

Abstract
Purpose
High rate of malunion and non union in displaced fracture clavicle treated conservatively lead to use of different types of internal fixation methods which also were found to be associated with various complications. Moreover their superiority over conservative treatment has not been established. This study was designed to compare clinical outcome of conservative treatment with external fixator in cases with displaced midshaft clavicle fractures.
Methods
Fifty adult consenting cases of acute midshaft fracture clavicle, displaced >15 mm were included. Twenty five cases were allotted to conservative (group A) and external fixator (group B) each. In group A treatment was given in form of clavicle brace. In group B schanz pins were inserted obliquely between supero-inferior and anterior-posterior direction and connected with rod. The outcome was measured by Constant score, union time and complications.
Results
Mean radiographic union time in group A was 23.45 ± 1.40 weeks (with 8% non union and 80% malunion) and in group B it was 9.36 ± 1.49 weeks. Mean Constant score at 6 months in group A was 78.28 ± 6.45 and in group B 92.72 ± 1.48. Mean shortening at 6 months in group A was 19.36 mm. In group B shortening at 6 months was noticed in three cases (6, 5, 6 mm).
Conclusion
Close reduction of acute fracture mid clavicle and application of external fixator is a simple procedure providing the benefits of rigid fixation and undisturbed fracture environment. Pain relief is faster, union time is shorter and there are no hardware related problems.
Keywords: Comparison fracture, Clavicle conservative, External fixator
1. Introduction
Clavicle fracture is one of the most common fractures in adults. Majority of clavicle fractures are situated in the middle (81%).1
All methods used for treatment of displaced fractures of midshaft clavicle have shortcomings. Conservative treatment of displaced fracture clavicle leads to shortening of clavicle, pain, loss of strength, rapid fatigue, hyperaesthesia of the hand and arm, difficulty sleeping on the affected side and aesthetic complications.2–6 More than 9.7% shortening of clavicle of its original length is associated with poor outcome.7 There is evident association between shortening and non union.3 Pseudarthrosis (upto 5%),8 high rate of malunion (upto two thirds)9 and non union (upto 15%)3 have been reported with displaced fracture treated conservatively. Many patients remain symptomatic for long time with increased risk of prolonged sequels at 9–10-year follow up.10
In cases of displaced or comminuted fractures operative treatment is reported to be better than conservative treatment2 but every fixation method has associated complications.
Intra-medullary devices are difficult to insert in clavicle due to inherent gentle s shape of the bone and small medullary canal. They can be associated with complications such as hardware failure, nerve injury, skin breakdown11–13 hardware migration and neurovascular injury.14,15 Without static locking mechanism there can be shortening of the clavicle in comminuted fractures.12,13
Plate fixation is associated with infection (5–22%), hardware irritation (9–64%), subcutaneous prominence, poor cosmesis due to postoperative scar, resurgery to remove plate, refracture after removal of plate and even non union after plating.2,3,16,17
Recently reported studies and cochrane review have not been able to establish clear superiority of operative over conservative management in fracture clavicle.18–20 This study was conducted to evaluate the clinical outcome and complications of fracture clavicle treated by external fixator in comparison to conservative method.
1.1. Research question
Does acute displaced fracture midshaft clavicle treated by external fixator result in better outcome than conservative method.
2. Methods
This study was conducted between October 2010 and April 2012. Fifty adult patients with midshaft clavicle fractures were enrolled in this study which was designed as a case control study. Institutional approval was obtained from the local Ethics Committee before initiation of the study. Informed consent was obtained from cases.
All consenting adult patients with less than one week old closed midshaft fracture of clavicle (Fig. 1) were included in the study. The fractures that were completely displaced, comminuted or with shortening of more than 15 mm (in comparison to normal side) were included.
Fig. 1.

Shows displaced fracture midshaft clavicle.
Open fracture clavicle, associated neurovascular injury, undisplaced fracture, fracture of medial or lateral ends, non union, malunion, medically unfit and non-consenting cases were excluded.
The conservative treatment was given in form of clavicle brace application. The affected upper limb was supported in an arm pouch. The clavicle brace was discontinued at 6 weeks but arm pouch sling was continued till union was ascertained. Pendulum shoulder exercise was initiated when pain resolved. Range of motion exercises were initiated after union was ascertained.
2.1. Technique of clavicle external fixation
Patient was put in supine position with a sandbag between the scapulae. Closed reduction was done under image intensifier guidance (antero-posterior and 45° cephalic tilt in antero-posterior) and was provisionally fixed with Kirschner wires. Two schanz pins (3.5 mm) were inserted on medial fragment from anterior to posterior in horizontal plane in slightly cephalad direction to avoid the injury to the pleural dome. On the lateral fragment two schanz pins were inserted obliquely between supero-inferior and anterior-posterior direction to avoid neurovascular structures. The pins were connected with the appropriate length of ‘gentle S’ shaped rod to complete the construct (Fig. 2). The limb was supported in an arm pouch sling. At each follow up pin sites and fixator stability was checked clinically and radiologically, till union. The fixator was removed when radiological union was evident (Fig. 3). The fracture was considered to be united when there was no tenderness and the fracture line was not visible or callous formation was seen on X-ray. Gentle pendulum exercise of the shoulder in the arm pouch was initiated at second day of surgery. At 4 weeks active range of motion of the shoulder was allowed but abduction was restricted to 80°. At 8 weeks active range of motion in all planes was allowed.
Fig. 2.

Shows external fixator on right clavicle after close reduction.
Fig. 3.

Shows union without shortening of fracture clavicle with external fixator.
Follow up was done at 2, 4, 8, 12, 16, 20 weeks and finally at 6 months for both the groups. The outcome was measured in terms of Constant and Murley score, union time and complications. The functional outcome by Constant and Murley score was performed at 6 months. The length of fractured clavicle was also measured at final follow up to calculate shortening.
3. Results
Out of 25 cases in each group, there were 96% male, 4% female in group A and 84% male, 16% female in group B. The mean age was (32.6 ± 6.43) in group A and (30.56 ± 7.10) in group B. Seventy six percent cases in group A and eighty percent cases in group B were younger than 39 years of age (Table 1). There were 8 cases (32%) of right side and 17 cases (68%) of left side fracture in both groups.
Table 1.
Shows demographic distribution.
| Age in years | Group A | % | Group B | % |
|---|---|---|---|---|
| 20–29 | 9 | 36% | 10 | 40% |
| 30–39 | 10 | 40% | 10 | 40% |
| 40–49 | 6 | 20% | 5 | 24% |
| Total | 25 | 100% | 25 | 100% |
The most common cause of fracture in both the groups was road traffic accident (72% cases in group A and 76% cases in group B). Fall on the affected shoulder was the cause of fracture in 12% cases in group A and 16% cases in group B. In group A in 16% cases and in group B in 8% cases cause of fracture was indirect injury due to fall on outstretched hand. Five cases had associated injuries due to road traffic accident, one had humerus fracture and one had head injury and 3 cases had ribs fracture.
Mean time of radiographic union in group A was 23.45 ± 1.40 weeks and in group B was 9.36 ± 1.49 weeks. In group A fracture union was documented in 16% cases by 16 weeks, 76% cases by 20 weeks and 8% resulted in non union. In group B union was documented in 72% cases by 8 weeks and in rest of 28% cases also fracture united by 12 weeks (Table 2).
Table 2.
Shows time of union.
| Time of union (in weeks) | Group A | % | Group B | % |
|---|---|---|---|---|
| 8 | 0 | 0 | 18 | 72% |
| 12 | 0 | 0 | 7 | 28% |
| 16 | 4 | 16% | 0 | |
| 20 | 19 | 76% | 0 |
In group A, 80% cases resulted in malunion (Fig. 4) and 8% cases had non union whereas Group B patients did not have any complication (Table 3). The cases in group A required analgesics till first follow up at two weeks but in group B analgesic support was not required beyond third postoperative day.
Fig. 4.

Shows malunion with shortening of fracture clavicle.
Table 3.
Shows complications.
| Complications | Group A | Percent (group A) | Group B | Percent (group B) |
|---|---|---|---|---|
| Malunion | 20 | 80% | 0 | 0% |
| Non union | 2 | 8% | 0 | 0 |
Mean pre-operative Constant and Murley score in group A was 30.56 ± 1.29 and group B was 32.24 ± 2.45. At 6 month follow up Constant and Murley score in group A was 78.28 ± 6.45 and in group B was 92.72 ± 1.48 (Table 4). After six month follow up, the difference in functional outcome in both groups was statistically significant (p = 0.00).
Table 4.
Shows the functional outcome as assessed by Constant and Murley score.
| Functional outcome at 6 months | Group A | % | Group B | % |
|---|---|---|---|---|
| Excellent | 0 | 0% | 25 | 100% |
| Good | 17 | 68% | 0 | 0% |
| Fair | 5 | 20% | 0 | 0% |
| Poor | 3 | 12% | 0 | 0% |
| Total | 25 | 100% | 25 | 100% |
In group A the mean pre treatment shortening was 23.28 mm and mean shortening at 6 months was 19.36 mm. In group B the mean pre treatment shortening was 25.76 mm and shortening at 6 months was noticed in three cases (6, 5, 6 mm).
4. Discussion
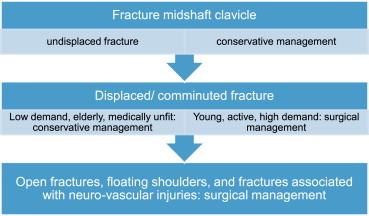
Most of the fractures of clavicle unite conservatively but surgery is indicated at the first place in open fractures, floating shoulders, and fractures associated with neurovascular injuries.21 Surgery should also be considered for fractures which are grossly displaced and severely comminuted as they have propensity to land up in non union [Table 5].22,23
Table 5.
Treatment recommendation for fracture midshaft clavicle.
Recent studies which have compared conservative with operative treatment of displaced midshaft fracture clavicle, have documented better union rates and early functional return with fixation and association of malunion and non union with conservative treatment [Table 6].19,24–29
Table 6.
Shows recent studies comparing conservative with surgical treatment.
| Robinson CM. J Bone Joint Surg Am. 2013 Sep 4; 95(17):1576–84 | Prospective randomised multi centric study comparing plating with conservative treatment | Plating reduces chances of non union and results in better functional outcome but can not be recommended for every case |
| Virtanen KJ et al J Bone Joint Surg Am. 2012 Sep 5; 94(17):1546–53 | Prospective randomised study comparing conservative with plate fixation | Higher non union rates at one year in conservatively treated group |
| McKee RC. J Bone Joint Surg Am. 2012 Apr 18; 94(8):675–84. | Meta analysis of conservative verses operative treatment | Operative treatment has significantly lower rate of non union and symptomatic malunion with early return of function |
| Kaisa J Virtanen et al Acta Orthopaedica 2012; 83(1): 65–73 | A systematic review of 1190 patients from the literature | Patients treated surgically had better functional outcome in short term. Surgery to be reserved for young active patients who want to return to previous activity level early. |
| Fardin Mirzatolooei. Acta Orthop Traumatol Turc. 2011; 45(1):34–40 | Prospective randomised trial comparing plating with conservative treatment | Open reduction and plating of comminuted fracture of clavicle has better outcome than conservative treatment |
| Vander Have KL. J Pediatr Orthop. 2010 Jun; 30(4):307–12 | Comparison of conservative treatment with plating in adolescents (case control study) | Plating group was found to have shorter union time, better pain relief and less complications. |
| Altamimi SA, McKee MD; Canadian Orthopaedic Trauma Society. J Bone Joint Surg Am. 2008 Mar; 90 suppl 2 Pt 1:1–8 | Prospective randomised multi centric study comparing plating with conservative treatment | At one year surgically treated had better functional outcome and lower rates of malunion and non union |
4.1. Union
To achieve union in anatomic position, fracture has to be reduced anatomically and fixed in this position till union occurs. We found that closed reduction of acute midshaft clavicle fracture is not difficult. As clavicle can be palpated through out its length and can be visualised per-operative by image intensifier (antero-posterior and 45° cephalic tilt in antero-posterior), acceptable reduction can be achieved. Application of external fixator is a simple procedure and it is capable in maintaining fracture in reduced position till union. We documented significantly shorter union time in fixator group than conservative group in this study. All the cases in external fixator group went on to have solid union by 12 weeks and in 72% cases union was noticed by 8 weeks. Excellent outcome with 100% union rate has been reported by use of external fixator in cases of established non union of fracture clavicle by Lodhi et al.30 But in conservative group in this study union was noticed in only 82% cases that too by 20 weeks and 8% cases in this group resulted in non union.
The inherent advantage of any closed reduction is undisturbed fracture haematoma and intact soft tissue envelop that provides a perfect biological milieu for fracture union. The combination of advantages of closed reduction and sound fixation leads shorter union time in external fixator group as noticed in this study.
Clavicle by virtue of its compact structure offers good hold of schanz screws. We inserted schanz screws in slightly different planes across fracture site to improve the construct biomechanically. There was no instance of failure of fixator in this study.
4.2. Pain relief
Because of minimal surgical invasion and immobilisation of fracture, all cases in the fixator group had substantial pain relief on first postoperative day and no need of analgesics after 3 days. But the group treated conservatively had pain for long time. Pain relief is an important factor for initiation of rehabilitation program hence preventing stiffness of shoulder and regaining strength around shoulder girdle. Because of pain relief in external fixator group pendular shoulder exercises could be initiated in immediate postoperative period.
4.3. Functional outcome and disabilities
We noticed that cases in external fixator group regained near normal shoulder function and all the cases had excellent Constant score whereas none of the cases in conservative group reached excellent constant score. Better functional outcome in external fixator group is depicted by statistically significant difference in mean Constant score of 92.72 ± 1.48 in external fixator group as compared to 78.28 ± 6.45 in conservative group at the end of six months.
4.4. Implant removal
Patients on external fixator had to undergo fixator removal but it is an out patient procedure with minimal pain. In many studies reported with plating, the rate of implant removal is high either due to hardware problems (breakage, failure, irritation) or routinely.17 Removal of plate requires surgical invasion, anaesthesia and admission hence increasing the cost of treatment. Cosmesis is also not a problem in external fixator as there is no surgical scar or palpable or visible bony bump which is present in displaced fracture managed conservatively.
4.5. Complications
Out of all potential complications, malunion associated with shortening is of utmost importance as it is associated with impaired biomechanics of the shoulder girdle by scapular winging, change in orientation of glenoid and sterno-clavicular joints.9,31 All the cases in group A had significant shortening at 6 months with a mean of 19.36 mm. Where as minimal shortening was also noticed in three cases of comminuted fracture of fixator group (6, 5 and 6 mm) but this did not cause any hindrance to functional return. Hill3 reported more than 20 mm shortening and Di Giorgi more than 9.7% shortening of length of clavicle as cut of leading to unsatisfactory outcome. The universal problem with external fixator group was difficulty with normal clothing. Displaced midshaft clavicle fractures managed conservatively have been reported to be associated with high rate of malunion and non union2–7 as also in this study. There were two cases of non union and shortening with malunion was a universal phenomena in the conservative group.
Any midshaft fracture clavicle which is comminuted and/or grossly displaced with shortening more than 15 mm as compared to the opposite side in young active adult is a suitable case for surgical fixation. Use of external fixator in such situation is valid alternative to open reduction and internal fixation. Because of paucity of literature for this technique as well as small sample size of this study it is difficult to establish superiority of this method over other methods of fixation. But because of inherent advantages like simplicity of procedure, faster pain relief, shorter union time and lesser chances of hardware related complications, use of external fixator in displaced midshaft clavicle fracture can become mainstay treatment. The small sample size is a drawback of the study.
5. Conclusion
Close reduction of acute fracture midshaft clavicle and fixation with external fixator is a simple procedure. It provides the benefits of conservative treatment as the fracture environment is undisturbed and also provides the benefits of implant fixation in terms of maintenance of reduction. Pain relief is faster, union time is shorter and there are no hardware related complications. It has potential to become a main line treatment option for displaced midshaft fracture of clavicle.
Conflicts of interest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
- 1.Postacchini F., Gumina S., De Santis P., Albo F. Epidemiology of clavicle fractures. J Shoulder Elbow Surg. 2002 Sep–Oct;11(5):452–456. doi: 10.1067/mse.2002.126613. [DOI] [PubMed] [Google Scholar]
- 2.Zlowodzki M., Zelle B.A., Cole P.A., Jeray K., McKee M.D. Treatment of acute midshaft clavicle fractures: systematic review of 2144 fractures: on behalf of the Evidence-Based Orthopaedic Trauma Working Group. J Orthop Trauma. 2005;19:504–507. doi: 10.1097/01.bot.0000172287.44278.ef. [DOI] [PubMed] [Google Scholar]
- 3.Hill J.M., McGuire M.H., Crosby L.A. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br. 1997;79:537–539. doi: 10.1302/0301-620x.79b4.7529. [DOI] [PubMed] [Google Scholar]
- 4.McKee M.D., Pedersen E.M., Jones C. Deficits following nonoperative treatment of displaced midshaft clavicular fractures. J Bone Joint Surg Am. 2006;88:35–40. doi: 10.2106/JBJS.D.02795. [DOI] [PubMed] [Google Scholar]
- 5.Nordqvist A., Redlund-Johnell I., von S.A., Petersson C.J. Shortening of clavicle after fracture. Incidence and clinical significance, a 5-year follow-up of 85 patients. Acta Orthop Scand. 1997;68:349–351. doi: 10.3109/17453679708996175. [DOI] [PubMed] [Google Scholar]
- 6.Gossard J.M. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br. 1998;80:558. [PubMed] [Google Scholar]
- 7.De Giorgi Silvana, Notarnicola Angela, Tafuri Silvio, Solarino Giuseppe, Moretti Lorenzo, Moretti Biagio. Conservative treatment of fractures of the clavicle. BMC Res Notes. 2011;4:333. doi: 10.1186/1756-0500-4-333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lenza M., Belloti J.C., Andriolo R.B., Gomes Dos Santos J.B., Faloppa F. Conservative interventions for treating middle third clavicle fractures in adolescents and adults. Cochrane Database Syst Rev. 2009;2:CD007121. doi: 10.1002/14651858.CD007121.pub2. [DOI] [PubMed] [Google Scholar]
- 9.Hillen R.J., Burger B.J., Poll R.G., de G.A., Robinson C.M. Malunion after midshaft clavicle fractures in adults. Acta Orthop. 2010;81:273–279. doi: 10.3109/17453674.2010.480939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Nowak J., Holgersson M., Larsson S. Can we predict longterm sequelae after fractures of the clavicle based on initial findings? A prospective study with nine to ten years of followup. J Shoulder Elbow Surg. 2004 Sep–Oct;13(5):479–486. doi: 10.1016/j.jse.2004.01.026. [DOI] [PubMed] [Google Scholar]
- 11.Ring D., Holovacs T. Brachial plexus palsy after intramedullary fixation of a clavicular fracture. A report of three cases. J Bone Joint Surg Am. 2005;87(8):1834–1837. doi: 10.2106/JBJS.D.02919. [DOI] [PubMed] [Google Scholar]
- 12.Kettler M., Schieker M., Braunstein V., König M., Mutschler W. Flexible intramedullary nailing for stabilization of displaced midshaft clavicle fractures: technique and results in 87 patients. Acta Orthop. 2007;78(3):424–429. doi: 10.1080/17453670710014022. [DOI] [PubMed] [Google Scholar]
- 13.Strauss E.J., Egol K.A., France M.A., Koval K.J., Zuckerman J.D. Complications of intramedullary Hagie pin fixation for acute midshaft clavicle fractures. J Shoulder Elbow Surg. 2007;16(3):280–284. doi: 10.1016/j.jse.2006.08.012. [DOI] [PubMed] [Google Scholar]
- 14.Sethi G.K., Scott S.M. Subclavian artery laceration due to migration of a Hagie pin. Surgery. 1976;80(5):644–646. [PubMed] [Google Scholar]
- 15.Jubel A., Andermahr J., Schiffer G., Tsironis K., Rehm K.E. Elastic stable intramedullary nailing of midclavicular fractures with a titanium nail. Clin Orthop Relat Res. 2003;408:279–285. doi: 10.1097/00003086-200303000-00037. [DOI] [PubMed] [Google Scholar]
- 16.Canadian Orthopaedic Trauma Society Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicenter, randomized clinical trial. J Bone Joint Surge Am. 2007;89:1–10. doi: 10.2106/JBJS.F.00020. [DOI] [PubMed] [Google Scholar]
- 17.Frans-Jasper G., Wijdicks Olivier A.J., der Meijden Van, Millett Peter J., Verleisdonk Egbert J.M.M., Houwert R. Marijn. Systematic review of the complications of plate fixation of clavicle fractures. Arch Orthop Trauma Surg. 2012;132:617–625. doi: 10.1007/s00402-011-1456-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rehn C.H., Kirkegaard M., Viberg B., Larsen M.S. Operative versus nonoperative treatment of displaced midshaft clavicle fractures in adults: a systematic review. Eur J Orthop Surg Traumatol. 2013 Dec 10 doi: 10.1007/s00590-013-1370-3. [published on line] [DOI] [PubMed] [Google Scholar]
- 19.McKee R.C., Whelan D.B., Schemitsch E.H., McKee M.D. Operative versus nonoperative care of displaced midshaft clavicular fractures: a meta-analysis of randomized clinical trials. J Bone Joint Surg Am. 2012 Apr 18;94(8):675–684. doi: 10.2106/JBJS.J.01364. [DOI] [PubMed] [Google Scholar]
- 20.Lenza M., Buchbinder R., Johnston R.V., Belloti J.C., Faloppa F. Surgical versus conservative interventions for treating fractures of the middle third of the clavicle. Cochrane Database Syst Rev. 2013 Jun 6;6:CD009363. doi: 10.1002/14651858.CD009363.pub2. [DOI] [PubMed] [Google Scholar]
- 21.Jeray K.J. Acute midshaft clavicular fracture. J Am Acad Orthop Surg. 2007;15:239–248. doi: 10.5435/00124635-200704000-00007. [DOI] [PubMed] [Google Scholar]
- 22.Brinker M.R., Edwards T.B., O’Connor D.P. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am. 2005;87:676–677. doi: 10.2106/00004623-200503000-00034. [DOI] [PubMed] [Google Scholar]
- 23.Khan L.A., Bradnock T.J., Scott C., Robinson C.M. Fractures of the clavicle. J Bone Joint Surg Am. 2009;91:447–460. doi: 10.2106/JBJS.H.00034. [DOI] [PubMed] [Google Scholar]
- 24.Robinson C.M., Goudie E.B., Murray I.R. Open reduction and plate fixation versus nonoperative treatment for displaced midshaft clavicular fractures: a multicenter, randomized, controlled trial. J Bone Joint Surg Am. 2013 Sep 4;95(17):1576–1584. doi: 10.2106/JBJS.L.00307. [DOI] [PubMed] [Google Scholar]
- 25.Virtanen K.J., Remes V., Pajarinen J., Savolainen V., Björkenheim J.M., Paavola M. Sling compared with plate osteosynthesis for treatment of displaced midshaft clavicular fractures: a randomized clinical trial. J Bone Joint Surg Am. 2012 Sep 5;94(17):1546–1553. doi: 10.2106/JBJS.J.01999. [DOI] [PubMed] [Google Scholar]
- 26.Virtanen Kaisa J., Malmivaara Antti O.V., Remes Ville M., Paavola Mika P. Operative and nonoperative treatment of clavicle fractures in adults; a systematic review of 1,190 patients from the literature. Acta Orthop. 2012;83(1):65–73. doi: 10.3109/17453674.2011.652884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Mirzatolooei Fardin. Comparison between operative and nonoperative treatment methods in the management of comminuted fractures of the clavicle. Acta Orthop Traumatol Turc. 2011;45(1):34–40. doi: 10.3944/AOTT.2011.2431. [DOI] [PubMed] [Google Scholar]
- 28.Vander Have K.L., Perdue AM., Caird M.S., Farley F.A. Operative versus nonoperative treatment of midshaft clavicle fractures in adolescents. J Pediatr Orthop. 2010 Jun;30(4):307–312. doi: 10.1097/BPO.0b013e3181db3227. [DOI] [PubMed] [Google Scholar]
- 29.Altamimi S.A., McKee M.D., Canadian Orthopaedic Trauma Society Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. Surgical technique. J Bone Joint Surg Am. 2008 Mar;90(suppl 2 Pt 1):1–8. doi: 10.2106/JBJS.G.01336. [DOI] [PubMed] [Google Scholar]
- 30.Lodhi I.A., Russell R., Sharp D.J., Shah K.Y. The treatment of non-union of the clavicle with the AO mini external fixator. Surgeon. 2007;5(6):335–338. doi: 10.1016/s1479-666x(07)80085-0. [DOI] [PubMed] [Google Scholar]
- 31.Ledger M., Leeks N., Ackland T., Wang A. Short malunions of the clavicle: an anatomic and functional study. J Shoulder Elbow Surg. 2005;14:349–354. doi: 10.1016/j.jse.2004.09.011. [DOI] [PubMed] [Google Scholar]