0.05). Considering surface treatment, SCSI significantly increased µTBS (p<0.05) compared to SC and AA. Resin cements (UN and ML) demonstrated significantly higher µTBS (p<0.05) compared to RMGIC cement.
Conclusions
Silica coating followed by silane application together with adhesive resin cements significantly increased µTBS, while thermocycling significantly decreased µTBS.
Keywords: Ceramics, Surface treatment, Resins, Bond strength
INTRODUCTION
High mechanical properties, chemical stability, and biocompatibility make zirconia an attractive core material for fabrication of all-ceramic restorations4,7,15-19. Bonding techniques of all-ceramic restorations are dependent on chemical compositions of each ceramic system12. Hydrofluoric acid etching and silanization are mandatory steps to achieve a durable resin bonding to silica ceramics12. On the other hand zirconia ceramic requires alternative techniques for long-term durable resin bonding2,10,23. Therefore several surface treatments are used to improve bonding to zirconia ceramic3,5,6, such as selective infiltration etching (SIE) technique1, laser etching8, alumina coating11, silica ceramic coating13, tribochemical silica coating3,6,9,12,22 or airborne-particle abrasion3,6,9,14,20,22,25. Several ceramic primers have been introduced into the dental market recently to enhance chemical bonding to zirconia ceramic12,14,16, such as primers containing a phosphonic acid monomer, 6-MHPA (6-methacryloxyhexylphosphonoacetate), (AZ, primer) or 3-trimethoxysilylpropyl methacrylate, MDP, ethanol (Clearfil Ceramic Primer) and organophosphate monomer, carboxylic acid monomer and other monomers (Z-Prime Plus)12,14,16. However, there are obvious problems in obtaining a durable bonding to zirconia ceramics7,14.
Conventional luting agents, such as glass ionomer cement (GIC), could be used for cementation of zirconia ceramic full-coverage restorations5,9,14. However adhesive cementation is preferred in case of compromised retention and resin-bonded fixed dental prosthesis3-5,14. Self-adhesive resin cements have been introduced into the dental market to simplify bonding procedures21. However bond strength results to zirconia ceramics in the literatures using different categories of luting agents are very controversial2,9,15,22,25. Moreover, chemical composition of zirconia ceramic and intaglio surface morphology are unique for each commercial system4,5. Therefore, conclusions drawn considering bonding to one zirconia ceramic system may not be applicable to other systems4,5.
Recently, a new zirconia ceramic (ICE Zirconia, ZirkonZahn) has been introduced in the dental market. According to its manufacturer, this zirconia ceramic has bending strength over 1,400 MPa and could be used for fabrication of 16-unit fixed dental prosthesis. However, no independent data considering bonding to this zirconia ceramic has been published yet.
Several studies have evaluated bond strength of adhesives in vitro in terms of shear4,5,18, tensile27,28 and microtensile bond strength (µTBS)2,26,30. However, µTBS test is considered as the most accurate one24,30. Moreover, aging and thermocycling are two important factors that have been shown to decrease the bond strength in in vitro studies4,5. The purpose of this study was to investigate in vitro the influence of different surface treatments, storage in water and thermocycling, on the µTBS of 3 luting agents to this zirconia ceramic. The null hypotheses of the study were (1) a durable bonding to the zirconia ceramic would be achieved regardless of the surface treatments, (2) self-adhesive resin cement would provide a durable bonding to this zirconia ceramic similar to multistep adhesive resin cement, and (3) resin-modified GIC (RMGIC) would provide a durable bonding to this zirconia ceramic compared to both adhesive resin cements.
MATERIAL AND MEHTODS
A total of 18 fully-sintered zirconia blocks (5x5x4 mm) in dimension were used for this study. Each ceramic block was duplicated in light-polymerized hybrid, type 2 restorative composite resin (Alphadent composite, shade A2) using vinyl polysiloxane material (President, Coltène Whaledent, Altstätten, Switzerland) (Figure 1). Composite resin was applied in increments 1-2 mm thickness and carefully condensed with ST Instrument with plastic working end (OptraSculpt, Ivoclar Vivadent, Schaan, Liechtenstein). Each increment was light-polymerized for 40 s at 5 mm distance and an intensity of irradiation 130 mW/cm2 (FutoLux 2, Carlo De Gorgi, Milano, Italy).
Figure 1.
Materials used in the study
| Materials | Lot/Batch No | Manufacturer |
|---|---|---|
| Zirconium-oxide ceramic with the following composition [Y2O3, 4.95-5.26, Al2O3, 0.15-0.35, SiO2, Max 0.02, Fe2O3 max. 0.01, Na2O3 Max.0.04] | CE0476 | ICE Zirkonia, ZirkonZahn, Gais, Italy |
| Transparent, two past, self curing adhesive resin cement dimethacrylate and HEMA, with barium glass silica and filler base/catalyst past in Clicker | K49940 | Multilink Automix; Ivoclar Vivadent, Schaan, Liechtenstein |
| Paste B, methacrylated polycarboxylic acid, BisGMA, HEMA, water, potassium persulfate, zirconia silica filler | ||
| Powder, alkaline (basic) fillers, silanated fillers, initiator components, pigments | ||
| Silane coupling agent 3-methacryloxyprophyltrimethoxysilane in ethanol | 323995 | ESPE Sil, 3M ESPE |
| 50 μm Al2O3 particles for airborne-particle abrasion 30 μm SiO2 | 14540 322199 | Alumina particles Pluradent, Offenbach, Germany CoJet - Sand, 3M ESPE |
| Visible light activated, radiopaque hybrid, type 2 composite resin | P121FJ | Alpha.Dent composite, Dental technologies, Illinois, USA |
Surface treatment before bonding
Ceramic blocks were divided into 3 groups (n=6) according to surface treatment as follow: Group 1: airborne-particle abrasion (AA), using Al2O3 (50-µm aluminum oxide particles, Pluradent, Offenbach, Germany) at 0.28 MPa for 13 s at a distance of 10 mm4 (Ney Blastmate II, Ney, CA, USA). Zirconia ceramic blocks were ultrasonically cleaned in distilled water for 3 min and dried with oil-free air stream; Group 2: Silica coating (SC), airborne-particle abrasion using 50-µm Al2O3 particles at 0.28 MPa for 13 s at a distance of 10 mm4 followed by airborne-particle abrasion with 30-µm SiO2 particles (CoJet sand, 3M ESPE, Seefeld, Germany) at a pressure of 0.25 MPa for 20 s at a distance of 10 mm26 (Ney Blastmate II). Zirconia ceramic blocks were ultrasonically cleaned in distilled water for 3 min and dried with oil-free air stream; Group 3 Silica coating and silane application (SCSI), same as Group SC followed by silane application26 (ESPE Sil, 3-methacryloxyprophyltrimethoxysilane in ethanol, 3M ESPE). Five minutes were allowed to elapse for silane reaction26.
Bonding zirconia and composite blocks
Each main group was divided into 3 subgroups (n=2) according to the following 3 luting agents, Ketac Cem Plus, RelyX Unicem and MultiLink Automix. Bonding procedures were performed according to the manufacturers' recommendations for each luting agent:
Ketac Cem Plus (GI): self curing, radiopaque, fluoride-releasing, RMGIC containing BisGMA and HEMA (3M ESPE). Equal amounts of past A and B were extruded on waxed paper pad, mixed for 20 s using a plastic spatula until a uniform color was achieved. The mix was applied to the intaglio surfaces of the zirconia ceramic blocks.
RelyX Unicem Aplicap (UN): dual-cure, self-adhesive resin cement, containing phosphoric acid monomer and methacrylate monomers (3M ESPE). The capsule was activated for 4 s, and then mixed in amalgamator (Silver Mix 80, Carlo De Giorgi, Milano, Italy) for 10 s. The capsule was inserted into the applier and cement was dispensed directly onto the intaglio surfaces of the zirconia ceramic blocks.
MultiLink Automix (ML): self-curing, transparent, two-past adhesive resin cement, containing dimethacrylate and HEMA (Ivoclar Vivadent). Equal amounts of adhesive resin cement were extruded, mixed for 20 s and applied to the intaglio surfaces of the zirconia ceramic blocks. Finally composite blocks were bonded to intaglio surfaces of zirconia ceramic blocks. Excess luting cement was removed using disposable minibrush (Ivoclar Vivadent). The bonding assembly was kept under a static load of 40 N for 5 min (Articolo 719/00, #1L01; Carlo De Giorgi), Combination of 3 surface treatments and 3 luting agents resulted in 9 test groups as follows: GIAA, GISC, GISCSI, UNAA, UNSC, UNSCSI, MLAA, MLSC and MLSCSI.
Preparation of microbars
Each block was then bonded with cyanoacrylate glue (Uhu®, batch 40267647, Uhu, Bühl, Germany) to a metal base that was fixed to a cutting machine2,26 (Isomet 1000, Buehler Ltd., Lake Bluff, IL, USA). Cutting was created under wet condition. The first 0.5-mm-thick slice was discarded2,6,26. Three slices 1±0.1 mm in thickness were obtained. Each slice was rotated 90º and bonded to another metal base again2,6,26. The first slice 0.5 mm was also disregarded. Other 3 additional cuts 1±0.1 mm in thickness were made2,6,26. This procedure was repeated for the other 2 slices. A total of 9 non-trimmed bar specimens (10 mm long and 1±0.1 mm2) bonded surface area were obtained from each block6. Microscopic examination (Wild Makroskop M 420; Heerbrugg, Switzerland) at 20× magnification of the bar specimens revealed that only 15 specimens from group GISC and 14 specimens from group GISCSI were free from microcracks. Therefore for standardization of the test groups, only 14 specimens from each subgroup were used to complete the test. Seven specimens from each subgroup were stored in water bath at 37ºC for 1 week. While the other 7 specimens were stored in water bath at 37ºC for one month followed by thermocycling (TC) for 7,500 cycles. Each cycle was consists of 1 minute in 5ºC cold bath and 1 minute in 55ºC hot bath with a dwell time of 30 s. Specimens were dried and glued parallel to the long axis of an adapted caliper using cyanoacrylate glue (Uhu®, batch 40267647, Uhu). This apparatus was fixed to the universal testing machine (Type 500, Lloyd Instrument, Farnham, UK).
Microtensile bond strength test
Specimens were loaded in tension to failure (Figure 2) at a crosshead speed of 1 mm/min. Microtensile bond strength µTBS values were recorded for each specimen in MPa using the formula:
Figure 2.
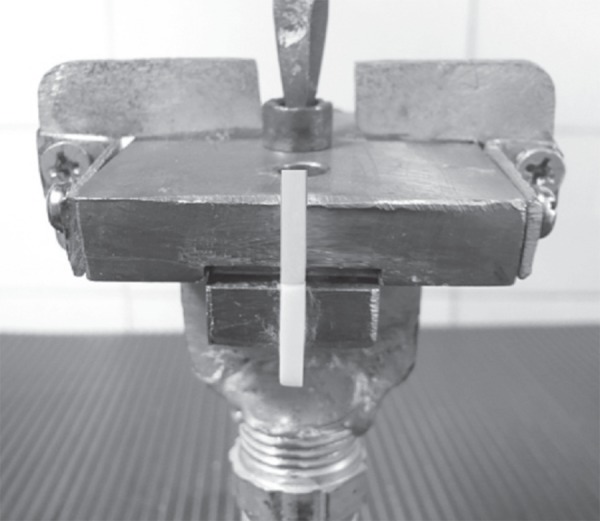
Debonded specimen glued to an adapted caliper and fixed to the universal testing machine
α=L/A, where 'L' is the load at failure (N) and 'A' is the bonded area 1±0.1 mm2.
Statistical analysis was conducted using the SPSS statistical software, version 16.0 (SPSS Inc, Chicago, Ill, USA). Statistical analyses were performed with 3-way ANOVA model followed by serial 1-way ANOVAs. Post Hoc Tukey-HSD test at α=0.05 was performed to test statistical significance between the groups.
Microscopic examination of the debonded specimens
The fractured interfaces of the debonded specimens were examined with a light microscope (Wild Makroskop M 420) at x20 magnification to determine the failure pattern, which was assigned to cohesive failure within resin cement or composite resin28, adhesive at ceramic/cement interface28 or mixed adhesive/cohesive modes28. Representative specimens for each failure pattern were examined using a scanning electron microscope (SEM; XL 30 CP; Philips, Eindhoven, Netherlands) with an acceleration voltage of 15 kV and a working distance of 10 mm.
RESULTS
Mean ± standard deviation, minimum and maximum µTBS without and with thermocycling of test groups in MPa and P values are summarized in (Table 1). µTBS means were compared across all test groups using 3-way ANOVA model including the following factors (luting agent, surface treatment, storage time and interaction). The overall F-test was highly significant (p<0.0001), indicating differences in mean µTBS across at least one of the 3 factors. All individual factors were significant, (p<0.001).The interaction between surface treatment and luting agent and surface treatment and storage time were significant (P<0.001). However luting agent and storage time was not significant (p=0.208).
Table 1.
Mean±standard deviations (SD), minimum and maximum microtensile bond strength in MPa after 1 week and 1 month storage in water with thermocycling of test groups and P values
| Test groups | One week | One month/ Thermocycling | |||
|---|---|---|---|---|---|
| Mean±SD | Min. | Mean±SD | Min. | P values | |
| Max. | Max. | 1 week Vs 1 month/TC | |||
| GIAA | 18±4.3 | 11.4 | 7.3±3.5 | 2.3 | <.001* |
| 23.5 | 12.8 | ||||
| GISC | 17.3±3.9 | 11. 6 | 0 | - | Debonded |
| 22 | |||||
| GISCSI | 16.8±3.7 | 13.3 | 0 | - | Debonded |
| 23 | |||||
| MLAA | 18.7±2.5 | 14.8 | 10.±2.4 | 7.1 | .004* |
| 22.7 | 13.7 | ||||
| MLSC | 20.4±2.2 | 17.1 | 9.7±3 | 6.1 | <.001* |
| 23.7 | 15 | ||||
| MLSCSI | 31.8±3.4 | 26.6 | 15.4±2.8 | 11.3 | <.001* |
| 36.3 | 18.6 | ||||
| UNAA | 19.1±4.4 | 11.9 | 9.2±3.9 | 6.2 | .04* |
| 23.8 | 18.6 | ||||
| UNSC | 21.6±3.3 | 17.3 | 13.1±3.8 | 8.4 | .006* |
| 26.2 | 19.2 | ||||
| UNSCSI | 28.6±6.2 | 19.2 | 16.4±4.2 | 10.5 | <.001* |
| 36 | 24 | ||||
Group codes
GI: Ketac Cem Plus
ML: Multilink Automix
UN: RelyX Unicem
AA: Air borne particle abrasion
SC: Silica coating
SCSI: Silica coating and silane application
Multiple comparisons with Post Hoc Tukey-HSD test at α=0.05 revealed that, considering 3 surface treatment performed, SCSI significantly increased µTBS (p<0.05) compared to SC and AA. However, there was no statistically significant difference between SC and AA (p=0.26).
Considering 3 luting agents used, ML and UN resin cements showed significantly higher µTBS than the GIC cement (p<0.001). However, there was no significant difference in the µTBS of the 2 resin cements (p=0.37).
Considering aging condition, 30-day water storage and thermocycling significantly decreased µTBS compared to 1-week water storage (p<0.05). Groups GISC and GISCSI were spontaneously debonded.
Fracture patterns of all test groups are summarized in (Figure 3). After 1 week of storage in water, the debonded specimens showed mainly mixed failure pattern (Figure 4). Some specimens showed adhesive and cohesive failure (Figure 5). After 30 days of storage in water and thermocycling, the failure pattern was mainly adhesive with remnants of the luting cements still adhered to zirconia ceramic surface (Figure 6).
Figure 3.
Failure pattern of all test groups after 1 week and 1 month storage in water
| "Test groups Failure Pattern" | One week | One month/Thermalcycling | ||||
|---|---|---|---|---|---|---|
| Mixed | Adhesive | Cohesive | Mixed | Adhesive | Cohesive | |
| MLSCSI | 4 | 3 | 0 | 2 | 5 | 0 |
| MLSC | 2 | 3 | 2 | 1 | 6 | 0 |
| MLAA | 3 | 3 | 1 | 0 | 7 | 0 |
| UNSCSI | 3 | 4 | 0 | 2 | 5 | 0 |
| UNSC | 6 | 0 | 1 | 2 | 5 | 0 |
| UNAA | 3 | 4 | 0 | 2 | 5 | 0 |
| GISCSI | 1 | 5 | 1 | 0 | 7 | 0 |
| GISC | 3 | 3 | 1 | 0 | 7 | 0 |
| GIAA | 3 | 4 | 0 | 1 | 6 | 0 |
Group codes
GI: Ketac Cem Plus
ML: Multilink Automix
UN: RelyX Unicem
AA: Air borne particle abrasion
SC: Silica coating
SCSI: Silica coating and silane application
Figure 4.

Representative scanning electron microscope micrograph at 1,000x magnification showing mixed failure, adhesive at ceramic/cement interface and cohesive within the composite resin restorative material
Figure 5.

Representative scanning electron microscope micrograph at 1,000x magnification showing cohesive failure within the composite resin restorative material
Figure 6.

Representative scanning electron microscope micrograph at 1,000x magnification showing adhesive failure at ceramic/cement interface
DISCUSSION
Clinically, restorations are subjected to repeated thermal stress and mechanical fatigue due to masticatory forces. Therefore, one limitation of this study is that specimens were subjected only to thermal stress without mechanical fatigue. In addition, storage in water during 1 month might be too short to allow water saturation of the luting cements. It is likely that hydrolytic effects might affect the bond strength negatively after longer time of storage in water.
Microtensile bond strength test is more accurate than shear and tensile2,30. Because the small dimensions and small interfacial bonding zone of the specimens result in a more uniform distribution of the applied stresses2,10,30. Airborne-particle abrasion and silica coating are surface treatments4,22,26 recommended by most of the manufactures of zirconia ceramics and luting agents to improve bonding to zirconia ceramics. Therefore, these surface treatments were tested in this study.
A range of 10-13 MPa was suggested as the minimum range for acceptable clinical bonding15. Therefore the results of this study clearly indicated that, silica coating and silane application together with resin cements would ensure a durable resin bonding to this zirconia ceramic 15-16 Mpa.
Considering surface treatment, airborne-particle abrasion produced an activated microroughened zirconia surface, increased the bonding area and modifying the surface energy and wettability21,22. In case of silica coating, alumina particles modified with silica acid were sprayed under pressure10,29. This tribochemical reaction produces a high temperature contact area that can hold the silica layer on the ceramic surface3,6,10,29. These particles formed a base for micromechanical interlocking10. Because no silane was applied before bonding, bond strength was directly correlated to the quality of micromechanical interlocking with the silica coating layer. However, bond strength to zirconia ceramic after silica coating was not improved in comparison to airborne-particle abrasion.
The results of this study are in agreement with the findings of several studies21,22,25, which reported that bond strength to zirconia ceramics was not improved after silica coating compared to airborne-particle abrasion. Oyagüe, et al.21,22 (2009) and Kern12 (2009) reported that airborne-particle abrasion of zirconia ceramics produces a certain roughness, but only limited undercuts were produced, thus not improving bonding to zirconia. Matinlinna, et al.18 (2006), after energy-dispersive x-ray analysis of silica-coated zirconia ceramic, reported that silica-coverage originating from the coating particles appears not to have become embedded onto the hard zirconia surface, consequently bond strength was not improved after silica coating. Moreover, ultrasonic cleaning in distilled water might removed a significant amount of silica coating layer, consequently bond strength of resin cements to silica-coated zirconia ceramic was decreased, as reported by Nishigawa, et al.19 (2008). However, the results of this study were contradicting to the results of other studies3,15, which reported that silica coating improved bond strength to zirconia ceramics compared to airborne-particle abrasion. This difference in the results could be attributed to the fact that, Atsu, et al.3 (2006) used 125-mm Al2O3 for airborne-particle abrasion followed by 30-mm Al2O3 particles modified by silica. Panavia luting cement together with different ceramic primers were used for bonding. On the other hand Lüthy, et al.15 (2006) used the Rocetac system for silica coating, which combines 110 mm Al2O3 for airborne-particle abrasion followed by 110-mm Al2O3 particles modified by silica. Rounded rods were bonded to zirconia ceramics instead of restorative composite resin. Moreover both studies used shear test. In the present study, 50-mm Al2O3 was used for airborne-particle abrasion followed by 30-mm Al2O3 particles modified by silica and a µTBS test were employed.
Silica coating and silane application significantly increased bond strength compared to airborne-particle abrasion or silica coating alone, as reported in several studies2,3,10. Silane coupling agent did not promote adequate bonding to zirconia ceramics, as these ceramics contain minimal or no silica content9,12,14. Therefore, silica coating of zirconia ceramics is a prerequisite for durable siloxane bonding, as it leave a physically and chemically active outer surface layer2,18. Silane coupling agent wets the adherent, increases its surface energy and makes it accessible for effective bonding18. Moreover, it is capable of forming covalent bond at silica coated ceramic/resin cement interface through formation of silanol groups18,26,29. Therefore, after silica coating and silanization, bond strength was based on both micromechanical interlocking plus chemical adhesion due to silane application18,26,29.
Variations in chemical composition, wetting capacity, viscosity and mechanical properties for each luting cement could be responsible for variations in the bonding capacity to zirconia ceramics9,15,17,20,28. According to the manufacturer, RelyX Unicem contains methacrylate monomers, adhesive phosphate monomer and silanated fillers in its chemical composition. Adhesive phosphate monomer enhanced self bonding to zirconia ceramics especially after silica coating and silane application as reported in several studies12,15,20. Ketac Cem Plus contains BisGMA, HEMA and zirconia filler. Several studies have reported that bond strengths of BisGMA containing resin cements were dramatically decreased after artificial aging12,15 due to their remarkable weak mechanical properties.
Multilink Automix contains no adhesive phosphate monomer. However, it contains dimethacrylate, HEMA and silica filler. Dimethacrylate and HEMA improved its mechanical properties. The improved mechanical properties could be responsible for high bond strength results of Multilink Automix. Nothdurft, et al.20 (2009) found no significance difference in the mean bond strength of Multilink Automix 21.2 MPa and RelyX Unicem 23.1 MPa to zirconia ceramics after different surface treatments.
RelyX Unicem and Multilink Automix have better mechanical properties than Ketac Cem Plus. According to the manufacturers flexural strength for RelyX Unicem (75 MPa) and Multilink Automix (70 MPa) are in the same range. However it is higher than that of Ketac Cem Plus (31.6 MPa). Flexural strength is an indicator for the mechanical properties of each luting agent. Luting cements with high mechanical properties are more resistant to aging conditions15. Therefore, variations in the mechanical properties of the 3 luting cements used could be another contributing factor for bond strength results as reported in other studies15,17.
In in vitro studies, water storage and thermocycling are two important factors that decrease the bond strength4,26,27. Therefore, 1 month storage in water and thermal cycling for 7,500 cycles was used as aging regime to simulate clinical conditions. After 30 days of storage in water and thermocycling, µTBS were significantly decreased in all groups. This decrease in bond strength might be due to degradation of the luting cement itself4,17,27 and the hydrolytic effect of water at the luting cement/ceramic interface9,27.
Moreover, mismatch between the coefficient of thermal expansion of the bonded specimens (zirconia ceramic, luting agent and composite resin) could result in hoop stress during thermocycling27. Another factor could be the fact that silanized surfaces were unstable in contact with moisture as reported by Derand, et al.9 (2005). Accumulation of negative effect of water, thermocycling and instability of silane could be responsible for the decrease of bond strength for all test groups.
The initial high bond strength results were reflected on the failure pattern of debonded specimens as examined by optical reflection microscope and confirmed by scanning electron microscopy. All groups showed mainly mixed failure pattern or adhesive failure while cohesive failure was minimal. Cohesive failure within composite resin could be due to the initiation of microcracks during cutting of the specimens24. Therefore, in this study, specimens with apparent microcracks under stereomicroscopic examination were discarded.
After 30 days of storage in water and thermocycling, the failure pattern was mainly adhesive indicating a decrease in the bond strength due to the hydrolytic effect of water, hoop stress due to thermocycling and degradation of the luting resin itself.
The general outcome of this study suggests that although conventional cements could be used for cementation of zirconia ceramics, resin cements are preferred for long-term bond durability. Bonding techniques based on micromechanical interlocking and chemical adhesion using silanes are preferred than other techniques.
CONCLUSIONS
Within the limitations of this study, the following conclusions were drawn:
Silica coating and silane application significantly improved µTBS compared to silica coating or airborne-particle abrasion.
There was no significance difference in the bond strength after using self-adhesive resin cement or multistep adhesive resin cement.
Both adhesive resin cements significantly increased µTBS compared to RMGIC.
ACKNOWLEDGMENT
The author thanks Prof. Dr. Hassan Soltan, Faculty of Engineering, Mansoura University for his help with statistical analysis of the results. The author thanks Mr. F. Lehmann Dipl.-Ing., Department of Prosthodontics, Propaedeutics and Dental Materials, School of Dentistry, Christian-Albrechts University at Kiel, Germany for his help with SEM micrograph. The author also thanks Ivoclar Vivadent and 3M ESPE for supplying all the materials with no cost.
REFERENCES
- 1.Aboushelib MN, Kleverlaan CJ, Feilzer AJ. Selective infiltrationetching technique for a strong and durable bond of resin cements to zirconia-based materials. J Prosthet Dent. 2007;98:379–388. doi: 10.1016/S0022-3913(07)60123-1. [DOI] [PubMed] [Google Scholar]
- 2.Amaral R, Ozcan M, Bottino MA, Valandro LF. Microtensile bond strength of a resin cement to glass infiltrated zirconia reinforced ceramic: the effect of surface conditioning. Dent Mater. 2006;22:283–290. doi: 10.1016/j.dental.2005.04.021. [DOI] [PubMed] [Google Scholar]
- 3.Atsu SS, Kilicarslan MA, Kucukesmen HC, Aka PS. Effect of zirconium-oxide ceramic surface treatments on the bond strength to adhesive resin. J Prosthet Dent. 2006;95:430–436. doi: 10.1016/j.prosdent.2006.03.016. [DOI] [PubMed] [Google Scholar]
- 4.Blatz MB, Chiche G, Holst S, Sadan A. Influence of surface treatment and simulated aging on bond strengths of luting agents to zirconia. Quintessence Int. 2007;38:745–753. [PubMed] [Google Scholar]
- 5.Blatz MB, Sadan A, Martin J, Lang B. In vitro evaluation of shear bond strengths of resin to densely-sintered high-purity zirconium-oxide ceramic after long-term storage and thermal cycling. J Prosthet Dent. 2004;91:356–362. doi: 10.1016/j.prosdent.2004.02.001. [DOI] [PubMed] [Google Scholar]
- 6.Bottino MA, Valandro LF, Scotti R, Buso L. Effect of surface treatments on the resin bond to zirconium-based ceramic. Int J Prosthodont. 2005;18:60–65. [PubMed] [Google Scholar]
- 7.Cehreli MC, Kökat AM, Akça K. CAD/CAM Zirconia vs. slip-cast glass-infiltrated Alumina/Zirconia all-ceramic crowns: 2-year results of a randomized controlled clinical trial. J Appl Oral Sci. 2009;17:49–55. doi: 10.1590/S1678-77572009000100010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Cavalcanti AN, Foxton RM, Watson TF, Oliveira MT, Giannini M, Marchi GM. Bond strength of resin cements to a zirconia ceramic with different surface treatments. Oper Dent. 2009;34:280–287. doi: 10.2341/08-80. [DOI] [PubMed] [Google Scholar]
- 9.Derand T, Molin M, Kvam K. Bond strength of composite luting cement to zirconia ceramic surfaces. Dent Mater. 2005;21:1158–1162. doi: 10.1016/j.dental.2005.02.005. [DOI] [PubMed] [Google Scholar]
- 10.Della Bona A, Borba M, Benetti P, Cecchetti D. Effect of surface treatments on the bond strength of a zirconia-reinforced ceramic to composite resin. Braz Oral Res. 2007;21:10–15. doi: 10.1590/s1806-83242007000100002. [DOI] [PubMed] [Google Scholar]
- 11.Jevnikar P, Krnel K, Kocjan A, Funduk N, Kosmac T. The effect of nano-structured alumina coating on resin-bond strength to zirconia ceramics. Dent Mater. 2010;29:688–696. doi: 10.1016/j.dental.2010.03.013. [DOI] [PubMed] [Google Scholar]
- 12.Kern M. Resin bonding to oxide ceramics for dental restorations. J Adhes Sci Technol. 2009;23:1097–1111. [Google Scholar]
- 13.Kitayama S, Nikaido T, Maruoka R, Zhu L, Ikeda M, Watanabe A, et al. Effect of an internal coating technique on tensile bond strengths of resin cements to zirconia ceramics. Dent Mater J. 2009;28:446–453. doi: 10.4012/dmj.28.446. [DOI] [PubMed] [Google Scholar]
- 14.Kitayama S, Nikaido T, Takahashi R, Zhu L, Ikeda M, Foxton RM, et al. Effect of primer treatment on bonding of resin cements to zirconia ceramic. Dent Mater. 2010;26:426–432. doi: 10.1016/j.dental.2009.11.159. [DOI] [PubMed] [Google Scholar]
- 15.Lüthy H, Loeffel O, Hammerle CH. Effect of thermocycling on bond strength of luting cements to zirconia ceramic. Dent Mater. 2006;22:195–200. doi: 10.1016/j.dental.2005.04.016. [DOI] [PubMed] [Google Scholar]
- 16.Magne P, Paranhos MP, Burnett LH., Jr New zirconia primer improves bond strength of resin-based cements. Dent Mater. 2010;26:345–352. doi: 10.1016/j.dental.2009.12.005. [DOI] [PubMed] [Google Scholar]
- 17.Marchan S, Coldero L, Whiting R, Barclay S. In vitro evaluation of the retention of zirconia-based ceramic posts luted with glass ionomer and resin cements. Braz Dent J. 2005;3:213–217. doi: 10.1590/s0103-64402005000300008. [DOI] [PubMed] [Google Scholar]
- 18.Matinlinna JP, Heikkinen T, Ozcan M, Lassila LV, Vallittu PK. Evaluation of resin adhesion to zirconia ceramic using some organosilanes. Dent Mater. 2006;22:824–831. doi: 10.1016/j.dental.2005.11.035. [DOI] [PubMed] [Google Scholar]
- 19.Nishigawa G, Maruo Y, Irie M, Oka M, Yoshihara K, Minagi S, et al. Ultrasonic cleaning of silica-coated zirconia influences bond strength between zirconia and resin luting material. Dent Mater J. 2008;27:842–848. doi: 10.4012/dmj.27.842. [DOI] [PubMed] [Google Scholar]
- 20.Nothdurft FP, Motter PJ, Pospiech PR. Effect of surface treatment on the initial bond strength of different luting cements to zirconium oxide ceramic. Clin Oral Investig. 2009;13:229–235. doi: 10.1007/s00784-008-0222-8. [DOI] [PubMed] [Google Scholar]
- 21.Oyagüe RC, Monticelli F, Toledano M, Osorio E, Ferrari M, Osorio R. Effect of water aging on microtensile bond strength of dual-cured resin cements to pre-treated sintered zirconium-oxide ceramics. Dent Mater. 2009;25:392–399. doi: 10.1016/j.dental.2008.09.002. [DOI] [PubMed] [Google Scholar]
- 22.Oyagüe RC, Monticelli F, Toledano M, Osorio E, Ferrari M, Osorio R. Influence of surface treatments and resin cement selection on bonding to densely-sintered zirconium-oxide ceramic. Dent Mater. 2009;25:172–179. doi: 10.1016/j.dental.2008.05.012. [DOI] [PubMed] [Google Scholar]
- 23.Phark JH, Duarte S, Jr, Blatz M, Sadan A. An in vitro evaluation of the long-term resin bond to a new densely sintered high-purity zirconium-oxide ceramic surface. J Prosthet Dent. 2009;101:29–38. doi: 10.1016/S0022-3913(08)60286-3. [DOI] [PubMed] [Google Scholar]
- 24.Scherrer SS, Cesar PF, Swain MV. Direct comparison of the bond strength results of the different test methods: a critical literature review. Dent Mater. 2010;26:e78–e93. doi: 10.1016/j.dental.2009.12.002. [DOI] [PubMed] [Google Scholar]
- 25.Uo M, Sjögren G, Sundh A, Goto M, Watari F, Bergman M. Effect of surface condition of dental zirconia ceramic (Denzir) on bonding. Dent Mater J. 2006;25:626–631. doi: 10.4012/dmj.25.626. [DOI] [PubMed] [Google Scholar]
- 26.Valandro LF, Ozcan M, Amaral R, Leite FP, Bottino MA. Microtensile bond strength of a resin cement to silica-coated and silanized In-Ceram Zirconia before and after aging. Int J Prosthodont. 2007;20:70–72. [PubMed] [Google Scholar]
- 27.Wegner SM, Gerdes W, Kern M. Effect of different artificial aging conditions on ceramic-composite bond strength. Int J Prosthodont. 2002;15:267–272. [PubMed] [Google Scholar]
- 28.Wolfart M, Lehmann F, Wolfart S, Kern M. Durability of the resin bond strength to zirconia ceramic after using different surface conditioning methods. Dent Mater. 2007;23:45–50. doi: 10.1016/j.dental.2005.11.040. [DOI] [PubMed] [Google Scholar]
- 29.Xible AA, Jesus Tavarez RR, Araujo Cdos R, Bonachela WC. Effect of silica coating and silanization on flexural and compositeresin bond strengths of zirconia posts: an in vitro study. J Prosthet Dent. 2006;95:224–229. doi: 10.1016/j.prosdent.2005.12.010. [DOI] [PubMed] [Google Scholar]
- 30.Yesil ZD. Microtensile bond strength testing of resin cements. Inter Journal Adhes Adhes. 2009;29:352–355. [Google Scholar]