

Abstract
Background:
This study aims to assess the frequency, causes, and places of injuries in a nationally representative sample of Iranian children and adolescents, as well as the referral, places allocated for injured individuals.
Methods:
This nationwide study was conducted in 2011-2012 among 13486 elementary, secondary and high-school students who were selected by random cluster stratified multistage sampling from 30 provinces in Iran. The Global School-based Health Survey questionnaire of the World Health Organization was used.
Results:
The study participants consisted of 50.8% boys, 75.6% urban resident with a mean age of 12.5 years. Overall, 20.25% of participants reported that they were minimally injured once in the last 12 months; this prevalence was higher in boys than in girls (25.74% vs. 14.58%, respectively, P < 0.001), without significant difference in urban (20.11%) and rural (20.69%) areas. Most of them (39.92%) were injured at homes or house yards with higher prevalence in girls than in boys (48.61% vs. 35.17%, respectively, P < 0.001) and in rural than in urban areas (27.30% vs. 20.89%, respectively, P < 0.001). Schools were reported as the second prevalent site of injury occurrence (22.50%). Emergency departments and physician offices were the most prevalent referral places for injured individuals (32.31% and 22.38%, respectively). Most of the school injuries occurred during play or sport activities (45.92%).
Conclusions:
Prevention of unintentional injuries should be considered as a health priority. Appropriate preventive strategies should be enhanced at homes and schools.
Keywords: Adolescents, children, injuries, Iran, prevention
INTRODUCTION
Injuries during childhood and adolescence are one of the major and detrimental problems, especially in developing countries.[1,2] Though different progressions are achieved in prevention and control of communicable disease and increasing the life expectancy, injuries are still assumed as one of the main factors of disability and morbidity.[3,4] Injuries could impose adverse mental and physical effects; albeit, these taints are affected with economic and cultural status of the family.[1,5] Children and adolescents are of the most vulnerable age groups in this regard.[6,7]
The prevalence of injuries is affected by different factors as the place of injury occurrence.[5] For instance, most of the injuries occur at homes and schools, they mainly comprise of falling, bone fractures, head trauma, burns, cuts, as well as vehicle accidents out of home and schools.[1,5,8,9,10,11,12,13] Different epidemiological studies have reported the prevalence of injuries in Iranian children; however, most of these studies comprised small sample size and have been conducted in restricted areas or reported hospital-based information. This study aims to assess the frequency, causes, and places of injury occurrence in a nationally representative sample of Iranian children and adolescents, as well as on places allocated for referring the injured individuals.
METHODS
This nationwide study was conducted in 2011-2012 as the fourth national survey of a school-based surveillance program entitled the childhood and adolescence surveillance and prevention of adult noncommunicable disease study. We have previously reported the methodology of this study,[14] and here we explain the methods related to the current paper.
Study population and sampling framework
The study population consisted of elementary, middle-, and high-school students from rural and urban areas of Iran. They were selected by multistage, cluster sampling method from 30 provinces of the country (48 cluster of 10 students in each province). Stratification was performed in each province according to location of residence (urban, rural), and school grade (elementary, middle- and high-school) proportional to the size and with equal sex ratio; that is, in each province, the number of boys and girls were the same and the ratios in urban and rural areas were proportionate to the population of students in each area. In this way, the number of samples in rural, urban areas and in each school grade was divided proportionally to the population of students in each grade.
Cluster sampling with equal clusters was used in each province to reach the sample size of interest. The clusters were determined at the level of schools, containing 10 samples in each cluster. The sample size was determined according to the cluster sampling method; the maximum sample size that could give a good estimate of all risk factors of interest was selected. Therefore, the sample size was calculated as 480 subjects in each province, therefore, 48 clusters of 10 subjects were selected in each province. Overall, 14880 students were selected by multistage sampling from 30 provinces in Iran.
The questionnaire of the World Health Organization - Global School-based Student Health Survey was used. It was translated to Persian, and we validated it as described before.[15]
Statistical analysis
Continuous variables are presented as mean (standard deviation) and categorical data as number (%). Categorical data were analyzed by Chi-square test. The sampling method (cluster sampling) was considered in all statistical analyses. Data were analyzed in the Stata Corp., 2011 (Stata Statistical Software: Release 12. College Station, TX: Stata Corp., LP. Package) by using survey (cluster) analysis design. P < 0.05 was considered as statistically significant.
RESULTS
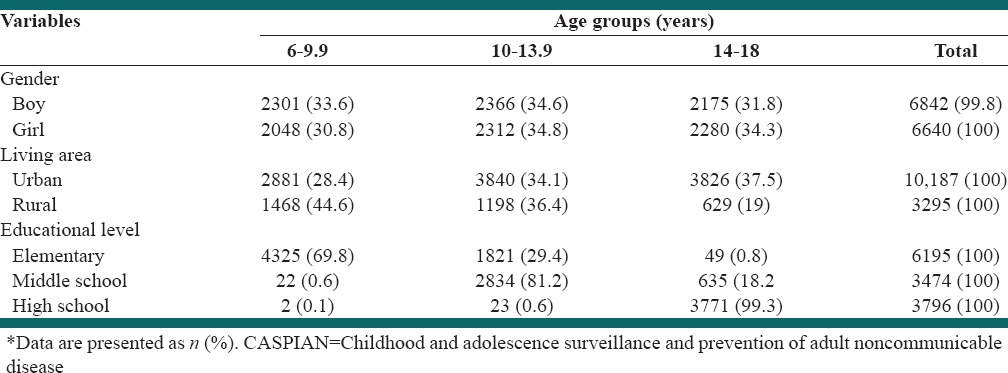
This survey comprised 13486 students (90.6% participation rate) consisting of 49.2% girls and 50.8% boys. The average age of participants was 12.47 ± 3.36 years, without significant difference in boys (12.36 ± 3.40 years) and girls (12.58 ± 3.32 years) respectively. Overall, 75.6% of students were from urban and 24.4% were from rural areas; 46% of students were from elementary schools, 25.9% from middle-school, and 28.1% from high-school. According to age categories 32.26%, 34.70%, and 33.04% were in the age groups of 6-10 years, 11-14 years, and 15-18 years, respectively. Table 1 shows the demographic characteristics of subjects by age groups.
Table 1.
Characteristics* of study participants according to gender, living area, and educational level: The CASPIAN-IV study
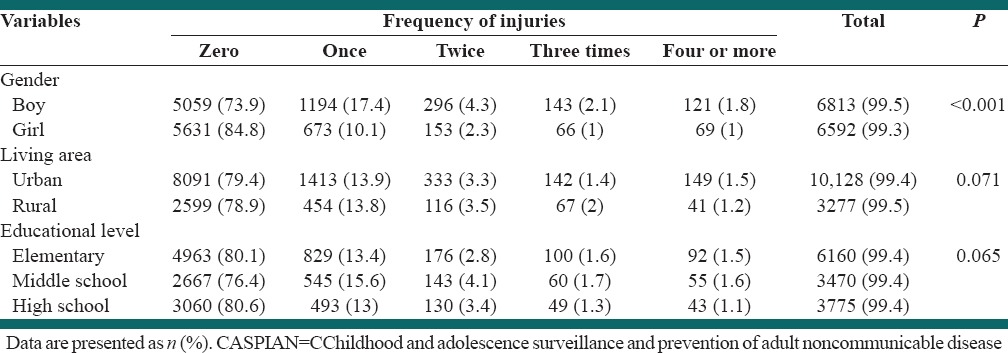
The frequency of one injury in the last 12 months was 13.93%, the prevalence of two, three, and at least four injuries were 3.35%, 1.56%, and 1%. 42% respectively; thus, 20.25% (n = 2645) of children and adolescents reported having been injured minimally once in the previous 12 months [Table 2]. This frequency was significantly higher in boys than in girls (25.74% vs. 14.58%, respectively, P < 0.001). This frequency was not significantly different in urban (20.11%) and rural areas (20.69%). The corresponding figures were 19.43%, 23.14% and 18.94% in elementary, middle, and high-school students respectively (P > 0.05).
Table 2.
Frequency of injuries during 12 months prior to the study according to gender, living area and educational level: The CASPIAN-IV study
Most of the children and adolescents (39.92%) were injured at their home or house yard; mean while this frequency was 22.50% in schools, and 17.09% in street [Table 3]. The frequency of injuries either in homes or schools was significantly higher in boys (35.17% and 22.12%) than in girls (48.61% and 23.18%), respectively, P < 0.001 [Table 3]. The frequency of injuries occurred in either homes or schools was higher in rural (40.87% and 27.30%) than in urban areas (39.61% and 20.89%) respectively, P < 0.001.
Table 3.
Place of injury occurrence during 12 months prior to the study according to gender, living area, and educational level: The CASPIAN-IV study
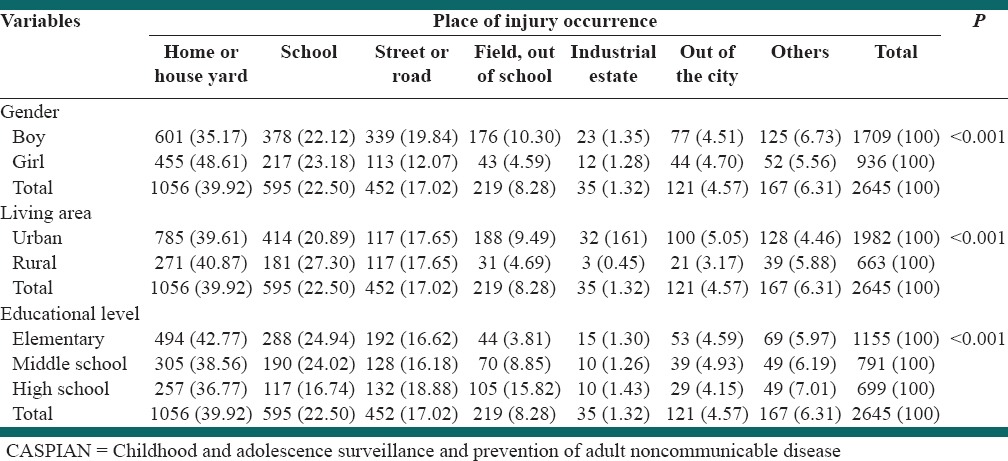
The frequency of injuries occurred at homes of students of elementary, secondary and high-schools was 42.77%, 38.56%, 36.77% respectively which was statistically significant (P < 0.001). Furthermore, the prevalence of injuries occurred at schools in elementary was significantly higher than secondary and high-schools (24.94%, 24.02% and, 16.74% respectively) (P < 0.001). Moreover, 18.88% of injured students in high-schools were injured in streets or routes in the previous 12 months.
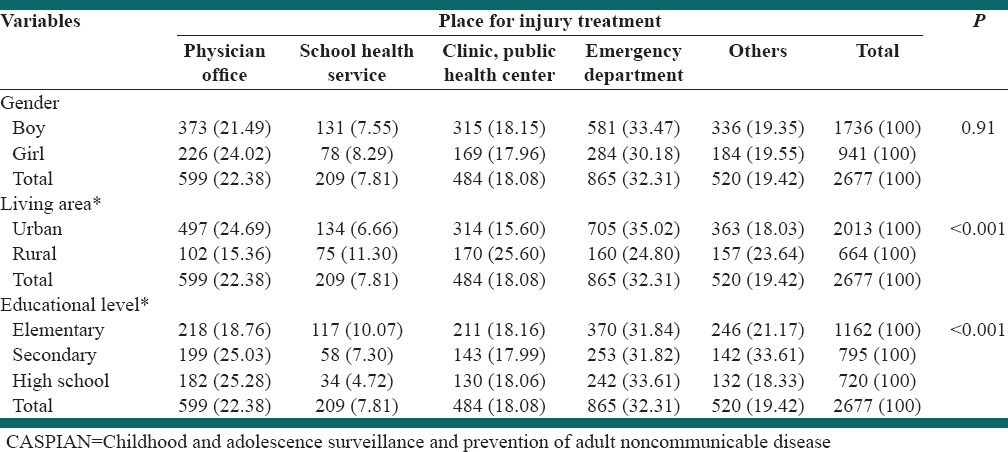
Table 4 shows the place for injuries treatment. As it shows 32.31% of the children and adolescents were referred to the emergency department, this frequency was not statistically different between boys and girls (33.47% vs. 30.18%, respectively, P > 0.05). In addition, the frequency of referrals to physician's office, clinics or public health centers, and school health services was 22.38%, 18.08%, and 7.81%, respectively. The frequency of referrals to the emergency department of hospitals was higher in urban than in rural areas (35.02% vs. 24.80%, respectively, P < 0.01), similarly, the frequency of referrals to clinics or public health centers was higher in urban than in rural areas (15.60% vs. 25.60%, respectively, P < 0.01).
Table 4.
Place of injury treatment during the 12 months prior to the study according to gender, living area and educational level: The CASPIAN-IV study
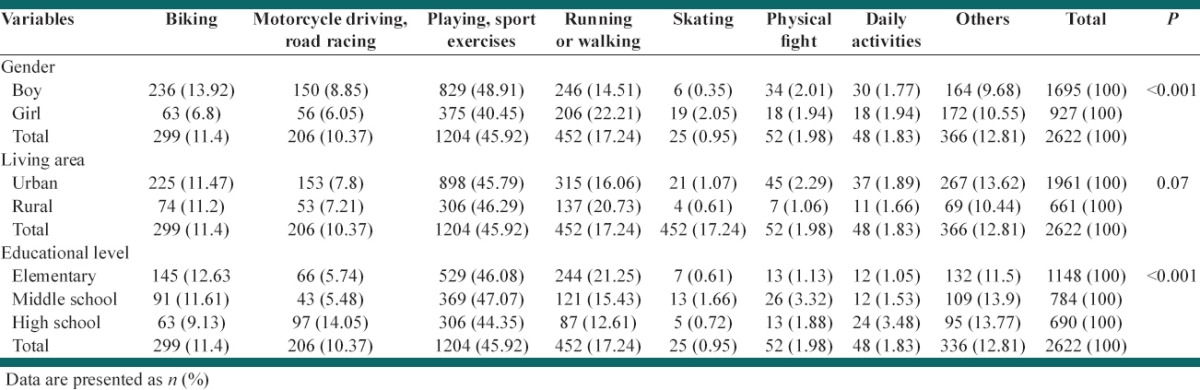
As shownin Table 5, 17.24% of participants reported that they have been injured while walking or running, 11.40% during biking, and 10.37% during motorcycle driving or road racing.
Table 5.
Frequency of activity pattern in time of injury during 12 months prior to the study according to gender, living area and educational level: The CASPIAN-IV study
DISCUSSION
The results of this nationwide study demonstrated that about 20% of Iranian children and adolescents were minimally injured during 12 months before the current study. In addition, the frequency of injuries was higher in boys than in girls, but it had no significant difference in rural and urban areas. These findings are in line with some previous national and international investigations.[5,13] Some previous studies have documented that the frequency of injuries is relatively high in Iranian children and adolescents, and usually boys are more injured than girls, similar to other studies.[5,8,13,16,17,18] This study showed that the most frequent places of injuries were homes, followed by schools. This finding is in line with some previous studies.[1,5,8,9,10,11,12,13,16,17,18] In the current study, the home injuries comprised falling, burning (directly or indirectly) and cut, whereas most of the school injuries occurred due to falling in playing fields. Therefore, more attention should be paid to the security issues of homes and schools to reduce injuries.
In the current study, most school injuries occurred during the physical exercises, this is consistent with some previous studies;[16,17,18,19,20] therefore, physical activity consideration should be emphasized for injury prevention, as recommended before.[21]
In the current study, the most prevalent places for treatment of injuries both in urban and rural areas were emergency departments and health centers respectively; this finding is consistent with some previous studies.[5,22]
Injuries are the leading cause of mortality in children and adolescents, and pose huge costs for the medical care and lost productivity. Injuries at home and school can be prevented. In the current study, most injuries had occurred at home; therefore, it is necessary to increase the knowledge of families about safety issues for preventing home and recreation-related injuries. It should be also ensured that all schools would have safe and healthy places for play and physical exercises of students.
Training children and adolescents about safety and necessary precautions for preventing injuries can be effective in reducing injuries.[23,24] It seems that implementing a comprehensive and appropriate strategy comprising appropriately sport activities for every age group, determination and controlling the possible risks of sport activities, increasing medical facilities in play and sport grounds are crucial for injury prevention.
Study limitations and strengths
The cross-sectional nature of the study and using self-reported data are the main limitations of the current study. However, its nationwide coverage, and using a valid international questionnaire are its main strengths.
CONCLUSIONS
Preventing unintentional injuries should be considered as a health priority for Iranian children and adolescents. The importance of safety at home and schools should be underscored.
ACKNOWLEDGMENTS
This study was conducted in cooperation with universities of medical sciences nationwide, we forward our sincere thanks to the large team working with this project, as well as the students, parents, and school staff.
Footnotes
Source of Support: This study was conducted as part of a national school-based surveillance program
Conflict of Interest: None declared.
REFERENCES
- 1.Peden M, Oyegbite K, Ozanne-Smith J, Hyder A, Branche C, Rahman F, et al. Geneva, Switzerland: World Health Organization and UNICEF; 2008. World Report on Child Injury Prevention. [PubMed] [Google Scholar]
- 2.Allender JA, Spradely BW. 3rd ed. Philadelphia: Lippincott; 2001. Community Health Nursing, Concept and Practice; p. 7. [Google Scholar]
- 3.Wong DL, Hockenberry M, Wilson D, Winkelstein M, Schwartz P. 7th ed. Ch 1, 7. St.Louis: Mosby; 2005. Nursing Care of Infant and Children; pp. 698–70. [Google Scholar]
- 4.Linnan M, Giersing M, Cox R, Linnan H, Williams M, Voumard C, et al. Florence, Italy: UNICEF Innocenti Research Centre; 2007. UNICEF Innocenti Working Papers: Child Mortality and Injury in Asia. [Google Scholar]
- 5.Khan UR, Bhatti JA, Zia N, Farooq U. School-based injury outcomes in children from a low-income setting: Results from the pilot injury surveillance in Rawalpindi city, Pakistan. BMC Res Notes. 2013;6:86. doi: 10.1186/1756-0500-6-86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Solis GR. Evaluation of a children's safety fair. Pediatr Nurs. 1991;17:255–8. [PubMed] [Google Scholar]
- 7.Nies MA, Mcewen M. 3rd ed. Philadelphia: W.B. Saunders Co; 2001. Community Health Nursing; p. 337. [Google Scholar]
- 8.Collins NC, Molcho M, Carney P, McEvoy L, Geoghegan L, Phillips JP, et al. Are boys and girls that different? An analysis of traumatic brain injury in children. Emerg Med J. 2013;30:675–8. doi: 10.1136/emermed-2011-200496. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Di Scala C, Gallagher SS, Schneps SE. Causes and outcomes of pediatric injuries occurring at school. J Sch Health. 1997;67:384–9. doi: 10.1111/j.1746-1561.1997.tb07182.x. [DOI] [PubMed] [Google Scholar]
- 10.Miller TR, Romano EO, Spicer RS. The cost of childhood unintentional injuries and the value of prevention. Future Child. 2000;10:137–63. [PubMed] [Google Scholar]
- 11.Yang CY, Yeh YC, Cheng MF, Lin MC. The incidence of school-related injuries among adolescents in Kaohsiung, Taiwan. Am J Prev Med. 1998;15:172–7. doi: 10.1016/s0749-3797(98)00046-4. [DOI] [PubMed] [Google Scholar]
- 12.Scheidt PC, Harel Y, Trumble AC, Jones DH, Overpeck MD, Bijur PE. The epidemiology of nonfatal injuries among US children and youth. Am J Public Health. 1995;85:932–8. doi: 10.2105/ajph.85.7.932. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bayat M, Shahsavari A, Forughi S, Mirzajani F, Alamneshan F. Prevalence of accidents in children under 5 years old referred to emergency ward. Mandish J. 2012;2:40–3. [Google Scholar]
- 14.Kelishadi R, Ardalan G, Qorbani M, Ataie-Jafari A, Bahreynian M, Taslimi M, et al. Methodology and early findings of the fourth survey of childhood and adolescence surveillance and prevention of adult non-communicable disease in Iran: The CASPIAN-IV Study. Int J Prev Med. 2013;4:1451–60. [PMC free article] [PubMed] [Google Scholar]
- 15.Kelishadi R, Majdzadeh R, Motlagh ME, Heshmat R, Aminaee T, Ardalan G, et al. Development and evaluation of a questionnaire for assessment of determinants of weight disorders among children and adolescents: The CASPIAN-IV study. Int J Prev Med. 2012;3:699–705. [PMC free article] [PubMed] [Google Scholar]
- 16.Laflamme L, Menckel E. School injuries in an occupational health perspective: What do we learn from community based epidemiological studies? Inj Prev. 1997;3:50–6. doi: 10.1136/ip.3.1.50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gratz RR. School injuries: What we know, what we need. J Pediatr Health Care. 1992;6:256–62. doi: 10.1016/0891-5245(92)90024-x. [DOI] [PubMed] [Google Scholar]
- 18.Fatmi Z, Kazi A, Hadden WC, Bhutta ZA, Razzak JA, Pappas G. Incidence and pattern of unintentional injuries and resulting disability among children under 5 years of age: Results of the National Health Survey of Pakistan. Paediatr Perinat Epidemiol. 2009;23:229–38. doi: 10.1111/j.1365-3016.2009.01024.x. [DOI] [PubMed] [Google Scholar]
- 19.Sosnowska S, Kostka T. Epidemiology of school accidents during a six school-year period in one region in Poland. Eur J Epidemiol. 2003;18:977–82. doi: 10.1023/a:1025802203726. [DOI] [PubMed] [Google Scholar]
- 20.Schalamon J, Eberl R, Ainoedhofer H, Singer G, Spitzer P, Mayr J, et al. School accidents in Austria. Pediatr Surg Int. 2007;23:861–5. doi: 10.1007/s00383-007-1951-5. [DOI] [PubMed] [Google Scholar]
- 21.Junkins EP, Jr, Knight S, Lightfoot AC, Cazier CF, Dean JM, Corneli HM. Epidemiology of school injuries in Utah: A population-based study. J Sch Health. 1999;69:409–12. doi: 10.1111/j.1746-1561.1999.tb06360.x. [DOI] [PubMed] [Google Scholar]
- 22.Sun YH, Yu IT, Wong TW, Zhang Y, Fan YP, Guo SQ. Unintentional injuries at school in China – patterns and risk factors. Accid Anal Prev. 2006;38:208–14. doi: 10.1016/j.aap.2005.09.010. [DOI] [PubMed] [Google Scholar]
- 23.Chapman RL, Buckley L, Sheehan M, Shochet IM. Pilot evaluation of an adolescent risk and injury prevention programme incorporating curriculum and school connectedness components. Health Educ Res. 2013;28:612–25. doi: 10.1093/her/cyt048. [DOI] [PubMed] [Google Scholar]
- 24.Lachapelle U, Noland RB, Von Hagen LA. Teaching children about bicycle safety: An evaluation of the New Jersey Bike School program. Accid Anal Prev. 2013;52:237–49. doi: 10.1016/j.aap.2012.09.015. [DOI] [PubMed] [Google Scholar]