

Abstract
Rationale
Nonadherence to prescribed medications is a significant barrier to the successful treatment of psychiatric disorders in clinical practice. It has been argued that patient participation in shared decision making improves adherence to treatment plans.
Purpose
To assess to what extent treatment adherence of psychiatric patients is influenced by the concordance between their preferred participation and their actual participation in decision making.
Materials and methods
A total of 967 consecutive psychiatric outpatients completed the Control Preference Scale twice consecutively before consultation, one for their preferences of participation, and the other for the style they had usually experienced until then, and the eight-item self-report Morisky Medication Adherence Scale 8.
Results
Most psychiatric outpatients preferred a collaborative role in decision making. Congruence was achieved in only 50% of the patients, with most mismatch cases preferring more involvement than had been experienced. Self-reported adherence was significantly higher in those patients in whom there was concordance between their preferences and their experiences of participation in decision making, regardless of the type of participation preferred.
Conclusion
Congruence between patients’ preferences and actual experiences for level of participation in shared decision making is relevant for their adherence to treatment.
Keywords: treatment adherence, psychiatric outpatients, shared decision making
Introduction
The advances of psychopharmacology in the last 5 decades have allowed broader stabilization, functional recovery, better social and vocational reintegration, and more favorable outcomes for patients with psychiatric disorders.1,2 However, medications do not work if patients do not take them. Poor adherence to pharmacologic treatment of psychiatric disorders is a worldwide problem of striking magnitude that contributes to the gap in care between best care, defined as the optimal use of proven efficacious pharmacologic therapies in psychiatric disorders, and usual care, the actual level of efficacious care being provided to psychiatric patients.3,4 Of course, adherence to prescribed psychotropic medication is relevant provided that the diagnosis of the psychiatric disorders is well established and the indication for the prescription of the drug treatment is adequate. In these cases, treatment effectiveness, crucial in severe mental illness and limited in minor psychiatric disorders, is hampered by the lack of adherence to the prescribed regimen. Half of patients with major depression for whom antidepressants are prescribed will not be taking the drugs 3 months after the initiation of therapy.5–7 Rates of adherence among patients with schizophrenia are between 50% and 60%, and among those with bipolar affective disorder, the rates are as low as 35%.8–11
Adherence is defined as “the extent to which the patient’s behavior matches agreed recommendations from the prescriber”.12 Adherence describes patient behavior in the actual taking of medicines. This definition of adherence presumes that the patient has reached some agreement with the health care professional about the prescribed medicine.13
At present, there is still a clear need to identify determinants of nonadherence that could be addressed in interventions to facilitate optimal use of medicines in psychiatric care that allow for not only a positive patient outcome but also a prevention of relapse. Review of the literature on predictors of compliance with psychiatric treatment prescribed has shown the inconsistency of sociodemographic and clinical variables.14
Although nearly 2 decades have passed since Charles et al at McMaster University proposed the hypothesis that active patient participation in the shared treatment decision-making (SDM) process will result in a greater commitment and adherence to the selected treatment regimen than to a regimen selected by the physician alone,15,16 very few studies are available at present showing that SDM actually results in patient improvement in treatment adherence that include medication adherence as an outcome.17
The aim of this study was to evaluate the influence of the match between preferred and experienced participation in SDM on self-reported adherence to prescribed treatment in psychiatric outpatient care.
Materials and methods
Sample
From October 2013 to May 2014, 1,220 consecutive psychiatric outpatients seen in the Community Mental Health Services on Tenerife Island (Canary Islands, Spain) were invited to participate in a cross-sectional study; a total of 967 accepted. Patients were eligible for inclusion in the study if they were aged 18 years and over and were diagnosed by their psychiatrists using the International Classification of Diseases (ICD)-10 as F20 (schizophrenia), F31 (bipolar affective disorder), F32–33 (depressive disorder), F40–48 (anxiety disorder), and F60–69 (disorders of adult personality and behavior). Each participant received a full explanation of the study, after which they signed an informed consent document approved by the clinical research ethics committee of Nuestra Señora de Candelaria University Hospital in Santa Cruz de Tenerife. Each participant then filled out a brief sociodemographic survey and the remaining questionnaires.
Measures
Sociodemographic characteristics and clinical variables
Age, sex, educational level (no formal education, primary studies, secondary studies, and university degree), history as psychiatric patient (in years), and type of psychoactive drugs currently taken were assessed. For assessment purposes, the drugs were divided into the common groups of psychotropic drugs: antidepressants (tricyclics, selective serotonin-reuptake inhibitors [SSRIs] and serotonin–norepinephrine reuptake inhibitors [SNRIs]), benzodiazepines, antipsychotics (conventional and atypical), and mood stabilizers. For statistical analysis purposes, a new variable (number of different drugs) was drawn up as an indirect measure of treatment complexity. We also recorded how long patients had been under psychiatric treatment (in months), the number of different psychiatrists treating them during that time, and the number of psychiatric admissions specifying their voluntary or involuntary character. Patients’ diagnoses and treatments were collected from their therapeutic recommendation sheets.
Instruments
Medication adherence
Medication adherence was tested using the Spanish version of the validated eight-item self-report Morisky Medication Adherence Scale (MMAS-8).18 The questions are formulated to avoid a “yes-saying” bias, ie, the wording of item 5 is reversed to prevent the tendency to respond in a specific way to a series of questions regardless of their content. Response choices are yes/no for items 1 through 7, and a 5-point Likert response scale for the last item. Each no response is rated as 1 and each yes rated as 0, except for item 5, in which each yes response is rated as 1 and each no is rated as 0. For item 8, it is necessary to standardize the code (0–4), by dividing by four when calculating a summated score. The total score on the MMAS-8 can range from 0 to 8, with scores of 8 reflecting high adherence, 7 or 6 reflecting medium adherence, and <6 reflecting low adherence. Permission to use the scale was granted by Donald Morisky, the copyright holder of the instrument.
Control Preferences Scale
The Control Preferences Scale (CPS) was developed by Degner et al19 to evaluate the amount of control patients want to assume in the process of making decisions about the treatment of their diseases. There are two different formats of the scale: a questionnaire and a card-sorting version, which was used in our study. This consists of five cards on a board, each illustrating a different role in decision making by means of a cartoon and short descriptive statement. The examiner asks the respondent to choose the preferred card, which is then covered up and cannot be chosen again; the examiner then asks the respondent to choose the preferred card from the remaining four cards. The procedure continues (four choices) until one card is left. If the second preference is incongruent with the first (nonadjacent pairing, such as card A with card C), the test is explained again and immediately readministered. In the event of a further incongruence, the test is not readministered, and a preference is not assigned. Administration requires about 5 minutes. Six scores are possible based on the subject’s two most preferred roles: active–active, active–collaborative, collaborative–active, collaborative–passive, passive–collaborative, and passive–passive. These scores are grouped as active (active–active or active–collaborative), collaborative (collaborative–active or collaborative–passive), or passive (passive–collaborative or passive–passive). Evidence suggests that the CPS is clinically relevant, easily administered, and valid in health care decision making to assess preferences for participation.20 The scale was administered twice consecutively in the waiting room before the psychiatric consultation. The first administration asked patients about their preferred style of clinical decision making in their clinical encounters with their psychiatrists. The second administration asked them about the style they had usually experienced until then in their previous consultations with their psychiatrists.
Statistical analysis
Data were analyzed using SPSS 19.21 We calculated a categorical variable (congruence), to summarize the relationship between SDM preferred and experienced according to CPS results, with two categories: matched (SDM experienced same as preferred) and unmatched (SDM experienced differently than preferred). The χ2 was used to test for differences between groups.
Results
We recorded a high response rate of 79%, resulting in a sample of 967 psychiatric outpatients. Table 1 shows the sample distribution according to sociodemographic and clinical variables included in the study, as well as the preferred roles and experienced roles according to the CPS, and the MMAS-8 scores.
Table 1.
Sociodemographic and clinical characteristics of the sample studied (n=967)
| Variable | Category | Number of cases | Percentage of the sample |
|---|---|---|---|
| Age, years (mean 49.6±13.8, rank 18–87) | 18–30 | 99 | 10.2 |
| 30–45 | 262 | 27.1 | |
| 45–60 | 406 | 42.0 | |
| 60–75 | 169 | 17.5 | |
| >75 | 30 | 3.1 | |
| Sex | Male | 358 | 37.1 |
| Female | 608 | 62.9 | |
| Educational level | Can read and write | 88 | 9.1 |
| Primary | 334 | 34.5 | |
| Secondary | 359 | 37.1 | |
| University | 186 | 19.2 | |
| ICD-10 diagnosis | Schizophrenia | 179 | 18.5 |
| Bipolar disorder | 118 | 12.2 | |
| Depressive disorder | 462 | 47.8 | |
| Anxiety disorders | 160 | 16.5 | |
| Personality disorders | 30 | 3.1 | |
| Other diagnoses | 18 | 1.9 | |
| History of psychiatric admissions (59.6% involuntary) | No | 641 | 66.3 |
| 1 | 121 | 12.5 | |
| 2 | 68 | 7.0 | |
| 3 | 51 | 5.3 | |
| ≥4 | 86 | 8.9 | |
| Psychiatrists, n (mean 2.7±2.0, rank 1–15) | 1 | 323 | 33.4 |
| 2 | 259 | 26.8 | |
| 3 | 147 | 15.2 | |
| 4 | 79 | 8.2 | |
| ≥5 | 159 | 16.3 | |
| Psychotropic drugs (mean 2.9±1.4 drugs, rank 0–8, polypharmacy 86.2%) | No drugs | 21 | 2.2 |
| One drug | 128 | 13.2 | |
| Two drugs | 260 | 26.9 | |
| Three drugs | 246 | 25.4 | |
| Four drugs | 172 | 17.8 | |
| Five or more drugs | 140 | 14.5 | |
| Treatment | Antidepressants | 667 | 69.0 |
| Tricyclics | 33 | 3.4 | |
| SSRIs | 502 | 51.9 | |
| SNRIs | 340 | 35.2 | |
| Benzodiazepines | 763 | 79.0 | |
| Antipsychotics | 327 | 33.8 | |
| Conventional | 48 | 5.0 | |
| Atypical | 315 | 32.6 | |
| Mood stabilizers | 275 | 28.4 | |
| Anticholinergics | 43 | 4.4 | |
| MMAS-8, (mean 6.3±1.6, rank 0.5–8) | Low adherence (<6) | 269 | 28.3 |
| Medium adherence (6–<8) | 444 | 46.8 | |
| High adherence (= 8) | 236 | 24.9 | |
| CPS, preferred role | |||
| Active | Active–active | 11 | 1.1 |
| Active–collaborative | 54 | 5.6 | |
| Collaborative | Collaborative–active | 23 | 2.4 |
| Collaborative–passive | 602 | 62.3 | |
| Passive | Passive–collaborative | 246 | 25.4 |
| Passive–passive | 31 | 3.2 | |
| CPS, experienced role | |||
| Active | Active–active | 0 | 0.0 |
| Active–collaborative | 3 | 0.3 | |
| Collaborative | Collaborative–active | 4 | 0.4 |
| Collaborative–passive | 208 | 21.5 | |
| Passive | Passive–collaborative | 487 | 50.4 |
| Passive–passive | 265 | 27.4 | |
Abbreviations: ICD, International Classification of Diseases; SNRIs, serotonin–norepinephrine reuptake inhibitors; SSRIs, selective serotonin-reuptake inhibitors; CPS, Control Preference Scale; MMAS-8, eight-item self-report Morisky Medication Adherence Scale.
Nearly half of the psychiatric outpatients self-reported a medium level of adherence to their psychiatric drugs prescribed, while around a quarter of them self-reported either a high or a low adherence. Most psychiatric outpatients (625 patients, 64.7%) preferred shared decisional control, while 277 (28.6%) preferred a passive approach and only 65 (6.7%) an active decisional control. The most common preferred role was for the doctor and patient sharing responsibility for deciding what treatment is best (62.3%). The experienced roles self-reported according to the CPS were mostly passive (772 patients, 77.8%), followed by a collaborative approach (212 patients, 21.9%), with only three patients (0.3%) self-reporting active decisional control. The most common experienced role was for the doctor to make the final decision after considering the patient’s opinion (50.4%). Congruence between patients’ preferred and experienced involvement in medical decision making was achieved in half of the psychiatric outpatients participating in the study. In cases of mismatch, the vast majority of patients preferred more involvement than they experienced.
In Table 2 are represented the distribution of the three levels of adherence to treatment according to participation preferences and experiences and also to congruence between patients’ preferred and perceived participation. Patients who preferred a passive role in decision making were significantly more likely to self-report adherence to their psychiatric treatment than patients who preferred a more active role. Concerning the role experienced in their psychiatric consultations, self-reported adherence was higher in patients experiencing more active roles, but the differences registered were of no significance (Figure 1). Self-reported adherence was significantly higher in those patients for whom preferences and experiences of participation in decision making matched than in those patients where they did not match. According to the specific type of matching (active with active, collaborative with collaborative, and passive with passive), no differences were found in self-reported adherence.
Table 2.
Distribution of preferred and experienced participation, the congruence between both roles, and the relationship with adherence to treatment
| n | % | χ2 | P | High adherence | Medium adherence | Low adherence | χ2 | P | |
|---|---|---|---|---|---|---|---|---|---|
| Preferred role | |||||||||
| Active | 64 | 6.7 | 20.3% | 40.6% | 39.1% | ||||
| Collaborative | 610 | 64.3 | 496.02 | 0.000 | 24.1% | 45.6% | 30.3% | 11.28 | 0.024 |
| Passive | 275 | 29 | 27.6% | 50.9% | 21.5% | ||||
| Experienced role | |||||||||
| Active | 3 | 0.3 | 33.3% | 66.7% | 0 | ||||
| Collaborative | 205 | 21.6 | 926.87 | 0.000 | 26.3% | 46.8% | 26.8% | 1.67 | 0.796 |
| Passive | 741 | 78.1 | 24.4% | 46.7% | 28.9% | ||||
| Congruence | |||||||||
| Matched | 486 | 50.3 | 0.03 | 0.872 | 27.5% | 49.1% | 23.5% | 11.66 | 0.003 |
| Unmatched | 481 | 49.7 | 22.2% | 44.5% | 33.3% | ||||
| Congruence | |||||||||
| Active–active | 3 | 0.6 | 33.3% | 66.7% | 0 | ||||
| Collab–collab | 208 | 42.8 | 247.94 | 0.000 | 27.8% | 50.9% | 21.2% | 3.04 | 0.550 |
| Passive–Passive | 275 | 56.6 | 27.5% | 49.1% | 23.5% | ||||
Abbreviation: Collab, collaborative.
Figure 1.
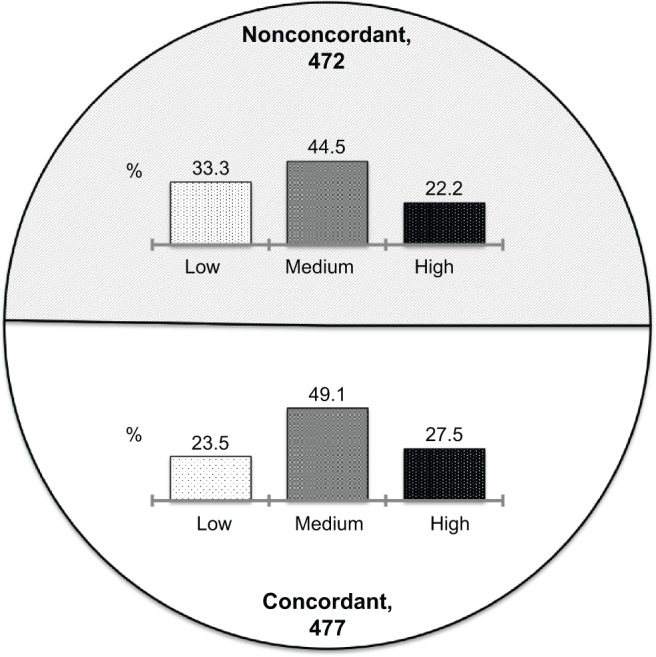
Eight-item self-report Morisky Medication Adherence Scale levels of adherence according to concordance between preferred and experienced participation in decision making.
Discussion
This is the first large, community psychiatry-based survey to explore to what extent the treatment adherence of psychiatric patients is influenced by the concordance between their preferred participation and their actual participation in decision making.
Some limitations of this study should be considered. First and foremost, our research did not study patient consultations directly, but only registered patients’ perceptions of decision-making styles. Second, since a cross-sectional survey was carried out, the study could only demonstrate associations and not causality. Another limitation is that preferences for decision making were measured as a state trait, and role preferences are dynamic and could vary during decision making, requiring regular clinical assessment to meet patients’ expectations. Also, we measured a general role in a general process of decision making, but patients can prefer different roles according to the different stages in the decision-making process that the CPS does not allow. Finally, given the explorative nature of the study carried out, our results should be interpreted with caution, and more research is required to replicate and evaluate the relevance of our findings.
In a previous paper,22 we reported a low level of concordance between patient preferences in clinical decision making and their actual experience, with more than half of the patients wanting a more active role than they had actually experienced. A logical conclusion of this and other studies17,23–25 would be that increased patient participation in clinical decision making could increase patient adherence to treatment. Our present study shows that psychiatric outpatients whose preferences of participation in clinical decision making were matched by their actual experience were significantly more likely to adhere to the drugs prescribed than patients who experienced a different level of participation than desired. As the greater source of mismatch is the preference of the patient for a more active role than the one actually experienced, it makes sense that the widespread opinion in the literature is that increasing the participation of psychiatric patients in SDM would increase their treatment adherence. However, according to our results, the concordance between the patient’s preferred level of participation and their actual participation seems to be more relevant for treatment adherence than the mere fact of being involved in the clinical decision-making process. Observational studies in medical patients suggest that failure to elicit and address patients’ individual circumstances and goals/preferences regarding their treatment regimen may contribute to treatment nonadherence.26 Likewise, a recent review on the congruence between patients’ preferred and perceived participation in medical decision making concluded that a similar approach to all patients is not likely to meet patients’ wishes, since preferences for participation vary among patients.21 As sanctioned by the age-old wisdom of Hippocrates, trust in the doctor and satisfaction with the doctor–patient relationship may well be the most accurate predictor of treatment adherence. Concordance between patient preferences and experiences in clinical decision making is likely to increase the satisfaction in the relationship and the confidence in the doctor. On the contrary, a lack of concordance may exacerbate psychological reactance in psychiatric patients, an aversive motivational state known to influence in a negative way the involvement of patients in health behaviors, treatment adherence, and relapse.26–29 Further studies about congruence and mismatch between doctor and patient attitudes in medical decision making are relevant for practice. A lack of sensitivity to this issue may result in suboptimal care and serve as a barrier to patient-centered care. In the context of psychiatric outpatient care, better adherence to the prescribed treatment may be achieved if psychiatrists ascertain their patients’ preferred role and minimize the dissonance between what they want and what they receive concerning clinical decision making.
In conclusion, mental health care professionals should be sensitive to patients’ individual preferences and participation wishes, and respond to those without trying to impose a preconceived attitude. This is the hallmark of personalized psychiatry.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Lebowitz BD, Rudorfer MV. Treatment research at the millennium: from efficacy to effectiveness. J Clin Psychopharmacol. 1998;18:1. doi: 10.1097/00004714-199802000-00001. [DOI] [PubMed] [Google Scholar]
- 2.Kane J. Progress defined – short-term efficacy, long-term effectiveness. Int Clin Psychopharmacol. 2001;16(Suppl 1):S1–S8. doi: 10.1097/00004850-200101001-00002. [DOI] [PubMed] [Google Scholar]
- 3.Sabaté E. Adherence to Long-Term Therapies: Evidence for Action. Geneva: World Health Organization; 2003. [Google Scholar]
- 4.De las Cuevas C. Towards a clarification of terminology in medicine-taking behavior: compliance, adherence and concordance are related although different terms with different uses. Curr Clin Pharmacol. 2011;6:74–77. doi: 10.2174/157488411796151110. [DOI] [PubMed] [Google Scholar]
- 5.Vergouwen AC, van Hout HP, Bakker A. Methods to improve patient compliance in the use of antidepressants. Ned Tijdschr Geneeskd. 2002;146:204–207. Dutch. [PubMed] [Google Scholar]
- 6.Julius RJ, Novitsky MA, Jr, Dubin WR. Medication adherence: a review of the literature and implications for clinical practice. J Psychiatr Pract. 2009;15:34–44. doi: 10.1097/01.pra.0000344917.43780.77. [DOI] [PubMed] [Google Scholar]
- 7.Roca M, Armengol S, Salvador-Carulla L, Monzón S, Salvà J, Gili M. Adherence to medication in depressive patients. J Clin Psychopharmacol. 2011;31:541–543. doi: 10.1097/JCP.0b013e3182223af9. [DOI] [PubMed] [Google Scholar]
- 8.Colom F, Vieta E, Martínez-Arán A, Reinares M, Benabarre A, Gastó C. Clinical factors associated with treatment noncompliance in euthymic bipolar patients. J Clin Psychiatry. 2000;61:549–555. doi: 10.4088/jcp.v61n0802. [DOI] [PubMed] [Google Scholar]
- 9.Lacro JP, Dunn LB, Dolder CR, Leckband SG, Jeste DV. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63:892–909. doi: 10.4088/jcp.v63n1007. [DOI] [PubMed] [Google Scholar]
- 10.Perkins DO. Predictors of noncompliance in patients with schizophrenia. J Clin Psychiatry. 2002;63:1121–1128. doi: 10.4088/jcp.v63n1206. [DOI] [PubMed] [Google Scholar]
- 11.Velligan DI, Weiden PJ, Sajatovic M, et al. The expert consensus guideline series: adherence problems in patients with serious and persistent mental illness. J Clin Psychiatry. 2009;70(Suppl 4):1–46. [PubMed] [Google Scholar]
- 12.Horne R, Weinman J, Barber N, Elliott R, Morgan M. Concordance, Adherence and Compliance in Medicine-Taking: Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R &D. Southampton: National Institute for Health Research; 2005. [Google Scholar]
- 13.Nunes V, Neilson J, O’Flynn N, et al. Clinical Guidelines and Evidence Review for Medicines Adherence: Involving Patients in Decisions about Prescribed Medicines and Supporting Adherence. London: National Collaborating Centre for Primary Care and Royal College of General Practitioners; 2009. [PubMed] [Google Scholar]
- 14.Rivero-Santana A, Perestelo-Perez L, Peŕez-Ramos J, Serrano-Aguilar P, De Las Cuevas C. Sociodemographic and clinical predictors of compliance with antidepressants for depressive disorders: systematic review of observational studies. Patient Prefer Adherence. 2013;7:151–169. doi: 10.2147/PPA.S39382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Charles C, Gafni A, Whelen T. Decision-making in the physician-patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med. 1999;49:651–661. doi: 10.1016/s0277-9536(99)00145-8. [DOI] [PubMed] [Google Scholar]
- 16.Charles C, Gafni A, Whelen T. Shared decision-making in the medical encounter: what does it mean? (Or it takes at least two to tango) Soc Sci Med. 1997;44:681–692. doi: 10.1016/s0277-9536(96)00221-3. [DOI] [PubMed] [Google Scholar]
- 17.Joosten EA, DeFuentes-Merillas L, de Weert GH, Sensky T, van der Staak CP, de Jong CA. Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence, and health status. Psychother Psychosom. 2008;77:219–226. doi: 10.1159/000126073. [DOI] [PubMed] [Google Scholar]
- 18.Morisky DE, Ang A, Krousel-Wood M, Ward H. Predictive validity of a medication adherence measure for hypertension control. J Clin Hypertens. 2008;10:348–354. doi: 10.1111/j.1751-7176.2008.07572.x. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 19.Degner LF, Sloan JA, Venkatesh P. The Control Preferences Scale. Can J Nurs Res. 1997;29:21–43. [PubMed] [Google Scholar]
- 20.Brom L, Hopmans W, Pasman HR, Timmermans DR, Widdershoven GA, Onwuteaka-Philipsen BD. Congruence between patients’ preferred and perceived participation in medical decision-making: a review of the literature. BMC Med Inform Decis Mak. 2014;14:25. doi: 10.1186/1472-6947-14-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.International Business Machines. IBM SPSS Statistics for Windows. Version 19.0. Armonk (NY): IBM; 2010. [Google Scholar]
- 22.De las Cuevas C, Peñate W, de Rivera L. Psychiatric patients preferences and experiences in clinical decision making: examining concordance and correlates of patient’s preferences. Patient Educ Couns. 2014;96:222–228. doi: 10.1016/j.pec.2014.05.009. [DOI] [PubMed] [Google Scholar]
- 23.Goss C, Moretti F, Mazzi MA, Del Piccolo L, Rimondini M, Zimmermann C. Involving patients in decisions during psychiatric consultations. Br J Psychiatry. 2008;193:416–421. doi: 10.1192/bjp.bp.107.048728. [DOI] [PubMed] [Google Scholar]
- 24.Hamann J, Cohen R, Leucht S, Busch R, Kissling W. Do patients with schizophrenia wish to be involved in decisions about their medical treatment? Am J Psychiatry. 2005;162:2382–2384. doi: 10.1176/appi.ajp.162.12.2382. [DOI] [PubMed] [Google Scholar]
- 25.Osterberg L, Blaschke T. Adherence to medication. N Engl J Med. 2005;353:487–497. doi: 10.1056/NEJMra050100. [DOI] [PubMed] [Google Scholar]
- 26.Moore A, Sellwood W, Stirling J. Compliance and psychological reactance in schizophrenia. Br J Clin Psychol. 2000;39:287–295. doi: 10.1348/014466500163293. [DOI] [PubMed] [Google Scholar]
- 27.Fogarty J, Youngs GA. Psychological reactance as a factor in patient noncompliance with medication taking: a field experiment. J Appl Soc Psychol. 2000;30:2365–2391. [Google Scholar]
- 28.De las Cuevas C, Peñate W, Betancort M, De Rivera L. Psychological reactance in psychiatric patients: examining the dimensionality and correlates of the Hong Psychological Reactance Scale in a large clinical sample. Pers Individ Diff. 2014;70:85–91. [Google Scholar]
- 29.De las Cuevas C, Peñate W, Sanz EJ. Risk factors for non-adherence to antidepressant treatment in patients with mood disorders. Eur J Clin Pharmacol. 2014;70:89–98. doi: 10.1007/s00228-013-1582-9. [DOI] [PubMed] [Google Scholar]