

Introduction
Parasitic myomas are those that have become partially or almost completely separated from the uterus and receive their main blood-supply from another source. The etiopathogenesis of parasitic myomas may be separation of peduncululated subserosal myomas that have outgrown their blood supply. More commonly, iatrogenic parasitic myomas may be caused by seeding of myoma fragments following morcellation during hysterectomy or myomectomy [1].
Case Report
A patient, aged 48 years, presented with complaints of menorrhagia for past 2 years. She had tried medical management without any relief. On examination, she was found to have uterus enlarged to 26 week's size. Ultrasonography showed posterior wall fibroid 14 × 11 cm. She underwent total laparoscopic hysterectomy with abdominal electromechanical morcellation through left lateral port using ROTOCUT G1 morcellator. She presented 3 months later with complaints of pain and mass in left lower abdomen. On examination, a hard mass was palpable, 6 × 5 cm in left iliac fossa and tender. Ultrasonography showed thick-walled mass-like lesion with surrounding inflammatory changes in the left side of pelvis with probable diagnosis of tubo-ovarian mass or infective hematoma. Patient was given antibiotic and analgesics for 5 days, but symptoms were not relieved. Patient was posted for diagnostic laparoscopy. On laparoscopy, omental adhesions were found to be present to the previous left port site on anterior abdominal wall. The mass was seen as an extraperitoneal bulge over left iliac region just above the inguinal ligament. Decision for laparotomy was taken. A 6-cm oblique incision was taken over the left iliac fossa, and the area was explored. A hard fibro muscular mass was seen involving left side oblique abdominal muscles (Fig. 1). Deep dissection was done, and mass was excised piecemeal. Degenerated caseous material was aspirated out from deep musculature. Hemostasis was ensured, and patient received one unit of blood postoperatively. In spite of thromboprophylaxis, patient developed gradual swelling in left leg on 3rd postoperative day. Color Doppler of left lower limb showed deep venous thrombosis extending to popliteal, femoral, and external iliac veins with diffuse severe stenosis of left external iliac artery. Vascular surgeon was consulted, and contrast magnetic resonance angiogram of abdominal aorta and lower limbs was done. It showed total occlusion of left external iliac and common femoral artery with reformation of distal common femoral artery on left side. Left side popliteal and leg arteries appeared normal. Patient was managed conservatively with low molecular weight heparin, low dose aspirin, warfarin, and vasodilator. Patient was followed up after 3 and 6 months; there was no muscular weakness in the left leg, and she could perform all routine activities and is now leading a normal life.
Fig. 1.
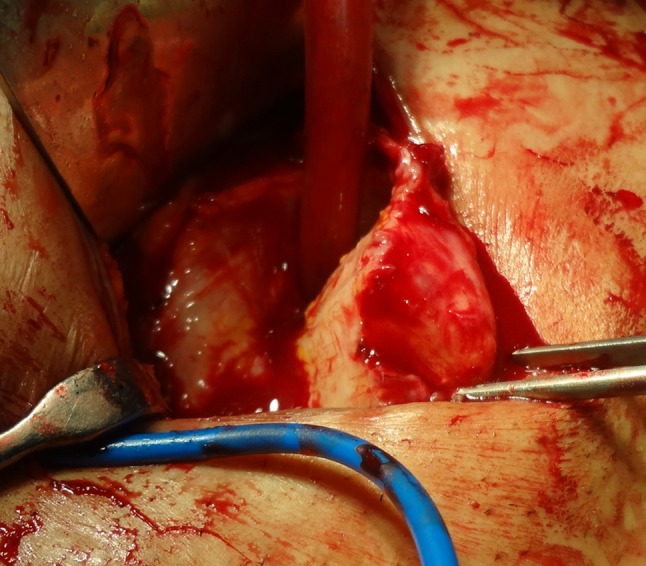
Operative photograph showing excision of parasitic fibroid
Discussion
Parasitic fibroids are defined as benign smooth-muscle tumors which have become separated from the uterus. The etiopathogenesis of parasitic myomas is not understood clearly; they are believed to originate from a pedunculated subserosal fibroid that twists and separates from its uterine attachment. Once it is free in the peritoneal cavity, it can attach to adjacent structures and receive its blood supply from the peritoneum. .
Electromechanical morcellation during laparoscopic hysterectomy and myomectomy can remove large specimens, but with risk of incomplete removal. A few recent case reports and small series [2–4] have found association of parasitic myomas with history of previous laparoscopic surgeries with morcellation, which suggests an iatrogenic mechanism for parasitic myoma. These iatrogenic myomas arise from fragments inadvertently left behind in the peritoneal cavity previous morcellation procedure [5]
Parasitic fibroids are rare complication of fibroids and with the increase of electromechanical morcellation during laparoscopic myomectomy and hysterectomy the incidence is likely to increase [5]. In the review of cases, parasitic fibroids have been described in the peritoneal cavity usually, but in this case, the fibroid was located in the anterior abdominal wall at the site of morcellation. Postoperatively, patient developed arterial stenosis. Imaging showed collaterals in the popliteal circulation 1 week postoperatively suggesting chronic obstruction in the arterial supply due to compression by the mass (Fig. 2). Probably, the cause of post operative deep vein thrombosis was intimal injury during deep dissection.
Fig. 2.
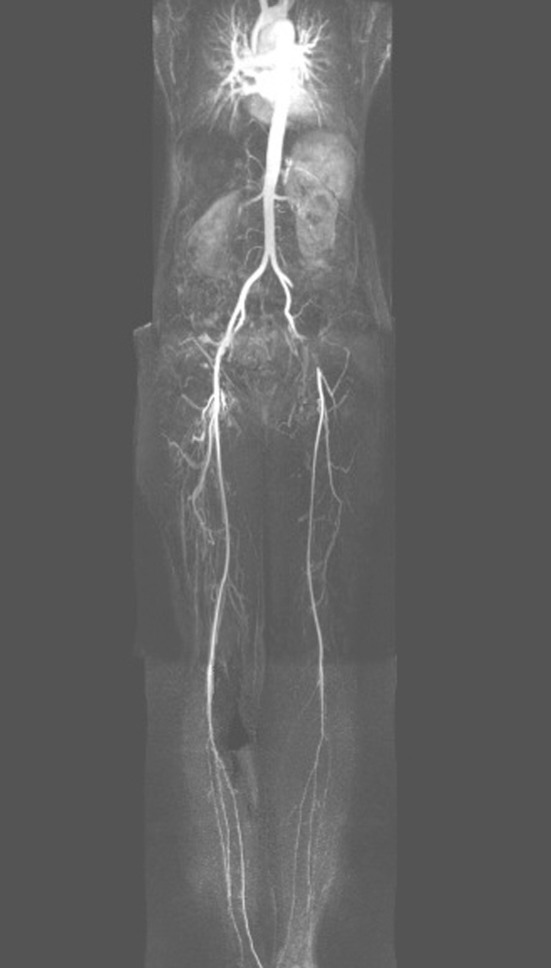
MR angiogram showing stenosis of left external iliac artery
Larraín et al. [6] in a study on iatrogenic fibroids, discussed important points to be considered while doing laparoscopic morcellation. In all patients who are at risk of uterine malignancy, endometrial biopsy and cervical cytology should be performed preoperatively to reduce the possible spread after unsuspected morcellation of a malignant tumor. At the time of the morcellation procedure, every effort should be made to remove all tissue fragments, and irrigation should be used judiciously to reduce spread of fragments to upper abdominal cavity. In cases of smaller surgical specimens, it is a good practice to morcellate inside an endoscopic bag. Small fragments of the myoma should be removed as soon as they are formed [7]. Thorough inspection along with repeated suction and irrigation should be done at the end of the surgery. In case of removal of multiple myomas, proper counting of fibroids should be done at the time of enucleation and then at tissue retrieval. The clinical significance is that in patients with symptoms or findings, suggesting new or recurrent pelvic mass with history of previous morcellation, iatrogenic parasitic myomas should be considered in the differential diagnosis.
References
- 1.Cucinella G, Granese R, Calagna G, Somigliana E, Perino A. Parasitic myomas after laparoscopic surgery: an emerging complication in the use of morcellator? Description of four cases. Fertil Steril. 2011;96:e90–e96. doi: 10.1016/j.fertnstert.2011.05.095. [DOI] [PubMed] [Google Scholar]
- 2.LaCoursiere DY, Kennedy J, Hoffman CP. Retained fragments after total laparoscopic hysterectomy. J Minim Invasive Gynecol. 2005;12:67–69. doi: 10.1016/j.jmig.2004.12.021. [DOI] [PubMed] [Google Scholar]
- 3.Takeda A, Mori M, Sakai K, et al. Parasitic peritoneal leiomyomatosis diagnosed 6 years after laparoscopic myomectomy with electrical tissue morcellation: report of a case and review of the literature. J Minim Invasive Gynecol. 2007;14:770–775. doi: 10.1016/j.jmig.2007.07.004. [DOI] [PubMed] [Google Scholar]
- 4.Sinha R, Sundaram M, Mahajan C, et al. Multiple leiomyomas after laparoscopic hysterectomy: report of two cases. J Minim Invasive Gynecol. 2007;14:123–127. doi: 10.1016/j.jmig.2006.08.002. [DOI] [PubMed] [Google Scholar]
- 5.Kho KA, Nezhat C. Parasitic myomas. Obstet Gynecol. 2009;114:611–615. doi: 10.1097/AOG.0b013e3181b2b09a. [DOI] [PubMed] [Google Scholar]
- 6.Larraín D, Rabischong B, Khoo CK, Botchorishvili R, Canis M, Mage G. Iatrogenic parasitic myomas: unusual late complication of laparoscopic morcellation procedures. J Minim Invasive Gynecol. 2010;17:719–724. doi: 10.1016/j.jmig.2010.05.013. [DOI] [PubMed] [Google Scholar]
- 7.Aust T, Gale P, Cario G, Robertson G. Bowel resection for iatrogenic parasitic fibroids with preoperative investigations suggestive of malignancy. Fertil Steril. 2011;96:e1. doi: 10.1016/j.fertnstert.2011.04.097. [DOI] [PubMed] [Google Scholar]