

Abstract
Background
The health transition theory argues that societal changes produce proportional changes in causes of disability and death. The aim of this study was to identify long-term changes in main causes of hospitalization in working-age population within a nation that has experienced considerable societal change.
Methodology
National trends in all-cause hospitalization and hospitalizations for the five main diagnostic categories were investigated in the data obtained from the Finnish Hospital Discharge Register. The seven-cohort sample covered the period from 1976 to 2010 and consisted of 3,769,356 randomly selected Finnish residents, each cohort representing 25% sample of population aged 18 to 64 years.
Principal Findings
Over the period of 35 years, the risk of hospitalization for cardiovascular diseases and respiratory diseases decreased. Hospitalization for musculoskeletal diseases increased whereas mental and behavioral hospitalizations slightly decreased. The risk of cancer hospitalization decreased marginally in men, whereas in women an upward trend was observed.
Conclusions/Significance
A considerable health transition related to hospitalizations and a shift in the utilization of health care services of working-age men and women took place in Finland between 1976 and 2010.
Introduction
Change in population-wide disease patterns is a major public health issue. Knowledge of the disease trends and changing burden of disease is essential for estimating the impact of primary prevention, defining public health priorities, and predicting future health care needs [1]. Information on sex-specific patterns is important as different strategies may be needed for women and men. Previous studies examining sex-specific trends in hospitalization have typically focused on specific diseases or diagnostic categories, including diabetes [2], stroke [3], heart failure [4], [5], myocardial infarction [6]–[8], acute coronary syndromes [9], coronary heart disease [10], peripheral artery disease [11], asthma [12], chronic obstructive pulmonary disease [13], and carpal tunnel syndrome [14]. However, research on sex-specific national trends in all-cause hospitalization and hospitalization for main diagnostic categories is rare and information on long-term trends is lacking. In Germany, Nowossadeck [15] analyzed changing rates of hospitalization for individual diagnoses between 2000 and 2009 and found increased rates for congestive heart failure and diseases for spine and back; whereas the hospitalization rates for ischemic heart disease, cerebrovascular diseases and certain cancers decreased. The underlying trends were mainly similar for women and men. However, there were also notable differences; lung cancer hospitalizations decreased in men but sharply increased in women [15].
The individual research findings on shifts in the disease burden based on long follow-ups can be interpreted from the point of view of the health transition theory. This theory suggests that economic, social, cultural and political changes are likely to produce proportional changes in causes of disability and death [16], [17]. It is surprising that – to the best of our best knowledge – there are no previous studies on national hospitalization trends examining long-term proportional changes in disease burden across main diagnostic groups. The present study was set out to investigate the health transition and changing burden of disease in working-age population in Finland; a country which experienced dramatic societal change between the mid-1970s and 2010. In the working-age population the societal shift was reflected in changes in the occupational structure (from agricultural and industrial occupations to service and knowledge-sector occupations) and job content (from physically demanding and chemically hazardous jobs to mentally, socially and cognitively intensive tasks), overall growth of highly-skilled work force, the emergence of late modern work organisations based on the use of information technologies and mobile networks, and considerable changes in leisure time activities [18], [19]. As an indicator of severe health problems and the use of medical treatment we analysed the transition in all-cause hospitalizations and hospitalizations for the main diagnostic categories from 1976 to 2010 in seven representative cohorts of working-age men and women. Hospitalization was measured by the number of discharges rather than by the total number of inpatient days.
Materials and Methods
Study population
The total study period was divided into seven five-year time periods (1976–1980, 1981–1985, 1986–1990, 1991–1995, 1996–2000, 2001–2005, and 2006–2010). These seven independent cohorts were constructed by randomly selecting 25% of the 18 to 64-year-old Finns. In total, the study population included 3,769,356 working-age adults (52% men). Data on age and sex were obtained from a population database maintained by Statistics Finland in which every Finnish resident is registered. The dates of death, where applicable, were obtained from the National Death Register kept by Statistics Finland.
Hospitalization data
Hospitalization data were obtained from the Finnish Hospital Discharge Register that is maintained by the National Institute for Health and Welfare. The data consist of information on all cases of inpatient medical treatment in Finnish public sector hospitals. A recent systematic review showed that completeness and accuracy in this register varies from satisfactory to very good [20]. For each individual the diagnosis data were linked to Statistics Finland records by using national identification numbers. Outcomes were all-cause hospitalization and hospitalizations for the five main diagnostic categories: Diseases of the circulatory system (International Classification of Diseases, Eighth (ICD-8) and Ninth Revision (ICD-9) codes 390–459, International Classification of Diseases, Tenth Revision (ICD-10 codes I00–I99); Mental and behavioral disorders (ICD-8 and ICD-9 codes 291–319; ICD-10 codes F04–F99); Diseases of the musculoskeletal system and connective tissue (ICD-8 and ICD-9 codes 710–739; ICD-10 codes M00–M99); Diseases of the respiratory systems (ICD-8 and ICD-9 codes 460–519; ICD-10 codes J00–J99); and Neoplasms (ICD-8 and ICD-9 codes 140–208; ICD-10 codes C00–C97)). Since the vast majority of pregnancy-related hospitalizations relate to healthy deliveries and therefore do not indicate morbidity, we excluded pregnancy-related causes (ICD8-9 630–679 and ICD10 000–099) from the analyses.
The proportions of the hospitalizations for the five main categories of all first hospitalizations were as follows: musculoskeletal disorders 20%, cardiovascular diseases 15%, respiratory diseases 10%, mental and behavioral disorders 6%, and cancer 4%.
We followed-up the hospitalization data over a five year period in each of the seven cohorts. The follow-up began on 1st January at the beginning of each cohort and ended on the day the participant was hospitalized or died. For the rest of the participants, the follow-up period ended five years after it began, on 31st December.
All records/information was anonymized and de-identified prior to linkage and analysis. Ethical approval for the study was received from the Finnish Institute of Occupational Health.
Statistical analyses
Age-standardized incidence rates for all-cause and the five main diagnostic categories of hospitalization were calculated separately for men and women and are expressed as the annual number of cases per 10,000 persons in each five-year cohort. For every individual within each cohort, only the first hospitalization for the given diagnostic category was included and the individual was then removed from the risk population (as in the case of death). We did not exclude individuals' subsequent hospitalizations for other diagnostic categories. To detect time trends we applied Cox regression model, which produced age-adjusted sex-stratified proportional hazard ratios (HR) with 95% confidence intervals (95% CI) for all-cause hospitalization and hospitalization for the five main diagnostic categories for each five-year cohort between 1981 and 2010 in relation to the earliest cohort (1976–1980). Due to the random selection method the same individual could appear in several cohorts, but such cases could not be identified and in the analyses the cohorts were assumed to be independent.
All analyses were performed using the SAS 9.2 (SAS Institute, Cary, NC, USA) software.
Results
Altogether 1,453,190 hospitalizations in men and 1,918,936 hospitalizations in women were recorded in the study cohorts between 1976 and 2010. The mean follow-up time per cohort was 4.97 years.
Figure 1 presents the total number of hospitalizations by cohort in men and women and the mean age and the mean follow-up time in each cohort. Figures 2–7 present the age-standardized incidence rates per 10,000 individuals for all-cause hospitalization and the five main diagnostic categories in the seven cohorts. Compared to women, men had higher age-standardized rates of hospitalization for cardiovascular diseases and mental and behavioral disorders, whereas age-standardized incidence rates of musculoskeletal disorders and cancer were higher in women. Up until 2001–2005 men had considerably higher levels of hospitalization for respiratory diseases, but the gap has been narrowing and in 2006–2010 the difference was very small.
Figure 1. The total number of hospitalizations by cohort in men and women and the mean age and the mean follow-up time in each cohort, Finland 1976–2010.
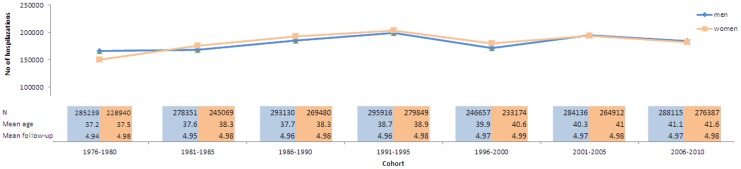
Figure 2. Age-standardized incidence rates per 10,000 individuals for all-cause hospitalizations in men and women, Finland 1976–2010.

Figure 7. Age-standardized incidence rates per 10,000 individuals for hospitalizations for cancers in men and women, Finland 1976–2010.

Figure 3. Age-standardized incidence rates per 10,000 individuals for hospitalizations for cardiovascular disease in men and women, Finland 1976–2010.

Figure 4. Age-standardized incidence rates per 10,000 individuals for hospitalizations for musculoskeletal disorders in men and women, Finland 1976–2010.

Figure 5. Age-standardized incidence rates per 10,000 individuals for hospitalizations for mental and behavioral disorders in men and women, Finland 1976–2010.

Figure 6. Age-standardized incidence rates per 10,000 individuals for hospitalizations for respiratory diseases in men and women, Finland 1976–2010.

In men, the age-standardized incidence rate decreased in all main causes of hospitalization apart from musculoskeletal disorders where it rose from 87 in 1976–1980 to 161 in 1996–2000 and remained stable until 2006–2010 (overall increase 85%). In women the age-standardized incidence rate of hospitalizations for musculoskeletal diagnoses increased from 112 in 1976–2010 to 174 in 2006–2010 (overall increase 55%). During the same period, the incidence rate of hospitalization for cardiovascular diseases decreased from 165 to 95 (overall decrease 42%) in men and from 165 to 66 (60%) in women. In a similar way, the incidence rate for respiratory diseases decreased, from 82 to 57 (30%) in men and from 66 to 51 (23%) in women. The incidence rate of hospitalizations for mental and behavioral disorders decreased from 45 to 30 (50%) in men and from 29 to 23 (21%) in women. In men the incidence rate for cancer-related hospitalizations decreased slightly from 31 to 28 (10%), whereas in women it increased from 29 to 44 in (52%). In men, cardiovascular diseases was the most common diagnostic category at the start of the study period, but was replaced by musculoskeletal disorders in 1996–2000. In women, musculoskeletal diagnoses overtook cardiovascular diagnoses as the largest diagnostic category already in 1986–1990.
Table 1 presents sex-stratified age-adjusted proportional risks of all-cause hospitalization and hospitalizations for the five main diagnostic categories among men and women in 1981–2010 using the first cohort (1976–1980) as the reference group. With the exception of cancer, the time trends were very similar in men and women. The risk of all-cause hospitalization remained relatively stable throughout the study period. The risk of hospitalization for cardiovascular diseases decreased systematically throughout the study period (HR 0.57; 95% CI: 0.56, 0.58 in 2006–2010 in men and HR 0.39; 95% CI: 0.38, 0.40 in 2006–2010 in women). The risk of hospitalization for musculoskeletal disorders increased, but the increase levelled off already in 1996–2000 (HR 1.83; 95% CI: 1.79, 1.88 in 2006–2010 in men and HR 1.52; 95% CI: 1.48, 1.55 in 2006–2010 women). The risk of hospitalization for mental and behavioral disorders decreased slightly (HR 0.63; 95% CI: 0.61, 0.66 in 2006–2010 in men and HR 0.81; 95% CI: 0.78, 0.85 in 2006–2010 in women).
Table 1. Age-adjusted Proportional Hazard Ratios (HR) and their 95% Confidence Intervals for Hospitalization in Relation to the First Cohort in Seven Consecutive Cohorts, Finland, 1976–2010.
| Men | Women | |||||
| All-cause | N/Cases | HR | 95% CI | N/Cases | HR | 95% CI |
| 1976–1980 | 285,239/81,164 | 1.00 | reference | 228,940/80,894 | 1.00 | reference |
| 1981–1985 | 278,351/80,108 | 1.03 | 1.02, 1.04 | 245,069/89,577 | 1.04 | 1.03, 1.05 |
| 1986–1990 | 293,130/86,562 | 1.06 | 1.05, 1.07 | 269,480/98,681 | 1.05 | 1.04, 1.06 |
| 1991–1995 | 295,916/88,868 | 1.05 | 1.04, 1.04 | 279,849/101,007 | 1.00 | 0.99, 1.01 |
| 1996–2000 | 246,657/79,058 | 1.13 | 1.12, 1.14 | 233,174/88,648 | 1.04 | 1.03, 1.05 |
| 2001–2005 | 284,136/90,563 | 1.10 | 1.09, 1.11 | 264,912/93,473 | 0.94 | 0.93, 0.95 |
| 2006–2010 | 288,115/88,795 | 1.02 | 1.01, 1.03 | 276,387/91,591 | 0.87 | 0.86, 0.88 |
| Cases | HR | 95% CI | Cases | HR | 95% CI | |
| Cardiovascular diseases | ||||||
| 1976–1980 | 16,670 | 1.00 | reference | 15,500 | 1.00 | reference |
| 1981–1985 | 15,024 | 0.92 | 0.90, 0.94 | 14,505 | 0.85 | 0.83, 0.87 |
| 1986–1990 | 15,298 | 0.89 | 0.87, 0.91 | 14,256 | 0.76 | 0.74, 0.77 |
| 1991–1995 | 14,836 | 0.79 | 0.78, 0.81 | 14,194 | 0.70 | 0.68, 0.71 |
| 1996–2000 | 11,990 | 0.73 | 0.71, 0.74 | 11,903 | 0.66 | 0.64, 0.67 |
| 2001–2005 | 13,124 | 0.67 | 0.65, 0.74 | 10,775 | 0.52 | 0.50, 0.53 |
| 2006–2010 | 12,441 | 0.57 | 0.56, 0.58 | 8797 | 0.39 | 0.38, 0.40 |
| Musculoskeletal disorders | ||||||
| 1976–1980 | 10,900 | 1.00 | reference | 10,965 | 1.00 | reference |
| 1981–1985 | 13,097 | 1.23 | 1.20, 1.26 | 14,230 | 1.20 | 1.17, 1.23 |
| 1986–1990 | 15,566 | 1.39 | 1.36, 1.42 | 16,631 | 1.28 | 1.25, 1.31 |
| 1991–1995 | 17,975 | 1.54 | 1.50, 1.57 | 18,470 | 1.31 | 1.28, 1.34 |
| 1996–2000 | 18,524 | 1.86 | 1.81, 1.90 | 19,416 | 1.57 | 1.53, 1.61 |
| 2001–2005 | 20,987 | 1.82 | 1.78, 1.86 | 20,953 | 1.48 | 1.45, 1.51 |
| 2006–2010 | 21,744 | 1.83 | 1.79, 1.88 | 22,673 | 1.52 | 1.48, 1.55 |
| Mental and behavioral disorders | ||||||
| 1976–1980 | 6624 | 1.00 | reference | 3291 | 1.00 | reference |
| 1981–1985 | 5392 | 0.83 | 0.80, 0.86 | 3132 | 0.89 | 0.84, 0.93 |
| 1986–1990 | 5873 | 0.86 | 0.83, 0.89 | 3387 | 0.87 | 0.83, 0.91 |
| 1991–1995 | 6574 | 0.95 | 0.92, 0.98 | 3938 | 0.96 | 0.92, 1.01 |
| 1996–2000 | 4334 | 0.74 | 0.72, 0.95 | 2970 | 0.86 | 0.82, 0.91 |
| 2001–2005 | 4877 | 0.73 | 0.70, 0.76 | 3489 | 0.90 | 0.86, 0.94 |
| 2006–2010 | 4226 | 0.63 | 0.61, 0.66 | 3229 | 0.81 | 0.78, 0.85 |
| Respiratory diseases | ||||||
| 1976–1980 | 11,326 | 1.00 | reference | 7449 | 1.00 | reference |
| 1981–1985 | 11,122 | 1.07 | 1.04, 1.09 | 7603 | 0.91 | 0.89, 0.94 |
| 1986–1990 | 11,343 | 1.04 | 1.01, 1.07 | 7611 | 0.96 | 0.93, 0.99 |
| 1991–1995 | 10,349 | 0.95 | 0.92, 0.97 | 8009 | 0.87 | 0.84, 0.90 |
| 1996–2000 | 8557 | 0.98 | 0.95, 1.01 | 6835 | 0.91 | 0.88, 0.94 |
| 2001–2005 | 9835 | 0.93 | 0.91, 0.96 | 7220 | 0.84 | 0.81, 0.87 |
| 2006–2010 | 7991 | 0.73 | 0.71, 0.75 | 6893 | 0.76 | 0.74, 0.79 |
| Cancers | ||||||
| 1976–1980 | 3002 | 1.00 | reference | 2589 | 1.00 | reference |
| 1981–1985 | 2726 | 0.94 | 0.89, 0.99 | 3088 | 1.08 | 1.03, 1.14 |
| 1986–1990 | 2736 | 0.91 | 0.87, 0.96 | 3715 | 1.21 | 1.15, 1.27 |
| 1991–1995 | 2777 | 0.85 | 0.81, 0.89 | 4290 | 1.26 | 1.20, 1.33 |
| 1996–2000 | 2471 | 0.87 | 0.83, 0.92 | 4439 | 1.45 | 1.38, 1.52 |
| 2001–2005 | 3361 | 0.97 | 0.92, 1.02 | 5421 | 1.52 | 1.45, 1.59 |
| 2006–2010 | 3666 | 0.90 | 0.66, 0.95 | 5987 | 1.51 | 1.45, 1.59 |
The risk of hospitalization for respiratory diseases has declined both in men and women. The risk of cancer hospitalization has decreased very slightly in men, whereas in women a constant upward trend in the risk can be observed (HR 1.51; 95% CI: 1.45, 1.59 in 2006–2010).
Discussion
The present study examined incidence rates and proportional risks for all-cause hospitalization and for the five main diagnostic categories in seven representative consecutive cohorts of Finnish working-age men and women between 1976 and 2010. The findings show that musculoskeletal disorders have increased their proportion of the total of all five diagnostic categories that were included in this study whilst the proportion of cardiovascular diseases has decreased. The observed overall trends were very similar in men and women with the exception of cancer: these hospitalizations marginally decreased in men but increased in women. The findings provide new evidence which specifies the health transition theory. It seems that the general transition occurs in hospitalizations when the nation moves towards the late modern societal order but the pattern of the changes is partly different for women and men. The general secular shifts and sex-specific findings are probably related to notable changes in lifestyles and in living and working conditions but at the same time they also are likely to be connected to developments in health care, health promotion, and health policies.
Cardiovascular disease
Our findings demonstrate a declining incidence of hospitalization for cardiovascular diseases; the decrease being a slightly larger in women. Studies from other national samples show that age-adjusted coronary heart disease and cerebrovascular disease hospitalization rates have significantly decreased [21]. The role of widespread primary prevention and decreases in conventional risk factors have been highlighted as important contributors to these reductions; including decreases in smoking prevalence and population wide levels of systolic blood pressure as well as favorable lipid effects [22], [23]. The widespread and increasing use of antihypertensive drugs as well as statins and other lipid-lowering drugs, has probably also contributed to these trends [24], [25]. However, it has been predicted that increasing prevalence of overweight and obesity may be compromising favorable trends in the risk factors in the future [23].
Moreover, it is well known that trends in cardiovascular diseases may be set decades before the conditions become manifest [26], and that early-life poor socio-economic conditions are associated with a higher cardiovascular risk later in life [27]; an important part of this is their potential effect on development of conventional risk factors [28]. It is therefore plausible that population-wide improvements in childhood socio-economic environments have contributed to declining cardiovascular risk. In addition, decreases in cardiovascular risk factors relate to an upward shift in educational attainment; a substantially smaller proportion of the population than before is exposed to the risk associated with low education [28]. The contribution of educational shift has been shown to be somewhat stronger for women than for men. In addition, changes in policies, such as introduction of comprehensive smoke-free policy, may have helped to change social norms [29].
Musculoskeletal disorders
Our results show a clear increase in hospitalizations for musculoskeletal disorders. Indeed, musculoskeletal disorders have become the most common reason for claiming sickness allowance in Finland [30]. Hospitalization due to musculoskeletal disorders has also increased in Germany [15]. In the US health care utilisation for spine conditions, the prevalence of chronic impairing low back pain, and back and neck-related health expenditure have increased [31], [32]. In Finland it has been noted that there have been improvements in diagnostic and therapeutic methods that reveal an increasing range of musculoskeletal disorders [33].
Increasing rates of musculoskeletal hospitalization may be attributable to changes in the nature of working life: the shift from manual types of jobs towards jobs involving more sedentary tasks such as more office-based and computer-based jobs. It is now acknowledged that for a large number of employees, lack of physical activity – both at work and on leisure time - is a major risk factor for musculoskeletal ill health [34]. At the same time, obesity, which is a risk factor for particularly certain musculoskeletal conditions [35], has rapidly increased.
Work-related psychosocial stress has also been linked to hospitalizations for musculoskeletal disorders [36]. Because of the globalisation of work, widespread information technology and a growing pressure to increase productivity and more stressful psychosocial environments and working patterns are now affecting increasing proportions of both the male and female workforce [37].
Mental and behavioral disorders
The risk of psychiatric hospitalization decreased slightly. Mental disorders as a reason for sickness absence and disability pension have increased in recent decades in Finland [33]. As in most high income countries, mental health service in Finland has been dramatically transformed by an increase in ambulatory treatment and care. However, despite decrease in the total number of hospital beds, the annual number of psychiatric in-patients has remained largely unchanged over time; this is due to the decrease in average length of psychiatric hospital stay [38].
Respiratory diseases
Our data show that the risk of hospitalization for respiratory diseases has decreased. In a similar way, in Danish working population, the number of hospitalizations for chronic lower respiratory diseases has been reduced over time [39].
The decrease in hospitalizations both for cardiovascular and respiratory diseases can be partially explained by widespread smoke-free legislation, introduced in Finland from 1990s onwards. A recent meta-analysis showed that smoke-free legislation is associated for a lower risk of hospitalization for cardiac, cerebrovascular and respiratory diseases [40].
In addition, considerable regulatory measures have been taken to prevent the adverse health outcomes of hazardous substances, for example all asbestos usage has been banned and lead-exposed workers are being biologically monitored [41]. Occupational inhalation exposure to most chemical agents has decreased in Finland since 1970s and chemical exposures and related disease burden are expected to further decrease in the future [42].
Cancer
Our results showed that the risk of cancer hospitalization decreased marginally in men, whereas in women an upward trend in risk can be observed. An earlier study in the Finnish general population similarly showed that in men there have been only minor changes in the age-standardized total cancer incidence rates, whereas in women the total cancer morbidity has slightly increased since the 1950s [43].
A number of reasons may have contributed to increasing cancer rates in working-age women. First, the risk of breast cancer has continuously increased. The introduction of organised mammographic screening programme affects the breast cancer incidence rate in a population as the diagnosis is advanced in time [44]. In Finland national mammographic screening was introduced in 1987; in that year the incidence of breast cancer increased by about one-tenth [45]. An analysis of secular trends which corrected for the influence of screening showed that in Finland the breast cancer rates increased by 13% per 5-year period [44]. Another important contributing factor for the increased breast cancer risk relates to the increased use of postmenopausal hormone therapy (HT) [45]. A study examining the HT use and breast cancer risk in Nordic countries in 1995 showed that in three other Nordic countries (Sweden, Norway and Iceland) that had had a significant drop in HT use, the increasing trends of breast cancer incidences either experienced a down-turn or the increase declined whereas in Finland, with only a small decline in HT, this was less evident [46].
Second, strong and consistent increases in endometrial cancer have been reported over the last 50 years; the biggest increase has been seen in postmenopausal women but in the last decade the rates have also increased in younger women [47].
Third, in Finland smoking has systematically decreased in men already over several decades whereas in women smoking has started to decline only in recent years. As a consequence, the incidence of lung cancer has constantly increased in women and is projected to continue to increase [45].
Finally, obesity has strongly increased over the last three decades and it is well established that excess body adiposity is a risk factor for cancer development [48]. It has also been shown that both in relative and absolute terms, obesity–related cancer is a greater problem for women than men; and endometrial, breast and colorectal cancers have been identified as priorities for research and public health measures [48].
Strengths and limitations
A major strength of our study was that the hospitalization data were derived from a national hospital discharge register with proven good accuracy and coverage [20]. There was no loss to follow-up and the changes in International Classification of Diseases were recoded to correspond to the most recent classification. As far as we are aware, this was the first study to examine long-term national trends in main causes of hospitalization among working-age men and women.
Despite these strengths, it is also important to acknowledge potential limitations. First, we used hospitalization as a proxy for underlying morbidity. Hospitalization is considered to be a reliable indicator of the use of medical treatment [49]. However, the long-term shifts in the use of hospital services and proportional share of diagnoses related to hospitalizations within a population are also likely to reflect changes in treatments and options of health care. Moreover, over time changes in coding practices and diagnostic criteria may have affected hospitalization trends for some causes and proportional shares of main diagnostic categories.
Second, referral bias and differential access to hospital services might have affected the results [50]. Self-referral and referral by general practitioners may be influenced by a number of factors such as geography, employment status, age, education, and economic status [50]. There are significant differences in health care service provision between local authorities and significant socioeconomic and regional inequities in the provision of and access to health care services in Finland [33], [51].
Third, we considered only the first hospitalization for any of the five diagnostic categories and excluded any subsequent hospitalizations for the same category.
Conclusions
The present study demonstrates that there have been significant secular shifts in main causes of hospitalization and consequently the content of disease burden requiring hospital treatment has considerably changed among the Finnish working-age population between 1976 and 2010. This study provides new evidence of the health transition in a nation that has moved towards the late modern spheres of life within a short period of time. Generally the main trend both in men and women was away from cardiovascular and respiratory diseases and towards musculoskeletal disorders. Interestingly, cancer treatments in hospitals decreased marginally in men but clearly increased in women. The exact reasons for the observed trends are not known. However, it is likely that two types of factors – health interventions and socio-economic and lifestyle changes - have affected these trends. Health interventions include better control of many cardiovascular risk factors and advances in medical treatments. Socio-economic and lifestyle changes beyond the health sector include changes in working life and in the occupational distribution of the labor force, higher educational levels, increased social mobility, increased use of digital technology, more sedentary work and lifestyles, and increasing obesity rates. The present findings can have significant policy implications. Awareness of sex-specific long-term temporal changes in main causes of hospitalizations can help to identify public health priorities and guide health care planning.
Data Availability
The authors confirm that, for approved reasons, some access restrictions apply to the data underlying the findings. Our study utilizes administrative record linkage and all data used in the present manuscript were obtained from third parties. Interested researchers need to obtain these data directly from them. Data on age and sex were obtained from the population database maintained by Statistics Finland and the dates of death were obtained from the National Death Register also kept by Statistics Finland. Hospitalization data were obtained from the Finnish Hospital Discharge Register that is maintained by the National Institute for Health and Welfare in Finland. Record linkage was conducted by Statistics Finland. Contact details for organizations that own the data: Data on hospitalizations: National Institute for Welfare and Health Arto Vuori, Development Manager THL Information Department arto.vuori@thl.fi tel. +358 29 524 7035. Other register data used in this study: Statistics Finland Registrar's Office Sanna Malinen, Statistician kirjaamo@stat.fi tel. +358 29 551 2564.
Funding Statement
This work was supported by the Academy of Finland (grant 67172). A. Kouvonen was supported by the Medical Research Council (MRC) (grant MR/K023241/1) and the Economic and Social Research Council (ESRC) (grant ES/L007509/1). R. De Vogli was supported by the Economic and Social Research Council (ESRC) (grant RES-070-27-0034). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1. Hoeymans N, Wong A, van Gool CH, Deeg DJH, Nusselder WJ, et al. (2012) The disabling effect of diseases: a study on trends in diseases, activity limitations, and their interrelationships. Am J Public Health 102: 163–170 10.2105/AJPH.2011.300296 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Lee JM, Davis MM, Gebremariam A, Kim C (2010) Age and sex differences in hospitalizations associated with diabetes. J Womens Heal 19: 2033–2042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Lewsey JD, Jhund PS, Gillies M, Chalmers JWT, Redpath A, et al. (2009) Age- and sex-specific trends in fatal incidence and hospitalized incidence of stroke in Scotland, 1986 to 2005. Circ Cardiovasc Qual Outcomes 2: 475–483 10.1161/CIRCOUTCOMES.108.825968 [DOI] [PubMed] [Google Scholar]
- 4.Haldeman GA, Croft JB, Giles WH, Rashidee A, Atlanta MS (1999) Congestive Heart Failure Hospitalization of patients with heart failure: National Hospital Discharge Survey, 1985 to 1995. [DOI] [PubMed]
- 5. Schaufelberger M, Swedberga K, Koster M, Rosen M, Rosengren A (2004) Decreasing one-year mortality and hospitalization rates for heart failure in Sweden: Data from the Swedish Hospital Discharge Registry 1988 to 2000. Eur Heart J 25: 300–307. [DOI] [PubMed] [Google Scholar]
- 6. Towfighi A, Markovic D, Ovbiagele B (2011) National gender-specific trends in myocardial infarction hospitalization rates among patients aged 35 to 64 years. Am J Cardiol 108: 1102–1107 10.1016/j.amjcard.2011.05.046 [DOI] [PubMed] [Google Scholar]
- 7. Wang OJ, Wang Y, Chen J, Krumholz HM (2012) Recent trends in hospitalization for acute myocardial infarction. Am J Cardiol 109: 1589–1593 10.1016/j.amjcard.2012.01.381 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Schmidt M, Bonde J, Lash TL, Bøtker HE, Sørensen HT (2012) 25 year trends in first time hospitalisation for acute myocardial infarction, subsequent short and long term mortality, and the prognostic impact of sex and comorbidity: a Danish nationwide cohort study. BMJ 356: 1–12 10.1136/bmj.e356 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Nedkoff LJ, Briffa TG, Preen DB, Sanfilippo FM, Hung J, et al. (2011) Age- and sex-specific trends in the incidence of hospitalized acute coronary syndromes in Western Australia. Circ Cardiovasc Qual Outcomes 4: 557–564 10.1161/CIRCOUTCOMES.110.960005 [DOI] [PubMed] [Google Scholar]
- 10. Briffa T, Nedkoff L, Peeters A, Tonkin A, Hung J, et al. (2011) Discordant age and sex-specific trends in the incidence of a first coronary heart disease event in Western Australia from 1996 to 2007. Heart 97: 400–404 10.1136/hrt.2010.210138 [DOI] [PubMed] [Google Scholar]
- 11. Inglis SC, Lewsey JD, Chandler D, Byrne DS, Lowe GDO, et al. (2012) Sex-specific time trends in first admission to hospital for peripheral artery disease in Scotland 1991–2007. Br J Surg 99: 680–687 10.1002/bjs.8686 [DOI] [PubMed] [Google Scholar]
- 12. Getahun D, Demissie K, Rhoads G (2005) Recent trends in asthma hospitalization and mortality in the United States. J Asthma 42: 373–378. [DOI] [PubMed] [Google Scholar]
- 13. Lykkegaard J, Søndergaard J, Kragstrup J, Rømhild Davidsen J, Knudsen T, et al. (2012) All Danish first-time COPD hospitalisations 2002–2008: incidence, outcome, patients, and care. Respir Med 106: 549–556 10.1016/j.rmed.2011.11.001 [DOI] [PubMed] [Google Scholar]
- 14. Mattioli S, Baldasseroni A, Curti S, Cooke RMT, Bena A, et al. (2008) Incidence rates of in-hospital carpal tunnel syndrome in the general population and possible associations with marital status. BMC Public Health 8: 374 10.1186/1471-2458-8-374 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Nowossadeck E (2012) Population aging and hospitalization for chronic disease in Germany. Dtsch Arztebl Int 109: 151–157 10.3238/arztebl.2012.0151 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Frenk J, Bobadilla J, Stern C, Frejka T, Lozano R (1991) Elements for a theory of the health transition. Heal Transit Rev 1: 21–38. [PubMed] [Google Scholar]
- 17.Mesle F, Vallin J (2006) The health transition: trends and prospects. In: Caselli G, Vallin J, Wunsch G, editors. Demography, Analysis and Synthesis. A Treatise in Demography. New York: Elsevier. pp.247–602. [Google Scholar]
- 18.Hjerppe R, Jalava J (2006) Economic Growth and Structural Change: A Century and a Half of Catching-up. In: Ojala J, Eloranta J, Jalava J, editors. The Road to Prosperity: an Economic History of Finland. Helsinki: Suomalaisen Kirjallisuuden Seura. [Google Scholar]
- 19.Lehto A-M, Sutela H (2008) Työolojen kolme vuosikymmentä. Työolotutkimusten tuloksia 1977–2008 [Three decades of working conditions. Results from the Working Conditions Survey 1977–2008]. Helsinki: Tilastokeskus [Statistics Finland].
- 20. Sund R (2012) Quality of the Finnish Hospital Discharge Register: a systematic review. Scand J Public Health 40: 505–515 10.1177/1403494812456637 [DOI] [PubMed] [Google Scholar]
- 21. Liu L (2011) Changes in cardiovascular hospitalization and comorbidity of heart failure in the United States: findings from the National Hospital Discharge Surveys 1980–2006. Int J Cardiol 149: 39–45 10.1016/j.ijcard.2009.11.037 [DOI] [PubMed] [Google Scholar]
- 22. Luepker R V (2008) Decline in incident coronary heart disease: why are the rates falling? Circulation 117: 592–593 10.1161/CIRCULATIONAHA.107.747477 [DOI] [PubMed] [Google Scholar]
- 23. Ford ES, Ajani UA, Croft JB, Critchley JA, Labarthe DR, et al. (2007) Explaining the decrease in U.S. deaths from coronary disease, 1980–2000. N Engl J Med 356: 2388–2398 10.1056/NEJMsa053935 [DOI] [PubMed] [Google Scholar]
- 24. Danaei G, Finucane MM, Lin JK, Singh GM, Paciorek CJ, et al. (2011) National, regional, and global trends in systolic blood pressure since 1980: systematic analysis of health examination surveys and epidemiological studies with 786 country-years and 5·4 million participants. Lancet 377: 568–577 10.1016/S0140-6736(10)62036-3 [DOI] [PubMed] [Google Scholar]
- 25. Farzadfar F, Finucane MM, Danaei G, Pelizzari PM, Cowan MJ, et al. (2011) National, regional, and global trends in serum total cholesterol since 1980: systematic analysis of health examination surveys and epidemiological studies with 321 country-years and 3·0 million participants. Lancet 377: 578–586 10.1016/S0140-6736(10)62038-7 [DOI] [PubMed] [Google Scholar]
- 26. Ulmer H, Kelleher CC, Fitz-Simon N, Diem G, Concin H (2007) Secular trends in cardiovascular risk factors: an age-period cohort analysis of 698,954 health examinations in 181,350 Austrian men and women. J Intern Med 261: 566–576 10.1111/j.1365-2796.2007.01779.x [DOI] [PubMed] [Google Scholar]
- 27. Galobardes B, Smith GD, Lynch JW (2006) Systematic review of the influence of childhood socioeconomic circumstances on risk for cardiovascular disease in adulthood. Ann Epidemiol 16: 91–104 10.1016/j.annepidem.2005.06.053 [DOI] [PubMed] [Google Scholar]
- 28. Harper S, Lynch J, Smith GD (2011) Social determinants and the decline of cardiovascular diseases: understanding the links. Annu Rev Public Health 32: 39–69 10.1146/annurev-publhealth-031210-101234 [DOI] [PubMed] [Google Scholar]
- 29. Thrasher JF, Boado M, Sebrié EM, Bianco E (2009) Smoke-free policies and the social acceptability of smoking in Uruguay and Mexico: findings from the International Tobacco Control Policy Evaluation Project. Nicotine Tob Res 11: 591–599 10.1093/ntr/ntp039 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kela [Social Insurance Institution] (2012) Statistical Yearbook of the Social Insurance Institution. Helsinki.
- 31. Freburger JK, Holmes GM, Agans RP, Jackman AM, Darter JD, et al. (2009) The rising prevalence of chronic low back pain. Arch Intern Med 169: 251–258 10.1001/archinternmed.2008.543 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Martin BI, Deyo RA, Mirza SK, Turner JA, Comstock BA, et al. (2008) Expenditures and health status among adults with back and neck problems. JAMA 299: 656–664 10.1001/jama.299.6.656 [DOI] [PubMed] [Google Scholar]
- 33. Vuorenkoski L (2008) Finland: Health System Review. European Observatory on Health Systems and Policies [Google Scholar]
- 34. Straker L, Mathiassen SE (2009) Increased physical work loads in modern work–a necessity for better health and performance? Ergonomics 52: 1215–1225 10.1080/00140130903039101 [DOI] [PubMed] [Google Scholar]
- 35. Wearing SC, Hennig EM, Byrne NM, Steele JR, Hills AP (2006) Musculoskeletal disorders associated with obesity: a biomechanical perspective. Obes Rev 7: 239–250 10.1111/j.1467-789X.2006.00251.x [DOI] [PubMed] [Google Scholar]
- 36. Lincoln AE, Smith GS, Amoroso PJ, Bell NS (2002) The natural history and risk factors of musculoskeletal conditions resulting in disability among US Army personnel. Work 18: 99–113. [PMC free article] [PubMed] [Google Scholar]
- 37.Schnall PL, Dobson M, Rosskam E, editors (2009) Unhealthy Work: Causes, Consequences, Cures. New York: Baywood Publishing.
- 38. Wahlbeck K, Westman J, Nordentoft M, Gissler M, Laursen TM (2011) Outcomes of Nordic mental health systems: life expectancy of patients with mental disorders. Br J Psychiatry 199: 453–458 10.1192/bjp.bp.110.085100 [DOI] [PubMed] [Google Scholar]
- 39. Tüchsen F, Hannerz H, Mølgaard EF, Brauer C, Kirkeskov L (2012) Time trend in hospitalised chronic lower respiratory diseases among Danish building and construction workers, 1981–2009: a cohort study. BMJ Open 2: 1–6 10.1136/bmjopen-2012-001761 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Tan CE, Glantz SA (2012) Association between smoke-free legislation and hospitalizations for cardiac, cerebrovascular, and respiratory diseases: a meta-analysis. Circulation 126: 2177–2183 10.1161/CIRCULATIONAHA.112.121301 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Nurminen M, Karjalainen A (2001) Epidemiologic estimate of the proportion of fatalities related to occupational factors in Finland. Scand J Work Environ Health 27: 161–213 10.5271/sjweh.605 [DOI] [PubMed] [Google Scholar]
- 42. Kauppinen T, Uuksulainen S, Saalo A, Mäkinen I (2013) Trends of Occupational Exposure to Chemical Agents in Finland in 1950–2020. Ann Occup Hyg 57: 593–609 10.1093/annhyg/mes090 [DOI] [PubMed] [Google Scholar]
- 43.Teppo L, Pukkala E, Sankila R (1999) Cancers. In: Koskinen S, Aromaa A, Huttunen J, Teperi J, editors. Health in Finland. Helsinki: National Public Health Institute KTL; National Research and Development Centre for Welfare and Health STAKES; Ministry of Social Affairs and Health. [Google Scholar]
- 44. Møller B, Weedon-Fekjaer H, Hakulinen T, Tryggvadóttir L, Storm HH, et al. (2005) The influence of mammographic screening on national trends in breast cancer incidence. Eur J Cancer Prev 14: 117–128. [DOI] [PubMed] [Google Scholar]
- 45.Pukkala E, Sankila R, Rautalahti M (2013) Cancer in Finland. Helsinki: Cancer Society of Finland.
- 46. Hemminki E, Kyyrönen P, Pukkala E (2008) Postmenopausal hormone drugs and breast and colon cancer: Nordic countries 1995–2005. Maturitas 61: 299–304 10.1016/j.maturitas.2008.09.022 [DOI] [PubMed] [Google Scholar]
- 47. Lindemann K, Eskild A, Vatten LJ, Bray F (2010) Endometrial cancer incidence trends in Norway during 1953–2007 and predictions for 2008–2027. Int J Cancer 127: 2661–2668 10.1002/ijc.25267 [DOI] [PubMed] [Google Scholar]
- 48. Renehan AG, Soerjomataram I, Tyson M, Egger M, Zwahlen M, et al. (2010) Incident cancer burden attributable to excess body mass index in 30 European countries. Int J Cancer 126: 692–702 10.1002/ijc.24803 [DOI] [PubMed] [Google Scholar]
- 49. Alamgir H, Koehoorn M, Ostry a, Tompa E, Demers P (2006) An evaluation of hospital discharge records as a tool for serious work related injury surveillance. Occup Environ Med 63: 290–296 10.1136/oem.2005.026047 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Tüchsen F, Andersen O, Olsen J (1996) Referral bias among health workers in studies using hospitalization as a proxy measure of the underlying incidence rate. J Clin Epidemiol 49: 791–794. [DOI] [PubMed] [Google Scholar]
- 51. McCallum AK, Manderbacka K, Arffman M, Leyland AH, Keskimäki I (2013) Socioeconomic differences in mortality amenable to health care among Finnish adults 1992–2003: 12 year follow up using individual level linked population register data. BMC Health Serv Res 13: 3 10.1186/1472-6963-13-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The authors confirm that, for approved reasons, some access restrictions apply to the data underlying the findings. Our study utilizes administrative record linkage and all data used in the present manuscript were obtained from third parties. Interested researchers need to obtain these data directly from them. Data on age and sex were obtained from the population database maintained by Statistics Finland and the dates of death were obtained from the National Death Register also kept by Statistics Finland. Hospitalization data were obtained from the Finnish Hospital Discharge Register that is maintained by the National Institute for Health and Welfare in Finland. Record linkage was conducted by Statistics Finland. Contact details for organizations that own the data: Data on hospitalizations: National Institute for Welfare and Health Arto Vuori, Development Manager THL Information Department arto.vuori@thl.fi tel. +358 29 524 7035. Other register data used in this study: Statistics Finland Registrar's Office Sanna Malinen, Statistician kirjaamo@stat.fi tel. +358 29 551 2564.