

Abstract
A 48-year-old man, a known case of Friedreich's ataxia (FRDA) underwent cardiac fluorodeoxyglucose (FDG) positron emission tomography -computed tomography (PET/CT) for evaluation of myocardial viability. Tetrofosmin images showed an enlarged left ventricular cavity with small mid and basal inferior and apical infarct global hypokinesia with ejection fraction of 39%. Fluorodeoxyglucose images showed poor quality myocardial images. Friedreich's ataxia is associated with a high incidence of diabetes mellitus. Non-diabetic patients with Friedreich's ataxia have insulin resistance. This is associated with a reduction in the affinity of insulin receptors and membrane abnormality that alters the binding function of the insulin receptor.
Keywords: Cardiac positron emission tomography-computed tomography scan, Friedreich's ataxia, insulin resistance, poor cardiac fluorodeoxyglucose uptake
INTRODUCTION
Positron emission tomography (PET) is a noninvasive medical imaging modality that produces functional rather than anatomical images, thereby providing greater insight to the patient's condition. Assessment of metabolism by PET provides the sensitive detection of tissue viability based on the integrity of cardiac substrate metabolism.
CASE REPORT
A 48-year-old male, a known case of Friedreich's ataxia (FRDA) complained of swelling of lower extremities and low ejection fraction on echocardiography (ECHO). His risk factors were hypertension, obesity, and dyslipidemia. He had a past history of non ST elevation myocardial infarction 6 years ago. His two-dimensional-ECHO showed an ejection fraction of 15%, dilated left atria and ventricle. Left ventricular apex, distal septum and inferior wall were severely hypokinetic. Patient was advised a cardiac PET scan for evaluation of myocardial viability.
Initially, patient was injected with 10 mCi tetrofosmin. After waiting for 45 min rest tetrofosmin images were acquired. Patient was 6 h fasting with a baseline sugar: 128 mg/dl. Fifty milligram oral glucose load was given, and 1 h later blood sugar was 198 mg/dl.[1] Two units IV insulin (actrapid) was administered; however, the blood sugar after ½ h was 230 mg/dl. On rechecking blood sugar again after ½ h increased to 249 mg/dl. Patient was then administered six units of IV insulin. One hour later, sugar level reduced to 123 mg/dl after which fluorodeoxyglucose (FDG) was injected.
Tetrofosmin images [Figure 1] showed an enlarged left ventricular cavity with moderate perfusion defect in the apex, apical anterior, apical inferior wall of myocardium. Severe perfusion defect was observed in mid and basal inferior wall of myocardium. Septal uptake was more than lateral wall, suggestive of left ventricular hypertrophy. Gated images showed global hypokinesia with akinetic mid and basal inferior wall, ejection fraction of 39%. FDG images [Figure 2] were acquired 1 h, 2 h, and 3 h later. All images showed poor quality myocardial uptake.
Figure 1.
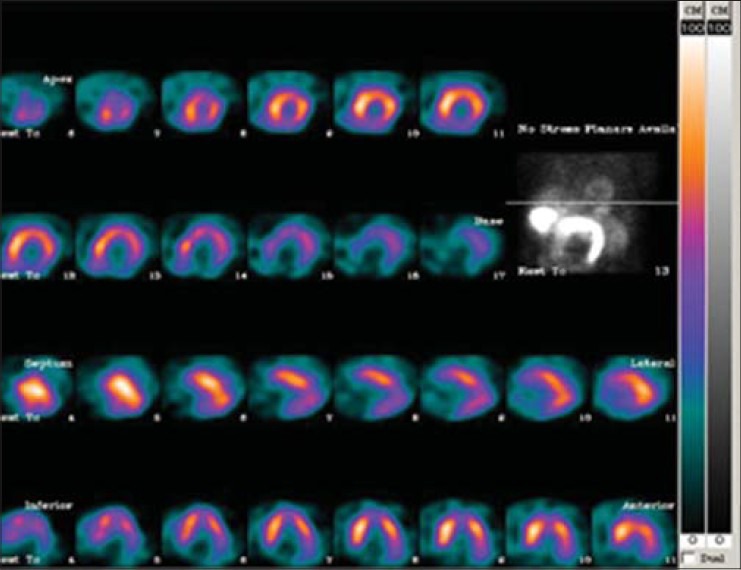
Tetrofosmin images showed perfusion defect
Figure 2.
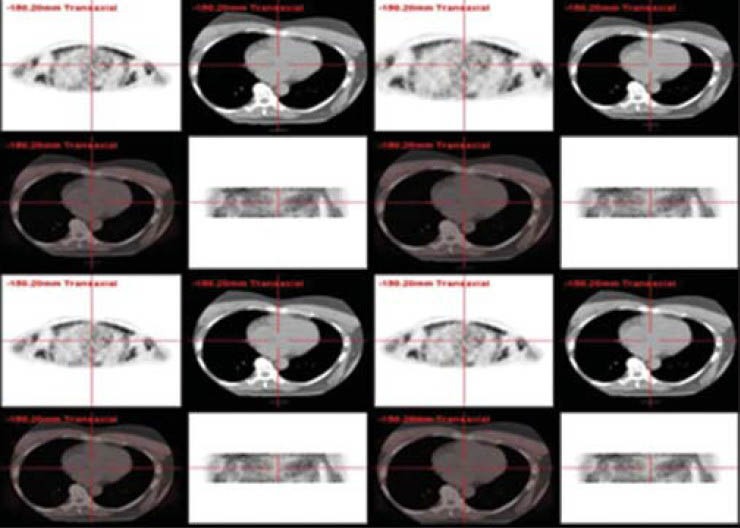
Images acquired at the interval of 1 h, 2 h, and 3 h post fluorodeoxyglucose administration show a similar picture of poor FDG uptake
DISCUSSION
Friedreich's ataxia is an inherited (genetic), progressive disorder of the nervous system that affects balance, coordination, movement, and sensation. FRDA affects approximately two out of every 100,000 people. The first symptoms of FRDA usually occur before age 20, but occasionally, onset can be as late as the 50s. The disorder is “recessive” (when both parents are FRDA carriers, they have a one-in-four chance in each pregnancy of conceiving a child who will develop the disease).
Males and females are equally affected FRDA, due to defects in a gene on chromosome 9 that carries the “recipe”, or “code”, for a cellular protein known as frataxin. The defects keep the affected cells from making a normal amount of frataxin. Without frataxin, iron builds up in the mitochondria and damages them. The resulting cellular “energy shortage” can kill the cell. Thus, nervous system degenerates over time. The cells most affected are those that transmit sensory and movement signals through long fibers.
Cells in the heart and pancreas are also affected in this disorder. FRDA is associated with a high incidence of diabetes mellitus. Nondiabetic patients with FRDA have insulin resistance.[2,3] Preliminary studies of insulin binding to erythrocytes suggest a difference in the binding characteristics among diabetic FRDA patients, while the binding in the nondiabetic FRDA group is similar to that of nondiabetic controls.[4] In most viability studies, the normal myocardium under glucose load and insulin stimulation shows good FDG uptake. Under normal conditions, most of the energy needs of the heart are met through fatty acid metabolism. However, areas of ischemia switch preferentially to glucose metabolism and have increased FDG uptake relative to perfusion. Cardiac glucose utilization is increased by Glucose administration which stimulates insulin secretion. The increased insulin level stimulates glucose metabolism. Thus, high serum glucose and insulin levels and low free fatty acid level promote FDG uptake. Our patient had only a small mid and basal inferior and apical infarct. The rest of the normal myocardium also did not surprisingly show any FDG uptake despite of repeated delayed images up to 3 h postFDG administration as insulin resistance is associated with a reduction in the affinity of insulin receptors and membrane abnormality that alters the binding function of the insulin receptor.
Although there is no known cure for FRDA, many of the problems imposed by the disease can be treated. Orthopedic intervention, which may include surgery, can alleviate scoliosis, and orthopedic appliances and physical therapy can help prolong ambulation. Heart problems can also be successfully treated for many years with medication. Insulin therapy is effective in controlling diabetes mellitus.
CONCLUSION
Even nondiabetic patients suffering from other diseases with insulin resistance due reduction in affinity of insulin receptors or membrane abnormality could surprise us as in our case.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Gerber BL, Ordoubadi FF, Wijns W, Vanoverschelde JL, Knuuti MJ, Janier M, et al. Positron emission tomography using (18)F fluorodeoxyglucose and euglycaemic hyperinsulinaemic glucose clamp: Optimal criteria for the prediction of recovery post ischemic left ventricular dysfunction. Results from the European Community Concerted Action multicenter study on use of (18)F-fluorodeoxyglucose positron emission tomography for the detection of myocardial viability. Eur Heart J. 2001;22:1691–701. doi: 10.1053/euhj.2000.2585. [DOI] [PubMed] [Google Scholar]
- 2.Khan RJ, Andermann E, Fantus IG. Glucose intolerance in Friedreich's ataxia: Association with insulin resistance and decreased insulin binding. Metabolism. 1986;35:1017–23. doi: 10.1016/0026-0495(86)90037-5. [DOI] [PubMed] [Google Scholar]
- 3.Fantus IG, Janjua N, Senni H, Andermann E. Glucose intolerance in first-degree relatives of patients with Friedreich's ataxia is associated with insulin resistance: Evidence for a closely linked inherited trait. Metabolism. 1991;40:788–93. doi: 10.1016/0026-0495(91)90004-g. [DOI] [PubMed] [Google Scholar]
- 4.Draper P, Shapcott D, Larose A, Stankova J, Levesque F, Lemieux B. Glucose tolerance and erythrocyte insulin receptors in Friedreich's ataxia. Can J Neurol Sci. 1979;6:233–9. doi: 10.1017/s0317167100119705. [DOI] [PubMed] [Google Scholar]