

Introduction
The incidence of malignancy occurring in pregnancy is approximately 0.7–0.1 % [1]. Sarcomas occurring during pregnancy are even rarer, and kidney is an unusual site for a synovial sarcoma (SS). The histogenesis of this tumor is unknown and is usually characterized by the specific translocation t(X; 18) (p 11.2; q 11) resulting in fusion of SYT gene on chromosome 18 with SSX gene on chromososme X. SSs in general have an aggressive clinical course. Their occurrence during pregnancy poses a challenge in management.
Case Report
We report a rare case of a monophasic primary synovial sarcomas (PSS) of kidney in a 25-year-old female who presented with abdominal distension, pain in the left flank, hematuria for 10 months, and amenorrhea for 2 months. A 10 × 10 cms left flank mass was palpated. USG abdomen showed an 8-week-old gestational sac with a healthy embryo. The CT and MRI findings were consistent with the clinical diagnosis of renal cell carcinoma, with no evidence of metastasis. A medical termination of pregnancy (MTP) was performed at 8 weeks of gestation as the patient had two living issues as well as economic constraints. Four days later, a left radical nephrectomy followed the MTP. She was later referred to an oncology institute for chemotherapy. No metastasis or recurrence was noted at 6 months of follow up (Fig. 1).
Fig. 1.
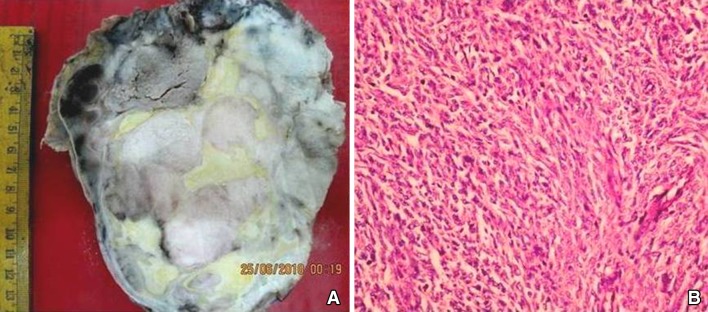
A Nephrectomy specimen with an encapsulated and variegated, renal tumor with areas of hemorrhage and necrosis. B Spindle cell sarcoma composed of fascicles of mildly pleomorphic plump spindle cells (H&E, ×100)
The nephrectomy specimen showed an encapsulated renal tumor measuring 15 × 11 × 10 cms with large areas of hemorrhage and necrosis. Hilar structures and left adrenal gland were free. No other tumor was found anywhere in the body.
Histopathological examination showed a malignant spindle cell neoplasm with tumor cells arranged in sheets, fascicles and whorls. Individual tumor cells were monomorphic, plump, spindle shaped, with mildly pleomorphic nuclei. Frequent mitoses and necrosis were seen. A diagnosis of PSS of kidney of monophasic type was considered along with other differentials of sarcomas.
On extensive immunohistochemistry, tumor cells were positive for bcl 2, Mic 2, and vimentin. Other markers for spindle cell malignancies were negative.
RT-PCR results, performed twice, using RNA extracted from paraffin embedded tissue blocks for fusion transcript SYT-SSX 1 were negative.
Classical histomorphology and extensive IHC work-up established the diagnosis as monophasic PSS of kidney.
Discussion
To the best of our knowledge, there is a single reported case of SS of kidney of size greater than 5 cm, occurring in pregnancy (at 32 weeks of gestation). The patient had an elective cesarean section and a tumor nephrectomy and delivered a healthy male baby. She received combined radiotherapy and chemotherapy 4 weeks later [2].
Controversy exists regarding the effect of pregnancy on the growth rate of high grade sarcomas. Some sarcomas grow rapidly during pregnancy, while some do not. The effect chemotherapy has on pregnancy depends on the trimester of pregnancy. Chemotherapy in first trimester is contraindicated, while in the second and third trimesters, it is controversial because of the possible long-term effects on the fetus [2].
The management of aggressive sarcomas in pregnancy is challenging, and treatment needs to be individualized. However, only limited data is available.
References
- 1.Orlandi E, Zonca G, Pignoli E, et al. Postoperative radiotherapy for synovial sarcoma of the head and neck during pregnancy: clinical and technical management and fetal dose estimates. Tumori. 2007;93(1):45–52. doi: 10.1177/030089160709300109. [DOI] [PubMed] [Google Scholar]
- 2.Bettendorf O, Bierer S, Köhler G, et al. Neoplasia of the kidney–a rare event during pregnancy: part 2. Eur Urol. 2006;50(2):375–376. doi: 10.1016/j.eururo.2006.02.029. [DOI] [PubMed] [Google Scholar]